You must be signed in to read the rest of this article.
Registration on CDEWorld is free. Sign up today!
Forgot your password? Click Here!
Introduction
Head and neck cancers, including oropharyngeal cancers (OPC), are the sixth most common cancer type worldwide; over the last decade and the human papillomavirus (HPV) has been linked to an estimated 70% of all oropharyngeal malignancies.1,2,3 The human papillomavirus is a group of more than 200 related viruses.4 Twelve types are considered high-risk as they manifest carcinogenicity in humans.4 One in four people in the United States (US) become infected with HPV annually through skin-to-skin, vaginal, anal or oral contact with an infected person.4 While no signs or symptoms may be present at the time of infection, a malignancy may develop years after the initial infection.1 Risk factors for oral HPV-related cancers include individuals who have multiple sexual partners and those who engage in oral sex practices.3 The Centers for Disease Control and Prevention (CDC) reported that approximately 44,000 people were diagnosed with HPV-related cancers between 2011 and 2015.5 While cervical cancer historically accounted for the greatest number of HPV-related cancers with 10,900 cases per year, HPV-associated OPC now account for 13,500 new cases annually.5 Incidence among males is nearly five times that of females, with 11,300 and 2,200 annual cases, respectively.5
Human papillomavirus infections can be prevented by vaccines that have been shown to be both safe and highly effective.6-8 While vaccine efficacy trials measured the prevention of cervical cancers, the vaccine targets the same virus types associated with HPV-related OPC and these vaccines are expected to also prevent OPC.6 While three vaccines were originally approved by the US Food and Drug Administration in 2006, Gardasil 9® (Merck; Kenilworth, NJ, USA) is currently the only vaccine available in the U.S. Gardasil 9® provides protection against 9 viral strains, including HPV 16, 18, the strains most often associated with OPC.6 Two to three doses are recommended based on the individual's age and risk factors. Following consultation with a health care professional, two doses have been recommended for those between the ages of 9 and 14 years, and three-doses for those between the ages of 15 and 45 years.8Despite vaccine availability, HPV vaccination rates remain low in the US compared to other routine childhood immunizations.9 As of 2018, only slightly more than half (51.1%) of adolescents in the US had completed the HPV-vaccine series.9
The lack of adherence to current vaccination recommendations may be due to lack of knowledge among the general population.10 Current public knowledge regarding HPV is largely related to cervical cancer and many people may be unaware of the relationship between HPV and OPC.11 Results from a national survey indicated that only 2% of the US population were able to identify HPV as a sexually transmitted infection and even fewer were aware of the link to OPC, creating intrinsic challenges for clinicians to dedicate additional time needed to provide vaccination education and patient counseling.
In 2016, the CDC reported that the number of people with a dental visit in the past year consisted of 84.6% children, aged 2-17 years; 63.4% adults, aged 18-64 years; and 64.3% adults, aged 65 and over.12 These data suggest that an opportunity exists to provide HPV-related education to those at greatest risk of HPV infection. Dental hygienists are well-positioned to provide HPV education as part of routine head and neck examinations and oral cancer screenings. This education opportunity includes the identification and discussion of risk factors in addition to early detection and diagnosis in the dental setting.13
Recent studies report that dentists and dental hygienists do not feel ready to discuss HPV-related risk factors with patients.14-18 One study found that most dental providers were not comfortable discussing the topic of HPV risk and transmission in the dental practice setting and that the level of comfort varied based on the patient's age, gender, and relationship to the provider.17 To overcome this provider discomfort, undergraduate dental hygiene programs should be prepared to assume the responsibility of preparing students with communication strategies regarding HPV infection, including vaccine advocacy. Dental hygiene students who are able to apply and practice these strategies will be better equipped to normalize conversations regarding HPV risk factors in clinical practice.
Currently there are no reports in the literature on how HPV topics are taught in US dental hygiene programs or whether dental hygiene faculty are trained to teach communication strategies related to HPV. The Commission on Dental Accreditation (CODA) Standard 2.24 indicates that dental hygiene programs are required to have an "ongoing curriculum review and evaluation process" with a "defined mechanism for coordinating instruction among dental hygiene faculty."19 The intent of this standard is to ensure that emerging information is periodically incorporated into the curriculum through workshops and in-service sessions, on an as needed basis. As HPV infection, and the ability to prevent disease through vaccination, is an emerging topic and of importance in oral as well as general health, it is important that dental hygiene programs consider the inclusion of curricular elements related to HPV. Furthermore, faculty may also benefit from preparation focused on HPV content in both didactic and clinical settings. The purpose of this study was to determine the extent to which HPV-related topics are taught in undergraduate dental hygiene programs in the US.
Methods
This study was reviewed and deemed exempt by the University of Minnesota (UMN) Institutional Review Board (STUDY00001463). A descriptive, cross-sectional design, consisting of a survey of US dental hygiene program directors and coordinators was used. Potential participants were identified from the American Dental Education Association's Listserv of dental hygiene program director emails as of January 2018 (n=335).
A link to an electronic survey was emailed to potential participants including a description of the study's purpose, the estimated time required to complete the survey and an informed consent option. Study data were collected and managed using the secure Research Electronic Data Capture (REDCap) software application hosted at UMN.20 The survey was available to participants during a six-week period in April - May 2018. Second and third emails were sent automatically to non-responders at two-week intervals following the initial invitation. All responses were anonymous and no identifying information was reported.
The survey was modified from a previously used validated instrument after receiving permission from the authors.21,22 The modified survey was pilot tested by six UMN School of Dentistry faculty members (five dental hygienists and one oral pathologist) and minor revisions were made based on the feedback. The 20-item survey included six demographic questions (institutional setting, degrees/credentials offered, average number of graduating students, program length, number of full-time faculty, and patient age groups served). Five items (yes or no responses) inquired about HPV-related curricula; use of HPV risk assessment in clinics, student requirement to discuss patient sexual risk factors or practices, faculty training to teach HPV-related topics, dental hygiene student engagement with other health care professional students, and HPV educational resource availability for patients. Three multiple-choice questions inquired regarding the number of hours spent in classroom instruction on HPV by program type; the estimated total number of hours of HPV didactic and clinical education; and the specific training of faculty responsible for teaching HPV-related OPC topics. Six items were specific to the total number of classroom and clinical hours students received regarding HPV and OPC risk; HPV screening, prevention, referral, infection management; knowledge of the HPV vaccine; skills in communication about HPV and the vaccine; and advocating for HPV vaccination for at-risk patients. Respondents also had the option for open-ended feedback in the last item.
Descriptive statistics reporting counts and proportions were used to analyze the data. SAS V9.3 (SAS Institute; Cary, NC, USA) statistical software was used for the analysis.
Results
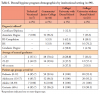
A total of 335 dental hygiene program directors and coordinators were invited to participate via email; 26 invit-ations were either duplicates or undeliverable. Of the unique and valid potential participants, 90 surveys were completed for a response rate of 29%. The majority of respondents were directors at community or junior colleges. Most programs graduated fewer than 25 students annually regardless of institutional setting. The patient population at all program sites was similar across pediatric, adolescent, adult, and geriatric age groups. Dental hygiene program demographics by institutional setting are shown in Table I.
Most respondents reported that HPV was included as part of classroom instruction content regardless of degree type or institutional setting. However, few dental hygiene programs included clinical assessments related to HPV (14.4%, n=90). The majority of programs limited the time spent on HPV-related topics to two hours or less. Few programs reported that their students engaged with other healthcare students on the topic of HPV, although students attending a college or university with a dental school were most likely to report interprofessional communication related to HPV. Similarly, few programs reported providing patients with HPV-related educational materials with technical/vocational schools and community colleges reporting the highest proportions. HPV- related topics and activities by institutional setting are shown in Table II.
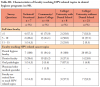
Characteristics of faculty teaching HPV-related topics in dental hygiene programs are shown in Table III. Nearly all instructors teaching HPV-related topics were dental hygiene faculty members (96%). In addition, dentists, oral pathologists or physicians/other medical specialists were also involved in teaching HPV-related topics (46.7%). Dental hygiene programs associated with a dental school were more likely to have an oral pathologist teach HPV content compared to programs without a dental school. Slightly more than one-fourth (26%) of faculty responsible for HPV content had completed special training on teaching HPV-related topics.
Discussion
Human papilloma virus-related content in dental hygiene curricula has not been previously reported in the literature. This study has similarities to research conducted by Wilder et al. regarding the introduction of another new topic into the dental hygiene curricula: the relationship between periodontal disease and systemic diseases.22 Similar to the Wilder et al. study, this new curricular content, HPV and OPC, received two hours or less time in the dental hygiene program, while topics such as cardiovascular diseases, diabetes and tobacco use, received between 3 to 5 hours.22
In this study, dental hygiene programs receiving the most classroom instruction on HPV-related topics were baccalaureate degree programs within a dental school, followed by those without a dental school, and the associate degree programs. Results were grouped by institutional type as baccalaureate degree programs have expanded requirements and require more time for degree completion compared to associate degree programs. Results from this study also confirmed that associate degree programs had fewer full-time faculty, perhaps increasing the difficulty of assuring a wide breadth of expertise. Curricular content may be more robust in institutions offering baccalaureate degrees. Further, dental hygiene programs offered at universities associated with dental school programs may have access to faculty members with specific expertise in head and neck cancers. This proximity often facilitates engaging resident experts in instructing dental hygiene and other related disciplines.
It is unclear whether providing up to two hours of HPV content results in dental hygiene students who can retain and apply the information upon graduation in clinical practice and additional professional development may be needed. In a study designed to test a web-based education module using a behavioral framework to encourage primary care providers (physicians, physician assistants, and nurse practitioners) to conduct oral cancer examinations on their patients, the majority of participants reported impactful learning for their professional practice and suggested that the 40 minute educational program be broken down into faster paced, 15-minute segments to accommodate busy schedules.23 While this finding is not directly comparable to teaching in a dental hygiene undergraduate program, these results may be helpful to provide HPV and OPC curricular content for practicing dental hygienists in continuing education settings.
Dental hygiene program directors in this study reported that 96% or more of instructors teaching HPV content were dental hygiene faculty with less than half receiving any training on how to teach HPV topics. Since there is limited evidence on HPV knowledge and training of dental hygiene educators, the available evidence on practicing licensed providers can be considered. Several studies report that few dental hygienists and dentists feel confident with their current HPV knowledge.14,15,24 Daley et al. identified knowledge deficits among dentists and dental hygienists, with a majority employed in a private practice setting.18 In another study, dental hygienists who scored significantly lower on the knowledge scale did not discuss HPV with patients compared to those who scored higher and were able to discuss HPV to some degree.15 Stull and Lunos found that 66% of respondents in the Minnesota dental community reported discomfort in HPV discussions with patients due to lack of knowledge along with other perceived barriers.14
Non-dental health care providers also report feelings of inadequacy when counseling patients on HPV-related issues. Afonso et al. examined HPV vaccination rates of millennial medical students (n=214) and discovered that while 82% of students believed in recommending the HPV vaccine, only 40% felt knowledgeable about the vaccine and were comfortable counseling patients.25 Overall, health care provider knowledge and comfort level in counseling patients about HPV vaccination appear to be lacking in multiple educational and clinical practice settings.
While research shows that dental hygiene clinicians are not comfortable having HPV discussions with their patients, it is not clear whether these findings apply to dental hygiene educators.15,24 Further research is needed to determine whether dental hygiene educators who teach HPV content are more comfortable having discussions with patients about HPV and other sensitive health topics in clinical education settings as compared to clinicians working in other practice settings.
Time constraints in crowded dental hygiene curricula may also affect the extent to which HPV content is represented. Hosking et al. surveyed pediatric dental program directors and found that while 77% of pediatric graduate program directors believe that they should discuss HPV vaccination with patients and parents, only 25% actually incorporate formal training related to HPV in their curriculum due to time constraints.26 However, 92.2% of directors reported a positive interest in showing their residents a 15-20 minute presentation about HPV vaccination and how to com-municate with parents.26 Strategies to combine HPV content in dental hygiene communication courses may be a potential resolution to the time limitations within the dental hygiene curriculum.
Results of this study found that patients are not receiving additional educational resources from the dental hygiene clinics where they receive care. Providing accurate information to patients is critical to disrupt disease transmission, particularly to those at high risk of contracting HPV.27,28 The dental community provides early head and neck cancer detection through routine screenings, and patients report that their most trusted source of oral health information is from their dental providers.13 Lazalde et al. reported that while parents are most comfortable with their child's primary care provider administering HPV vaccines, they reported high levels of comfort with dentists in other prevention roles, such as providing information about HPV vaccination or talking about HPV risk, suggesting that the dental office is an alternative practice setting suitable for participating in the delivery of education.29 Several organizations including the American Dental Association and the Centers for Disease Control and Prevention have developed HPV educational materials for oral health providers to deliver to patients in dental practice settings. Providers also can review and recommend emerging HPV information available through mobile apps, social media messages, videos, podcasts, fact sheets, brochures, and question and answer guides.
This study had limitations. While the sampling strategy included all dental hygiene program directors, the response rate was lower than desired. The low response rate may be due to lack of time or survey fatigue, as the ease of sending electronic surveys has increased the numbers of surveys distributed and requests are often ignored by recipients.30 Program directors focused on administration as compared to teaching, may not have accurate information regarding the exact amount of time spent, faculty training completed, or patient education provided specific to HPV. Further, while the survey instrument had been used previously, it was adapted for use in this study and the modifications were not validated. The cross-sectional design also limits the generalization of the results.
Future research should focus on the impact of effective HPV communi-cation, educational materials, and evaluation protocols for clinicians. Interprofessional collaborative efforts should be developed during dental hygiene education to improve HPV and OPC education and HPV vaccination efforts. Ongoing faculty development in HPV education should be supported as well as the role of HPV focused continuing education courses.
Conclusion
Results of this study indicate that dental hygiene programs, regardless of institutional setting, currently provide minimal didactic content and clinical application specific to HPV topics. Dental hygiene faculty teach HPV content in most DH programs, and few clinical teaching facilities provide HPV educational content to patients. More research is needed to understand the adequate time and teaching strategies required to assure that dental hygiene students are well-equipped to address HPV preventive strategies in clinical practice.
Disclosure
This study was funded in part by the University of Minnesota, School of Dentistry, Division of Dental Hygiene.
Kelli A. Trauger, RDH, MSDH is a teaching specialist; Cynthia L. Stull, RDH, MDH, DHSc is an associate clinical professor; Michelle C. Arnett, RDH, MS is an assistant professor; Christine M. Blue, RDH, DHSc is an associate professor; Priscilla M. Flynn, RDH, DrPHis an associate professor; all in the Division of Dental Hygiene, University of Minnesota School of Dentistry, Minneapolis, MN, USA.
Corresponding author: Kelli A. Trauger, RDH, MSDH: blan0207@umn.edu
References
1. CDC. Cancers caused by HPV are preventable [Internet]. Atlanta (GA): Centers for Disease Control and Prevention; 2020 [cited 2020 Nov 2]. Available from: https://www.cdc.gov/hpv/hcp/protecting-patients.html
2. CDC. HPV-associated cancer statistics [Internet]. Atlanta (GA): Centers for Disease Control and Prevention; c 2019-2020 [cited 2019 Mar 25]. Available from: https://www.cdc.gov/cancer/hpv/statistics/index.htm
3. Brown LM, Check DP, Devesa SS. Oral cavity and pharynx cancer incidence trends by subsite in the United States: Changing gender patterns. J Oncol. 2012;2012:649498.
4. National Cancer Institute. HPV and cancer; [Internet]. Bethesda (MD): National Cancer Institute; 2021 [cited 2021 Mar 24]. Available from: https://www.cancer.gov/about-cancer/causes-prevention/risk/infectious-agents/hpv-and-cancer#what-is-hpv
5. Saraiya M, Unger ER, Thompson TD, et al. US assessment of HPV types in cancers: implications for current and 9-valent HPV vaccines. J Natl Cancer Inst.2015 Apr 29;107(6):djv086.
6. CDC. HPV vaccine scheduling and dosing. Human papillomavirus [Internet]. Atlanta (GA): Centers for Disease Control and Prevention; c 2019-2020 [cited 2021 Mar 24]; [about 1 screen]. Available from: https://www.cdc.gov/hpv/hcp/schedules-recommendations.html
7. Food and Drug Administration. FDA approves expanded use of Gardasil 9 to include individuals 27 through 45 years old [Internet]. Washington (DC): Food and Drug Administration; 2018 Oct 18 [cited 2020 Nov 2]. Available from: https://www.fda.gov/news-events/press-announcements/fda-approves-expanded-use-gardasil-9-include-individuals-27-through-45-years-old
8. Food and Drug Administration. Patient information about GARDASIL®9 (Human Papillomavirus 9-valent Vaccine, Recombinant) [Internet]. Washington (DC): Food and Drug Administration; 2021 [cited 2021 Mar 24]. Available from: https://www.fda.gov/media/90070/download
9. Walker T, Elam-Evans L, Yankey D, et al. National, regional, state, and selected local area vaccination coverage among adolescents aged 13-17 years-United States, 2018. MMWR. 2019 Aug 23;68(33);718-23.
10. Demopoulos C, Stewart T, Ditmyer M. Bridging the HPV knowledge gap. Dimens Dent Hyg. 2017 Jun;15(6):32-7.
11. Friedman AL, Shepeard H. Exploring the knowledge, attitudes, beliefs, and communication preferences of the general public regarding HPV: findings from CDC focus group research and implications for practice. Health Educ Behav. 2007 Jun;34(3):471-85.
12. CDC. Oral and dental health. Diseases and conditions [Internet]. Atlanta (GA): Centers for Disease Control and Prevention; 2021 Mar 1 [cited 2021 Mar 24]; [about 12 screens]. Available from: https://www.cdc.gov/nchs/fastats/dental.htm
13. Oral Cancer Foundation. Dental information-support-advocacy-research…and hope [Internet]. Newport Beach (CA): Oral Cancer Foundation; 2021[cited 2021 Mar 24]. Available from: https://oralcancerfoundation.org/dental/
14. Stull CL, Lunos S. Knowledge, attitudes and practices regarding human papilloma virus communication and vaccine advocacy among Minnesota dentists and dental hygienists. J Dent Hyg. 2019 Feb;93(1):33-42.
15. Daley EM, Thompson EL, Vamos CA, et al. HPV-related knowledge among dentists and dental hygienists. J Cancer Educ. 2016;33:901-6.
16. Daley E, Debate R, Dodd V, et al. Exploring awareness, attitudes, and perceived role among oral health providers regarding HPV-related oral cancers. J Public Health Dent. 2011 Spring;71(2):136-42.
17. Northridge ME, Manji N, Piamonte RT, et al. HPV, oropharyngeal cancer, and the role of the dentist: A professional ethical approach. J Health Care Poor Underserved. 2012 Nov;23(4 Suppl):47-57.
18. Daley E, Dodd V, Debate R, et al. Prevention of HPV-related oral cancer: Assessing dentists' readiness. Public Health. 2014 Mar;128(3):231-8.
19. Commission on Dental Accreditation. Accreditation standards for dental hygiene education programs. Chicago (IL): American Dental Association; 2013 Jan. 44 p.
20. Harris P, Taylor R, Thielke R, et al. Research electronic data capture (REDCap)-A metadata-driven methodology and workflow process for providing translational research informatics support, J Biomed Inform. 2009 Apr;42(2):377-81.
21. Wilder RS, Lacopino AM, Feldman CA, et al. Periodontal-systemic disease education in U.S. and Canadian dental schools. J Dent Educ. 2009 Jan;73(1):38-52.
22. Wilder RS, Thomas KM, Jared H. Periodontal-systemic disease education in United States dental hygiene programs. J Dent Educ. 2008 Jun;72(6):669-79.
23. Wee AG, Zimmerman LM, Pullen CH, et al. Evaluating a web-based educational module on oral cancer examination based on a behavioral framework. J Cancer Educ. 2016 Mar;31(1):158-65.
24. Kline N, Vamos C, Thompson E, et al. Are dental providers the next line of HPV-related prevention? Providers' perceived role and needs. Papillomavirus Res. 2018 Jun;5:104-8.
25. Afonso NM, Kavanagh MJ, Swanberg SM, et al. Will they lead by example? Assessment of vaccination rates and attitudes to human papilloma virus in millennial medical students. BMC Public Health. 2017 Jan 6;17(35):1-9.
26. Hosking Y, Cappelli D, Donly K, Redding S. HPV vaccination and the role of the pediatric dentist: survey of graduate program directors. Pediatr Dent. 2017 Sep 15;39(5):383-9.
27. Kim HW. Awareness of human papillomavirus and factors associated with intention to obtain HPV vaccination among Korean youth: quasi-experimental study. BMC Int Health Hum Rights [Internet]. 2015 Feb 21;15:4.
28. Bakir A, Skarzynski M. Health disparities in the immunoprevention of human papillomavirus infection and associated malignancies. Front Public Health 2015 Dec 17;3:256.
29. Lazalde G, Gilkey M, Kornides M, McRee A-L. Parent perceptions of dentists' role in HPV vaccination. Vaccine. 2018 Jan;36(4):461-6.
30. Porter S, Whitcomb M, Weitzer W. Multiple surveys of students and survey fatigue. New Dir Inst Res. 2004 Mar 31; (121):63-73.