You must be signed in to read the rest of this article.
Registration on CDEWorld is free. Sign up today!
Forgot your password? Click Here!
Introduction
Depression is a rising global health concern characterized by decreased energy, sadness, feelings of guilt, low self-esteem, insomnia, chronic fatigue, and thoughts of death or suicide.1-4 Signs and symptoms of depression exist on a continuum, with variations in the length and severity of depressive episodes.1-4 The persistence of at least five of the diagnostic symptoms for a period of two weeks or more is considered an episode of major depressive disorder; the most common form of depression.5 In 2017, data from the Anxiety and Depression Association of America indicated that 7.1% of Americans reported having had at least one major depressive episode within the past year.6 While this statistic may seem relatively low, the rate of suicide has increased by 33% over the last two decades.7 The sharp increase in cases of depression, as well as, the associated systemic and oral health outcomes, underscores the need for quality medical and oral health care for at-risk individuals. However, research has shown that patients with depression and other mental illnesses may not receive this comprehensive care due to healthcare professionals' stigmatized views of mental health conditions.8-10 For the purposes of this review, the term "stigma" refers to prejudicial attitudes and discriminatory behaviors expressed toward people with depression.9
Substantial evidence has confirmed strong, sometimes bidirectional, relationships between depression and chronic systemic conditions known to have a strong association with periodontal diseases including type 2 diabetes, cardiovascular disease, autoimmune diseases, and other inflammatory disease conditions.11,12 Compounding this issue, research shows people with depression are less likely to maintain routine medical and dental care, which may, in turn, worsen and exacerbate these chronic diseases.1,13 While limited research has been reported in the literature focusing on the connections between depression and oral health status, emerging evidence has demonstrated the two are closely linked through changes in oral hygiene behaviors, immune response, increased inflammation, and decreased use of oral health care services.13,14 Consequently, this population is at an increased risk for dental caries, periodontal disease and tooth loss.13-15
Although various factors have been identified as potential barriers to health and dental care, stigmatization remains a prominent barrier to treatment and recovery for individuals with mental illness.9,17 Perceived and experienced stigmas may cause patients to be less likely to pursue treatment, while stigmatized viewpoints may influence decision-making and treatment outcomes.8,10 Some studies indicate that health care providers endorse the stigmatization of mental illness in a variety of settings.10,18,19 However, there is a gap in the literature regarding the perspectives of oral health care professionals towards individuals with depression. The sharp increase of depression across the United States (US) highlights the need for more research in dentistry in order to identify barriers to quality care and provide insight for future education and practice modifications. The purpose of this study was to explore oral health professionals' knowledge, attitudes, and practices toward patients with depression and evaluate the predictive relationship between variables.
Methods
A quantitative, cross-sectional study was developed using descriptive theory to identify characteristics of oral health care providers regarding depression and identify any relationships between these factors and the provision of oral health care. A knowledge, attitudes, and practices (KAP) survey model was selected to answer the research question, minimize bias, and maintain anonymity. The KAP assessment tool is designed to help reveal misconceptions or misunderstandings that may serve as potential barriers to a particular activity or behavior change.20
Survey instrument
The 24-item survey instrument was divided into the following sections: knowledge (6 items), attitude (4 items), practice-based (6 items), and demographics (8 items). The "attitudes" section of the survey used a modified version of the validated Depression Stigma Scale (DSS), designed to measure personal and perceived stigma toward depression.21 The original version of the DSS scale consisted of 18 questions; "personal stigma" (9 items) and "perceived stigma" (9 items).21 Personal stigma was defined on the DSS as an individual's own attitudes toward depression, while perceived stigma referred to an individual's belief about what others think regarding depression.21 Since the aim of this study was to measure the attitudes of oral health care providers toward depression, only questions from the "personal stigma" portion of the questionnaire were considered. The following items were selected based on relevance to this study: 1) People with depression could snap out of it if they wanted, 2) Depression is a sign of personal weakness, 3) People with depression are dangerous, and 4) If I had depression, I wouldn't tell anyone. The item "People with depression are dangerous" was modified to read "People with depression have a tendency to be lazy."
Items related to "knowledge" and "practices" were investigator developed and based on the most current research about depression. The modified KAP survey underwent content validity testing by four experts in the related mental and oral health fields, using a 4-point content validity index (CVI). Panel members included a mental/oral health researcher, oral health researcher, and two licensed mental health therapists. Based on the content validity index score (I-CVI = 1), no modifications were necessary.
Sample selection
The study used non-probability, convenience and snowball sampling methods. These methods were chosen to help increase the number of participants and gather responses from oral health professionals across the US. Oral health providers (dentists, dental hygienists, dental assistants, or dental specialists) who were fluent in English, actively practicing in the US, and over the age of 18 were eligible to participate. Non-English-speaking oral health professionals not currently practicing in the US or not currently licensed were excluded from the sample. In accordance with 45 CFR 46.101(B)(2), this study was assigned "exempt" status by the MCPHS University Institutional Review Board, IRB071618R.
Participants were recruited through online public Facebook forums, state oral health coalitions, dental hygiene and dental assisting state associations. In addition, administrators of the Iowa Dental Assistants' Association, Massachusetts Dental Hygienists' Association, West Virginia Oral Health Coalition, Pennsylvania Coalition for Oral Health, Washington State Oral Health Coalition, Indiana Oral Health Coalition, and the Kentucky Oral Health Coalition also agreed to forward the survey link via email to members of their organizations. Recruitment emails were sent directly by organization administrators and then forwarded to members via a mass email, to maintain privacy. Participants were encouraged to share the link with other oral health professionals who may qualify and be willing to participate in the study. The electronic survey remained open for a total of 35 days, and all Facebook posts were refreshed in week 3. Consent to participate was implied when the participant began the survey.
Statistical analysis
Descriptive statistics were used to analyze the data. Subscales for Likert scale responses were calculated by averaging item scores for each subscale to create a single score. Missing data responses were analyzed, and responses were weighted when necessary to adjust for data missing at random. Associations between all variables were examined using Spearman and Pearson correlations where appropriate and chi-square tests of independence. A test of internal reliability assessed the interrelationships of items for each subscale using Cronbach's alpha.22 Regression was used to determine the predictive relationship between predictor and outcome variables. Depending on assumptions of normality, linear, logistic, ordinal, or multinomial regression was used. All statistical hypothesis testing for this study used an alpha level of .05 and reported 95% confidence intervals (95%CI) and all other effect size statistics where appropriate.
A priori power analysis for this study was conducted using G*Power. Using 80% power, with a medium effect size (f2=.15), and alpha=.05, as parameters, the target sample size for regression testing was 77. All analyses were conducted using the Statistical Package for the Social Sciences, SPSS 23 (IBM, Armonk, NY).
Results
A total of 318 oral health care professionals completed the survey (n=318). Following data analysis 15 respondents were removed for missing more than 80% of questionnaire responses, 13 were removed for not meeting the inclusion criteria, and 2 were removed due to incomplete demographic information, leaving 288 respondents in the final sample (n=288). The vast majority of the sample were females (91%, n=261) with a mean age of 42.1 years (SD=13.7) and had been in practice an average of 17.3 years (SD=13.9). Demographic information is shown in Table I.
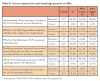
Separate analyses were conducted to describe the knowledge, attitude, and practice of the respondents. Knowledge was determined by creating a "knowledge score" with the number and percentage of correct responses out of six items. Overall, respondents answered 56% of the knowledge questions correctly. However, the majority of the participants (96%, n=277) overestimated the number of people suffering from depression in the US. The mean correct responses broken down by profession are shown in Table II. Responses to the individual knowledge questions are displayed in Table II.
The number of years in practice was negatively correlated (rho=-.34, p<.001) with having mental health education included during the respondent's professional education. Respondents who indicated having had an education that included curricular content in mental health were more likely to indicate that they review a patient's history of depression (rho=.17, p=.004). Interest in attending continuing education programs to learn more about depression was not significantly correlated with any other variable (p>.05). The knowledge score was not significantly correlated with any other variable in the study (p>.05).
Attitude questions had fair internal reliability with a Cronbach's alpha of .61 and were combined by averaging the four questions into a new variable "attitude." The mean attitude score by profession is shown in Table IV. Respondents who had been practicing longer and are older had a more positive attitude toward patients with depression (years of practice, rho=.19, p=.002; age, rho=.17, p=.004). Attitude was separated into individual questions to determine which specific questions were correlated to other variables. Agreement with the statement "People with depression have a tendency to be lazy" was negatively correlated with age (rho=-.28, p<.001), and years of practice (rho=-.29, p<.001); indicating that older professionals in practice longer tended to disagree with this statement.
Items regarding practices related to patients with depression were evaluated separately and are reported with the mean knowledge and attitude scores by profession in Table IV. Age was positively correlated with performance of reviewing or assisting in reviewing a patient's depression history during routine dental visits (r=.16, p=.007), as well as, referring or assisting in the referral of a patient to a mental health specialist (r=.30, p<.001). The number of years of practice was also positively associated with referring or assisting in the referral of a patient to a mental health specialist (r=.29, p=.001).
To examine the predictive relationship of the attitude and practice items, four separate logistic regression models were created. Each practice question (yes=1, no=0) was regressed onto attitude questions. Of the four different models, only the attitude statement "If I had depression I would not tell anyone" was inversely related to whether a respondent indicated that they had reviewed or assisted in reviewing a patient's depression history (Chi2 (1, 272)=4.46, p=.04). The result showed that a one-unit increase in agreement with the statement meant a person was 24% less likely to agree they review or assist in reviewing a patient's depression history (β=-76, p<0.001).
Two one-way ANOVAs were conducted to compare mean differences in attitude and knowledge scores between the oral health care professions. Mean differences in attitude scores were significantly different (F(2, 271)=3.61, p=.03, hp2=.03) with pairwise comparisons showing dentists had significantly more positive attitudes than dental assistants (p=.02, d=.54), and dental hygienists had more positive attitudes than dental assistants (p=.01, d=.43). There were no differences in attitude found between dentists and dental hygienists (p=.46). There were statistically significant differences in mean knowledge scores between the professions (F(1, 271)=3.03, p=.05, hp2=.02). Dental hygienists had a higher average knowledge score compared to dental assistants (p=.01, d=.57), but there was no difference between dentists and dental hygienists (p=.74).
Two one-way ANOVAs were conducted to compare mean differences in attitude and knowledge score between education levels. There were statistically significant differences in attitude between education levels (F(1, 272)=3.66, p=.01, hp2=.04), but not knowledge scores (F<1). Respondents with doctoral degrees had more positive mean attitude scores than those with bachelor (p=.01, d=.48) and associate degrees (p=.02, d=.48). Respondents with a master's degree also had more positive mean attitude scores than those with a bachelor (p=.02, d=.44) and associate (p=.04, d=.43) degree, but not a doctorate degree (p=.75). Attitude and knowledge scores, differentiated by the oral health care professions, are shown in Table III.
Discussion
Findings from this study of dental professionals are consistent with previous research regarding health care professionals' knowledge, attitudes, and practices regarding individuals with mental illness.10,19 A 2016 study of Finnish nurses demonstrated that while their attitudes towards patients with schizophrenia were generally positive, there were statistically significant correlations between the providers' attitudes and their experience, age, and mental health education.19 As each of these variables increased, the level of stigma toward patients with mental illness decreased,19 a finding that was similar to the oral health care providers in this study.
Research by Corrigan et al. showed that providers with greater personal stigma toward mental illness were less likely to refill patient's prescriptions and refer to specialists, thus impacting the individual's overall health.10 Results from this study, however, demonstrated that oral healthcare professionals were more likely to inquire about a patient's history with depression if they felt comfortable telling others about their own depression history and had less of a stigma regarding mental health. Better understanding of these correlations regarding the impact of personal stigma can lead to improvements in overall patient care.
Additionally, this study found that previous education experiences were also shown to influence oral health care providers' knowledge, attitudes, and practices toward patients with depression. While it was not possible to determine the exact type of education experience (lecture, clinical rotation, etc.) of the respondents, participants who indicated having had an education that included coursework on mental health were more likely to review a patient's history of depression. A randomized controlled trial by Papish et al. demonstrated that comprehensive, contact-based education as compared to an undergraduate psychiatry course integrating educational strategies was more effective in reducing stigma towards mental illness among second-year medical students.17 The "contact-based" approach involves presentations given by patients who share their stories of having a mental illness.17 Students are given the opportunity to ask the presenters questions regarding their experiences with their illness. This approach aims to reduce stigma by encouraging interpersonal contact with actual patients and can effectively be incorporated into professional health education courses.17 Improving the attitudes of younger, less experienced oral health professionals could begin with integrating similar experiences into dental education curricula.
Results regarding mental illness knowledge showed little variance in the number of correct responses across each category of oral health professionals (Table I). This lack of variation may have been due to similar levels of knowledge regarding depression across the oral health professions. It is also possible that the phrasing and multiple-choice format of the survey items may have led respondents to choose similar answers, regardless of the correct answer. The majority of respondents (96%, n=277) overestimated the percentage of depression prevalence in the US (correct response: 7%). In analyzing this response, a key detail has been identified as a possible explanation. The statistic used in the survey referred to people in the US diagnosed with major depressive disorder, which requires the symptoms to persist for two or more weeks. It is possible respondents assumed the term "depression" referred to all forms of depression, including the milder form.
The intent of this study was to address the gap in the literature regarding oral health care professionals' practices in caring for patients with depression. This study found that nearly one-third of the participants reported they did not review or assist in reviewing a patient's history with depression during dental visits. Results also showed that many oral health care professionals do not review how this medical condition may affect the patient's homecare practices, nor did they consider treatment modifications due to a patient's history with depression. It is possible that professionals who responded "no" to one or both of these questions did so because their role in the dental practice does not currently encompass these duties. It is possible that the dentist may have the role of reviewing the patient's medical history prior to treatment, therefore leading the dental assistant or dental hygienist within the same practice to respond "no." It is also possible that participants chose this response because depression and other mental health conditions have not been identified. This could be due to lack of a formal diagnosis, lack of patient disclosure, or the omission of depression and other mental health conditions from the medical history form. Also, oral health professionals may be avoiding discussing a patient's history with depression or making treatment modifications due to their own lack of understanding regarding the impact of mental illnesses on dental treatment and overall health and wellness. Increased education on depression and its effects on oral and systemic health may bring a heightened awareness to the importance of a holistic approach and the need to modify oral health care practices. Treatment modifications may not only improve the quality of care provided to these patients, but also decrease their risk for serious inflammatory conditions including cardiovascular and periodontal disease.12,16
Oral health professionals are responsible for identifying and treating oral diseases. However, the oral health provider role has continued to expand with emerging literature on oral/systemic health relationships. In this study, however, approximately one third of the respondents stated they had never referred or assisted in referring a patient to a mental health specialist. Taking into consideration the links that have been identified between depression and systemic conditions,12,14 oral health providers should consider screening for depression and referring to mental health specialists as a part of routine practice. Preliminary research has shown that general dentists to have a generally positive attitude towards developing a referral system.23 Doing so in dental settings could provide an opportunity to identify undiagnosed cases of depression, make referrals to mental health specialists, and open discussions regarding how depression may impact an individual's homecare routine, lifestyle, and overall health.
This study had limitations. Self-report questionnaires may be open to misinterpretation and leave little opportunity for clarification.24 The survey format may have served as a limitation, due to the inability to clarify questions of participants such as the terminology used to classify depression. Participants may also be susceptible to recall bias, particularly when dealing with personal issues and attitudes.24 Also, since respondents participated voluntarily, it is possible that the participants may have a greater interest in depression and mental health issues. Additionally, the professional distribution across the Facebook groups, coalitions, and associations was unknown, and the results may not be generalizable. Finally, although the use of an electronic survey allows for easy distribution, some participants did not complete the entire survey. As a result, non-response bias may play a factor.
Further research with a larger sample of oral health professionals is needed to verify the results of this study. Future studies should also explore the impact of contact-based education strategies on oral health professionals' attitudes and specific practice modifications. Research is needed to determine whether screening for depression in dental settings and developing a referral system to mental health specialists influences the oral and overall health of patients with depression.
Conclusion
Results from this study showed many oral health professionals do not review or assist in reviewing a patient's history with depression during dental visits, or discuss the impact of depression on a patient's homecare routine, nor do they consider treatment modifications due to a patient's history with depression. This study also showed a link between oral health professionals' comfort level when seeking mental health care for themselves and the likelihood that they would ask about a patient's history with depression, indicating that personal stigma could directly affect professional practice. Contact-based education strategies may be an appropriate addition to oral health curricula, as a means to provide future professionals with early exposure to mental illness and reduce stigmatized views.
About the Authors
Emily E. McCleary, MSDH, RDH, is an adjunct faculty member, Forsyth School of Dental Hygiene.
Lori Rainchuso, DHSc, MS, RDH, is a professor, School of Healthcare Business, Doctor of Health Sciences Program.
Jared Vineyard, PhD, is an adjunct faculty member.
Lori Giblin-Scanlon, DHS, RDH, is the Associate Dean for Clinical Programs, Forsyth School of Dental Hygiene.
All from MCPHS University, Boston, MA.
References
1. World Federation for Mental Health. Depression: A global crisis [Internet]. Occoquan (VA): World Federation for Mental Health; 2012 [cited 2019 July 20]. Available from: http://www.who.int/mental_health/management/depression/wfmh_paper_depression_wmhd_2012.pdf.
2. World Health Organization. Depression and other common mental disorders: Global health estimates [Internet]. Geneva (CH): World Health Organization; 2017 [cited 2019 July 20]. Available from: http://apps.who.int/iris/bitstream/10665/254610/1/WHO-MSD-MER-2017.2-eng.pdf.
3. American Academy of Periodontology. Periodontal disease and systemic health [Internet]. Chicago (IL): American Academy of Periodontology; 2017 [cited 2019 July 20]. Available from: https://www.perio.org/consumer/other-diseases.
4. Centers for Disease Control and Prevention. Dental and oral health [Internet]. Atlanta (GA): Centers for Disease Control and Prevention; 2019 Dec 4 [cited 2019 Dec 20]. Available from: https://www.cdc.gov/nchs/fastats/dental.htm.
5. Anxiety and Depression Association of America. Depression [Internet]. Silver Spring (MD): Anxiety and Depression Association of America; 2018 [cited 2019 October 25]. Available from: https://adaa.org/understanding-anxiety/depression.
6. National Institute of Mental Health. Major depression [Internet]. National Institute of Mental Health; 2019 Feb [cited 2019 Dec 20]. Available from: https://www.nimh.nih.gov/health/statistics/major-depression.shtml.
7. Hedegaard MD, Curtin SC, Warner M. Suicide mortality in the United States, 1999 - 2017. Hyattsville (MD): National Center for Health Sciences (US); 2018 Nov. NCHS Data Brief No.: 330.
8. Mitchell AJ, Malone D, Doebbeling CC. Quality of medical care for people with and without comorbid mental illness and substance misuse: systematic review of comparative studies. Br J Psychiatry. 2009 Jun;194(6):491-9.
9. Mental Health Commission of Canada. Opening minds, interim report. Calgary (CA): Mental Health Commission of Canada. 2013 Nov 18. Report No.: 11.18.13/250.
10. Corrigan PW, Mittal D, Reaves CM, et al. Mental health stigma and primary health care decisions. Psychiatry Res. 2014 Aug 15;218(1-2):35-8.
11. Caneo C, Marston L, Bellón JÁ, King M. Examining the relationship between physical illness and depression: Is there a difference between inflammatory and non-inflammatory diseases? A cohort study. Gen Hosp Psychiatry. 2016 Dec; 43:71-7.
12. Wu Q, Kling JM. Depression and the risk of myocardial infarction and coronary death: A meta-analysis of prospective cohort studies. Medicine (Baltimore). 2016 Feb;95(6):e2815.
13. Okoro CA, Strine TW, Eke PI, et al. The association between depression and anxiety and use of oral health services and tooth loss. Community Dent Oral Epidemiol. 2012 Apr;40(2):134-44.
14. Park SJ, Ko KD, Shin SI, et al. Association of oral health behaviors and status with depression: results from the Korean national health and nutrition examination survey. J Public Health Dent. 2014 Spring;74(2):127-38.
15. Kisely S, Sawyer E, Siskind D, Lalloo R. The oral health of people with anxiety and depressive disorders - a systematic review and meta-analysis. J Affect Disord. 2016 Aug; 200:119-32.
16. Peruzzo DC, Benatti BB, Ambrosano GM, et al. A systematic review of stress and psychological factors as possible risk factors for periodontal disease. J Periodontol. 2007 Aug;78(8):1491-1504.
17. Papish A, Kassam A, Modgill G, et al. Reducing the stigma of mental illness in undergraduate medical education: a randomized controlled trial. BMC Med Educ. 2013 Oct 24;13:141.
18. Ye J, Chen TF, Paul D, et al. Stigma and discrimination experienced by people living with severe and persistent mental illness in assertive community treatment settings. Int J Soc Psychiatry. 2016 Sep;62(6):532-41.
The Journal of Dental Hygiene 13 Vol. 94 • No. 5 • October 2020
19. Ihalainen-Tamlander N, Vahaniemi A, Loyttyniemi E, et al. Stigmatizing attitudes in nurses towards people with mental illness: A cross-sectional study in primary settings in Finland. J Psychiatr Ment Health Nurs. 2016 Aug;23(6-7):427-37.
20. Gumucio S, et al. KAP survey model (knowledge, attitudes, and practices) Data Collection - Quantitative Methods. Médicins du Monde. 2011 Jan;1-72.
21. Griffiths KM, Christensen H, Jorm AF, et al. Effect of web-based depression literacy and cognitive-behavioural therapy interventions on stigmatising attitudes to depression: Randomised controlled trial. Br J Psychiatry. 2004;185:342-49.
22. Faul F, Erdfelder EF, Lang AG, Buchner A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav Res Methods. 2007 May; 39:175-91.
23. Lloyd Williams F, Hillon D, Humphris G. A preliminary communication on whether general dental practitioners have a role in identifying dental patients with mental health problems. Br Dent J. 2001 Dec; 191(11):625-629.
24. Portney L, Watkins M. Foundations of clinical research: Applications to practice. 3rd ed. Upper Saddle River (NJ): F.A Davis Company; 2015. 696p.