You must be signed in to read the rest of this article.
Registration on CDEWorld is free. Sign up today!
Forgot your password? Click Here!
Introduction
Mental health and overall well-being have long been recognized in the United States (US) as areas of concern, as evidenced by the National Mental Health Act, signed into law in 1946.1 Recent estimates from the National Institute of Mental Health indicate that approximately 19% of adults in the U.S. have experienced anxiety, and about 16.2 million adults have had one or more major depressive episodes at some point in their life.2 Anxiety, like many mental health disorders, can interfere with daily activities such as work performance, school, and personal relationships.3 In regards to work performance, one major concern is professional burn-out. Professional burnout is characterized by emotional and physical exhaustion, detachment from work, and feelings of professional loneliness.4 When a person experiences an overload of chronic stress that is work-related, burn-out is frequently the end result.4 Professional burn-out is a concerning factor among many professions and has been shown to have a greater impact on individuals who work closely with others.4 Because the dental team works closely together to care for patients, dental professionals are at risk of experiencing burn-out.4
Recently, there has been growing interest and awareness of mental health as an essential component of overall health. However, there has been limited research on this topic among dental health professionals. The first study regarding the mental health and well-being of dental hygienists was conducted 20 years ago by Deckard and Rountree and focused specifically on burn-out.5 Respondents reported feeling emotionally exhausted, experienced high levels of depersonalization, and had negative feelings about their daily tasks in general.5 More current research has identified additional factors for occupational stress and negativity within the profession, with lack of autonomy and decision making in the workplace common reasons.6 Individuals with lower levels of autonomy, who struggled to identify their professional roles, were shown to experience the most burn-out.6 Another common theme in the literature has been the need to incorporate stress management courses within dental hygiene programs.4,6 By addressing stress management as part of the dental hygiene curriculum, new graduates can have a better understanding of how they like to work, and this knowledge may help to reduce the likelihood of experiencing burn-out.4 Stress assessment tools, policies, and open communication are methods currently suggested in the literature for stress reduction among dental professionals.4
There is an overall lack of research pertaining to the mental health of dental hygienists in the US; however, a number of studies have been conducted outside of the US.6 In a study pertaining to job satisfaction among Dutch dental hygienists, those who held a four-year degree in the Netherlands had more autonomy and felt fewer symptoms associated with stress than those with a two-year degree.6 Dental hygienists in Canada reported lack of job satisfaction and stress stemmed from low pay and insufficient benefits.6 These studies suggest dental hygienists in different areas of the world experience various stressors related to their scope of practice.6 In addition to a lack of autonomy, existing literature identifies other stressors that contribute to low job satisfaction. These stressors include demanding schedules and patients, lack of time, and musculoskeletal complaints.7,8 Musculoskeletal disorders are a common issue among the dental hygiene profession and can lead to a decrease in clinical working hours.7 Sick leave among dental hygienists has been shown to be significantly higher among professionals with musculoskeletal complaints.7
Organizational work factors and work-family overload are additional contributing stressors that can lead to a greater prevalence of reduced mental health and well-being.8 Elevated mental health and well-being were associated with a high perception of personal mastery, active leisure, and high levels of management support.8 Similar research has been conducted on stress, anxiety, and burn-out of dentists.9 These studies conclude that due to the nature of clinical practice, general dentists and those in the field of dentistry are likely to experience burn-out in their profession.9
While there is limited research available regarding burnout of dental professionals, there are multiple studies on burnout within other health professions. A study conducted on the incidence of burn-out in US physicians revealed almost half of the studied physicians reported feeling symptoms of burn-out.10 Burn-out was described as feelings characterized by loss of enthusiasm at work, feeling cynical, and having a low sense of personal accomplishment.10,11 Long-term effects of burn-out experienced by physicians can lead to adverse effects towards patient care.10 Nurses and other medical staff members experience similar feelings of low job satisfaction and burn-out. In a study of hospital nurses working in the US, the majority reported experiencing symptoms of burnout.12 When staff members are experiencing burn-out, they are typically not performing to the best of their abilities. This diminished level of job performance can place added stress on the doctor and supporting staff they are working with, decreasing the overall quality of care being provided.11
The majority of current research on mental health and well-being of dental hygienists has been limited focusing on ergonomics and musculoskeletal issues associated with dental hygiene occupational stress.7,8 Existing research suggests occupational stress and burn-out among dental hygienists may produce a decline in overall mental health and wellbeing, increase physical strain, and may lead to chronic disease over time.4,9 However, little is known about the prevalence of mental health conditions and self-care strategies among dental hygienists. More in-depth investigation of the incidence, risk factors, and resources available is needed, in order to determine better coping methods and ways to avoid job related burn-out for dental hygienists.4 The purpose of this study was to gather data regarding the mental health status, self-care practices, and stress triggers among dental hygienists.
Methods
This cross-sectional survey study of dental hygienists in the state of Oregon was deemed exempt by the Pacific University Institutional Review Board. The survey instrument was developed by the authors and was pilot tested by 3 dental hygienists and 1 mental health professional, and revisions were made based on feedback. The final survey instrument consisted of 28 items which addressed the following areas: participants' experiences with symptoms of depression and anxiety, perception of stress, support system, consultation with a mental health professional, strategies for stress relief, work benefits and incentives surrounding mental health and wellbeing, work history, and demographics. The online survey was developed using Qualtrics software (Qualtrics; Provo, UT) and administered via email to members of the Oregon Dental Hygienists Association (ODHA). A total of 251 invitations were successfully delivered to the ODHA membership listserv.
Descriptive and inferential statistics were computed using SPSS version 23 (IBM; Armonk, NY). Inferential analyses (Fisher's Exact Tests) were conducted to determine whether perceptions of stress and stress management practices varied based on the total number of hours worked per week, type of dental hygiene position, and clinical practice type. The level of statistical significance was set at 0.05.
Results
A total of 83 ODHA member dental hygienists agreed to participate for a response rate of 33%. Ninety-five percent (n=79) of the population surveyed worked in general dentistry, 5% (n=4) in periodontics, 1% (n=1) in pediatric dentistry, and 10% (n=8) in a public health setting. Regarding the number of hours worked per week, 45% worked 31-40 hours per week (n=38), while 40% (n=33) worked on average, less than 30 hours per week.
Respondents were asked to rate their average daily stress level in 3 categories; low, moderate and high. Sixteen percent of respondents (n=13) reported having high daily stress levels, while over half (65%, n=54) reported having a moderate daily stress level and 19% reported low daily stress (n=16). Participants were also asked to what extent they felt their daily stress levels were due to work. Eleven percent (n=9) felt their stress was entirely due to work, while 57% (n=46) felt it was primarily due to work, 28% (n=25) felt it was somewhat due to work, and 4% (n=3) felt it was not related to work. Fisher's Exact tests revealed that dental hygienists who worked ≥20 hours per week were more likely to attribute their daily stress primarily or entirely to work (p=0.009). Participants were also asked to rate how well they were managing their daily stress levels. Seventeen percent (n=14) indicated extremely well, 60% (n=50) somewhat well, 10% (n=8) neutral, and 13% (n=11) somewhat poorly. Fisher's Exact tests revealed that the number of hours worked per week was directly related to the perception of managing stress, indicating that participants who worked more hours per week felt less able to manage their stress (p=0.006).
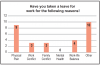
Thirty-eight percent of respondents (n=32) reported on their reason(s) for taking leave from work (Figure 1). Of these respondents, 11% percent (n=9) responded that their work leave was due to physical pain, while 12% (n=10) reported work leave was taken for unspecified specified reasons. None of the respondents indicated mental health as a reason for taking leave from work. When asked to select what most often triggered stress among those who responded, 35% (n=29) of the participants stated difficulty maintaining a work-life balance, while 34% (n=28) mentioned a dysfunctional work team as a stress trigger, and 65% (n=54) indicated not enough time in the work schedule as a stress trigger (Figure 2).
When the participants were asked what type of support system they had outside of their work environment, a majority (92%, n=76) identified their family while three-fourths (78%, n=65) stated that their friends served as their support system. Additionally, 8% (n=16) of respondents sought support outside of work with a mental health professional and 8% (n=16) sought support with a community organization. About one third (36%, n=30) of the participants reported that their employer offered incentives to help with stress reduction. Examples of employer provided incentives included team building opportunities (17%, n=14), travel opportunities (6%, n=5), and other unspecified incentives (8%, n=7). Eight percent (n=7) found these incentives to be very beneficial, 11% (n=9) found the incentives somewhat beneficial, and 4% (n=3) stated they had neutral feelings about how helpful their office incentives contributed to their mental health. None of the participants indicated that the incentives were detrimental to their mental health and well-being.
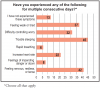
Respondents were asked to identify symptoms of depression and anxiety experienced over multiple consecutive days. These conditions were not labeled as symptoms of anxiety and depression on the survey. Data revealed the most common symptoms of depression were anger, irritability, and frustration (n=44), appetite and weight changes (n=26), and difficulty thinking, concentrating and making decisions (n=25) (Figure 3). Data identified symptoms of anxiety were trouble sleeping (n=45) and feeling nervous, restless, or tense (n=42). Nineteen percent of the respondents indicated that they had consulted a mental health professional about their mental health concerns (Figure 4).
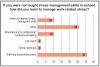
The majority of respondents reported that having more time to engage in self-care activities (71%, n=59) and improved working conditions (57%, n=47) would be the most successful stress reduction interventions. Other responses included additional education (14%, n=12), and seeking a new profession (17%, n=14). When the respondents were prompted to identify how they learned to manage stress, over one third (37%, n=31) identified learning through self-help books and instructions and a little less than one-third (31%, n=26) reported learning stress management through other unspecified methods. Only 21% (n=17) reported receiving information or training on stress management and or burn-out during their dental hygiene education (Figure 5).
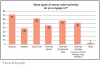
When prompted to identify all of the various types of stress relief activities the respondents engaged in, 85% (n=71) reported exercise, 73% (n=61) quiet time, 67% (n=57) spending time with loved ones, 62% (n=51) self-care activities, and 4% (n=3) other (Figure 6). Examples of self-care activities included manicure, pedicure, massage, meditation, and yoga. Respondents were asked how often they engaged in stress reduction activities, both on the average, and during times of significant stress. Rates of participation in stress-relief activities were shown to be lower during times of significant stress, with the majority 39% (n=33) stating 1-2 days per week, followed by 27% (n=22) who selected 3-4 days per week. In regard to the average frequency of stress-relief activities, 26% (n=21) selected 1-2 days per week, 42% (n=34) selected 3-4 days per week, 21% (n=17) selected 5-6 days per week, and 11% (n=9) selected daily.
Discussion
Results from this study support findings from other studies in the existing pool of literature. Nearly half of the participants experienced symptoms of nervousness, tiredness, restlessness, trouble sleeping, anger, and irritability for multiple consecutive days. Similar symptoms have been noted in general dentists as well.9 Of the study participants, over half had not consulted with a mental health professional regarding mental health concerns. In addition, over half of the respondents reported moderate levels of daily stress, with lack of time in schedule, physical pain, and the neediness of patients the most commonly identified triggers. These findings are relevant as they identify specific stress symptoms and triggers. Data suggest that a large portion of practicing dental hygienists experience work related stressors that may contribute to burn-out.
These findings have importance for practicing dental hygienists, because they shed light on the prevalence and nature of decreased mental health and well-being within dentistry. Members of the profession should understand that increases in symptoms such as mental fatigue, impatience, headache, and anxiety can contribute to more frequent leaves from work and to an overall decrease in longevity of clinical career.7 In addition to expanding the research within this area, this study identified methods of stress management currently utilized by practicing dental hygienists. It is important that stress triggers and symptoms be identified to help prevent future negative mental health disorders and burn-out within the dental hygiene profession.
The majority of participants in this study did not receive training during their dental hygiene education regarding stress management. While data suggests stressors and poor mental health are prevalent in practice, there is a lack of curricular content dedicated to the subject within formal education programs. Results from this study supported the existing literature regarding a need for dental hygiene schools to implement stress management courses in their curriculum.4,6,8 Other studies have also suggested that incorporating stress management into dental hygiene education would provide new practitioners the opportunity to reflect on their ideal work environment, resulting in decreased work-related stress.4 However, education on stress management is not currently a required element according to the standards set forth by the Commission on Dental Accreditation (CODA).13 While it is not required, the addition of a stress management course or related content could benefit students by preparing them to deal with stressors that could lead to burn-out in addition to improving conflict resolution and communication skills.4
Participants reported learning to unwind, including participating in leisure and self-care activities, helped with managing work-related stress. Previous research has shown that stressors experienced by practicing dental hygienists were related to lack of time in the schedule and musculoskeletal complaints.4,7,8 Findings from this study support previous research showing that dental hygienists identify a lack of time in their schedule as a major contributor to stress in the work place. Physical pain was an additional reason for taking time off from work and the second most commonly experienced stressor among the participants in this study.
Burn-out is universal among all health care providers and has been shown to negatively affect the care that patients receive.14 Research has shown that when the health and work life of providers improves, better patient care follows.14 Physicians experiencing burn-out have been shown to have less empathy for their patients, deviate from treatment plans, and prescribe unnecessary medications.15,16,17 Burn-out has been shown to be particularly prevalent among professions with a high number of interactions with other people18 making it reasonable to expect to see a higher level of burn-out among dental hygienists.
Previous research focusing on burn-out and mental well-being of dental hygienists has shown that lack autonomy was one of the largest stressors leading to symptoms of stress, anxiety, depression, and burn-out among dental hygienists.4,6 While this study did not specifically inquire about lack of autonomy, lack of decision making was an included item. A relatively small proportion of respondents (14%, n=12) reported that lack of decision-making ability was a stressor. This inconsistency with existing literature could be a result of Oregon's progressive practice act and broad scope of practice for dental hygienists.
This study had limitations. The sample population was limited to the 251 members of the ODHA and does not reflect dental hygienists outside of the state of Oregon. While a 33% response rate is acceptable for survey research, a larger sample size would increase the generalizability of the results. There is also the potential for non-response bias due to the sample population. Participants were all members of the ODHA and may not be representative of the entire population of dental hygienists. Future research on this topic should include a more representative sample of all dental hygienists by expanding the survey nationwide. A national survey would also allow for a comparison between practice acts with differing responsibilities and levels of autonomy. A larger survey sample would add knowledge regarding the impact of the dental industry on mental health and identify areas where changes in education and professional practice could be made.
Conclusion
Dental hygienists in Oregon experience symptoms associated with depression and anxiety. The most common triggers for feeling stressed were a lack of time to spend with patients, demanding needs of patients, work schedules, physical and musculoskeletal pain, and difficulty maintaining a balance between work and personal life. The most common methods of stress management used were exercising, quiet time, and spending time with loved ones. While mental health symptoms were indicated by some of the respondents, few have sought services with a mental health care provider. Future research is needed on the mental health and well-being of dental hygienists on a national level to provide an understanding and a way to help manage symptoms of anxiety and depression to prevent burn-out.
About the Authors
SaraJane A. Barnard, RDH, BSDH; Bree A. Alexander, RDH, BSDH; Ashli K. Lockett, RDH, BSDH; are graduates of the School of Dental Hygiene Studies, Pacific University, Hillsboro, OR. Jennifer J. Lusk, RDH, BSDH is an adjunct clinical faculty member; Kathryn P. Bell, RDH, EPDH, MS; is an associate professor in the School of Dental Hygiene Studies and the Associate Dean for Interprofessional Education; Lesley A. Harbison, RDH, EPDH, MS is an assistant professor in the School of Dental Hygiene Studies; all at Pacific University, Hillsboro, OR.
Corresponding author: Lesley A. Harbison, RDH, EPDH, MS; Lesley.harbison@pacificu.edu
References
1. National Institutes of Health. Mission statement [Internet]. Bethesda: National Institute of Health; 2018 [cited 2018 Nov15]. Available from: https://www.nih.gov/about-nih/what-we-do/nih-almanac/national-institute-mental-health-nimh.
2. National Institute of Mental Health. Major depression [Internet]. Bethesda: U.S. Department of Health and Human Services; 2019 [cited 2018 Nov13]. Available from: https://www.nimh.nih.gov/health/statistics/major-depression.shtml.
3. National Institute of Mental Health. Any anxiety disorder [Internet]. Bethesda: U.S. Department of Health and Human Services; 2018 [cited 2018Nov12]. Available from: https://www.nimh.nih.gov/health/statistics/any-anxiety-disorder.shtml
4. Gorter R. Work stress and burnout among dental hygienists. Int J Dent Hyg. 2005 May; 3(2):88-92.
5. Deckard GJ, Rountree B. Burnout in dental hygiene. J Dent Hyg 1984 July; 58: 307-13.
6. Lopresti S. Stress and the dental hygiene profession: risk factors, symptoms, and coping strategies. C J Dent Hyg. 2014; 48(2): 63-9.
7. Petrén V, Petzall K, Preber H, et al. The relationship between working conditions and sick leave in Swedish dental hygienists. Int J Dent Hyg. 2007; 5(1): 27-35.
8. Ylipaa V, Szuster F, Spencer J, et al. Health, mental well-being, and musculoskeletal disorders: a comparison between Swedish and Australian dental hygienists. J Dent Hyg. 2002; 76 (1): 47-58.
9. Rada RE, Johnson-Leong C. Stress, burnout, anxiety and depression among dentists. J Am Dent Assoc. 2004; 135(6):788-94.
10. Shanafelt TD, Boone S, Tan L, et al. Burnout and satisfaction with work-life balance among US physicians relative to the general US population. Arch Intern Med. 2012;172(18):1377-85.
11. Friedberg MW, Chen PG, Van Busum KR, et al. Factors affecting physician professional satisfaction and their implications for patient care, health systems and health policy. Rand Health Q. 2014 Dec 1;3(4):1. eCollection Winter 2014.
12. McHugh MD, Kutney-Lee A, Cimiotti JP, et al. Nurses' widespread job dissatisfaction, burnout, and frustration with health benefits signal problems for patient care. Health Aff (Millwood). 2011; 30(2):202-10.
13. Commission on Dental Accreditation. Accreditation standards for dental hygiene education programs [Internet]. Chicago: American Dental Association; 2019 [cited 2019 Mar 12]. Available from: http://www.ada.org/~/media/CODA/Files/2016_dh.ashx
14. Bodenheimer T, Sinsky C. From triple to quadruple aim: care of the patient requires care of the provider. Annals Fam Med. 2014; 12(6):573-6.
15. Hojat M, Louis DZ, Markham FW, et al. Physicians' empathy and clinical outcomes for diabetic patients. Acad Med. 2011; 86(3):359-64.
16. DiMatteo MR, Sherbourne CD, Hays RD, and et al. Physicians 'characteristics influence patients' adherence to medical treatment: results from the Medical Outcomes Study. Health Psychol. 1993; 12(2):93-102.
17. Williams ES, Skinner AC. Outcomes of physician job satisfaction: a narrative review, implications, and directions for future research. Health Care Manage Rev. 2003; 28(2):119-39.