You must be signed in to read the rest of this article.
Registration on CDEWorld is free. Sign up today!
Forgot your password? Click Here!
Local anesthetics (LAs) are the safest and most effective drugs in medicine for the prevention and management of pain. Local anesthetics are one of the few classes of drugs that prevent a nociceptive impulse from reaching the patient's brain where it would be interpreted as pain. Deposit a LA close to a nerve and it will-in virtually all clinical situations-provide effective pain control. Annually, in the United States, approximately 300 million dental LA cartridges are administered.1 Worldwide, 1.96 billion cartridges are used by the dental profession.2 Five LAs are available in dentistry. Availability and specific formulations of these drugs vary from country to country.
Pharmacology
Local anesthetics-lidocaine, for example-are insoluble in water. Hydrochloric acid (HCl) is added to the anesthetic, producing the water-soluble acid salt-lidocaine HCl. The pH of a "plain" LA (without a vasoconstrictor such as epinephrine)-mepivacaine HCl 3% and prilocaine 4%-is approximately 6.5. Plain LAs provide a relatively short duration of not-as-profound anesthesia as the same drug formulated with a vasoconstrictor.3
The addition of a vasoconstrictor to the LA confers three significant advantages: (1) increased duration of pulpal anesthesia; (2) increased depth of pulpal anesthesia; and (3) increased safety of the anesthetic formulation.4
However, epinephrine is quite labile-easily "destroyed" by exposure to heat, light, and oxygen.5 With some variability, the average "shelf-life" of a cartridge of "plain" LA is 36 months, while that of a vasoconstrictor-containing cartridge is 24 months. To maximize the shelf-life of the vasoconstrictor-containing LA cartridge, an antioxidant-Na+ metabisulfite-is added to the cartridge. This lowers the pH of the cartridge to approximately 3.5.6 As Na+ metabisulfite is oxidized into metabisulfate, over time its pH is further lowered to approximately 3.0. Clinicians know from experience that as an epinephrine-containing LA is being injected, patients experience a self-described uncomfortable burning sensation.
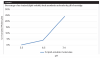
For a LA to block nerve conduction, it must first diffuse through the lipid-rich nerve membrane to the interior of the nerve where it then blocks Na+ channels, preventing the propagation of the nerve impulse. To do this, local anesthetics must also be lipid soluble. An organic ring confers lipid solubility to the LA-most dental LAs have a benzene ring, whereas articaine has a thiophene ring. Depending upon the pH of the LA solution in a cartridge, the percentage of lipid-soluble (un-ionized) molecules will vary considerably. At a 3.5 pH (lidocaine with epinephrine), only 0.004% of the lidocaine molecules in a cartridge are lipid soluble. As pH increases, the percentage of lipid-soluble molecules increases-at a pH of 6.5 ("plain" lidocaine), 3.83%; at 7.4 (pH of the human body), this increases to 24.03% (Figure 1). This process-buffering-begins as soon as the LA is injected into the patient's soft tissue but is exquisitely slow. Fernandez et al demonstrated a success rate (pulpal anesthesia) of 95% following an inferior alveolar nerve block (IANB) with lidocaine 2% with epinephrine 1:100,000. However, it took 45 minutes to reach that level.7
Onset Time for Pulpal and Soft Tissue Anesthesia
As mentioned in the previous paragraph, the low pH of vasoconstrictor-containing LAs leads to a slower onset of pulpal anesthesia. The drug package inserts (DPIs) of LAs indicate an onset of 3 to 5 minutes for infiltrations and from 5 to 7 minutes for nerve blocks.8 These numbers can be traced back to the primary local anesthesia textbook used from 1957 through the late 1970s-Leonard Monheim's Local Anesthesia and Pain Control in Dental Practice.9
However, in "real life" clinical dental practice, most dentists estimate that they wait 10 minutes for their anesthetic to take effect. However, a survey of dental assistants found the average time most dentists wait after injection to check a patient for anesthesia was 15 minutes.10
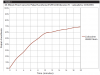
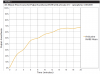
Why do dentists wait longer that the time recommended in the drug package insert? Well-designed, randomized, controlled, clinical trials (RCTs), as well as the real-life experiences of dentists, demonstrate that these numbers are far from accurate.11 In a meta-analysis of 34 RCTs involving 1,078 subjects, in which lidocaine 2% with epinephrine 1:100,000 was administered by IANB and pulpal anesthesia was assessed every 2 minutes for 30 minutes using an electric pulp tester (EPT), it was demonstrated that at 6 minutes following injection, 40% of the subjects had achieved pulpal anesthesia.11 This increased to 60% at 10 minutes and 65% at 15 minutes (Figure 2). A review of 5 RCTs (n = 222) with articaine 4% with epinephrine 1:100,000 produced an almost identical curve11 (Figure 3).
In a paper reporting on how patients evaluate their dentist, the second most important factor was "a dentist who doesn't hurt" (second only to "the ability to give a painless injection").12
There is no correlation between soft tissue anesthesia and pulpal anesthesia. In a clinical trial by Lai et al, soft tissue anesthesia was evaluated every 2 minutes (using a sharp dental explorer) following IANB with lidocaine 2% with epinephrine 1:100,000.13 At 10 minutes, approximately 87.5% had soft tissue anesthesia, increasing to slightly less than 90% at 15 minutes.
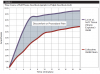
Many dentists rely on soft tissue anesthesia (eg, lip and tongue) as a gauge of pulpal anesthesia. "Are you numb?" is frequently asked by the dentist. The patient bites his or her lip and/or tongue, and if the response is "yes," the procedure begins. If, at 10 minutes following IANB, 87% of patients have profound soft tissue anesthesia (Figure 4, purple line) but only 60% have pulpal (Figure 4, red line), the patient experiences pain when the bur enters into dentin.11,13
Therefore, it behooves one to consider whether it is possible for a dentist to confirm pulpal anesthesia prior to starting a dental procedure. In clinical research, the electric pulp tester (EPT) is most commonly employed. The ability to apply a maximum EPT output to a tooth with no response from the patient is (in non-pulpally involved teeth) a 90% or higher guarantee of successful pulpal anesthesia.14 A similar result can be obtained more easily with a refrigerant spray, such as Endo Ice or Endo Freeze, applied to the tooth using a cotton pellet.15,16
Buffering: More Effective and More Comfortable
Buffering of the LA cartridge-raising its pH to 7.4-significantly increases the percentage of lipid-soluble (un-ionized) molecules found in the cartridge and confers several benefits, including: (1) more rapid onset of pulpal anesthesia; (2) more comfortable injection; (3) more profound pulpal anesthesia; and (4) less post-injection soreness.17
In a double-blind RCT, patients received an IANB on two occasions with lidocaine 2% with epinephrine 1:100,000: a "traditional" cartridge (pH ~3.5), and a buffered cartridge (pH 7.4).17 Onset of pulpal anesthesia (EPT) was 6 minutes and 37 seconds for traditional lidocaine, and 1 minute and 51 seconds with the buffered lidocaine. Seventy-one percent of the buffered IANBs achieved pulpal anesthesia in less than 2 minutes, compared to only 12% of the traditional IANBs. Using a visual analogue scale (no pain = 0; worst pain imaginable = 10), 44% of buffered IANBs were zero, compared with 6% unbuffered IANBs.17
Buffering of LAs increases the depth of pulpal anesthesia. A meta-analysis compared the effectiveness of buffered versus unbuffered LAs in both maxillary and mandibular pulpally involved teeth. The authors concluded "this investigation revealed that buffered local anesthetics are more effective than unbuffered local anesthetics when used for mandibular or maxillary anesthesia in pulpally involved teeth. Buffering of local anesthetics has a 2.29 greater likelihood of achieving successful anesthesia."18
The evaluation of patient comfort post-injection (soreness) demonstrated that 72% preferred the buffered LA to only 11% of the traditional.17 Following IANB with a traditional LA, patients will feel soreness the following day from (1) soft tissue trauma due to needle insertion, and (2) the highly acidic LA solution. With buffered LAs, only the needle trauma is present.
Incorporating Buffering into the Dental Practice
Besides the benefits of buffering LA cartridges presented above, buffering can also save a dentist considerable time on every patient. Following IANB, most dentists leave their patients for 10 to 15 minutes while they "get numb." At 10 minutes only 60% of patients are adequately numb; at 15 minutes only 67%.11 To realize, after 10 or 15 minutes, that the IANB has failed and that reinjection is necessary can add chairtime and stress to the dental appointment for both the dentist and patient.
When administering an IANB with a buffered LA, wait 2 minutes and then, using an EPT or refrigerant spray, assess the tooth for pulpal anesthesia. If no response, begin the dental procedure. If there is a response, repeat the injection, again using buffered LA. Saving 10 to 15 minutes per patient may have a significant impact on the way a dentist practices.
How to Buffer
Three buffering options for dental LAs are presently available: "do it yourself" (DIY) and two commercial systems.
Medical doctors who use local anesthetics-primarily dermatologists, allergists, and plastic and reconstructive surgeons-buffer LAs on a regular basis, as the administration of LA into skin is painful.19 Physicians do not use prefilled cartridges of local anesthetics, instead using multidose bottles (50 mL) of lidocaine 1% or 2% with epinephrine 1:100,000; a multidose bottle (50 mL) of 8.4% sodium bicarbonate (the buffering solution); and a plastic disposable syringe. The medical literature is replete with articles describing DIY techniques and their success rates. Ratios of 10 parts lidocaine to 1 part bicarbonate; 5 to 1; and 30 to 1 have been reported with varying results.20-22
In order to guarantee successful buffering of a local anesthetic cartridge to a pH of approximately 7.4, one needs to know the pH of the buffering agent, Na+ bicarbonate, as its pH will determine the final pH of the combined solution. If the resultant pH of the LA cartridge is not high enough (<7.0), the benefits of buffering will not be observed. If the pH of the solution is too high (~7.58 or higher), several (non-life-threatening) complications-edema at the injection site and/or a precipitate forming inside the LA cartridge-might be observed (see below).23,24
As the pH of Na+ bicarbonate determines the final pH of the LA solution, it is important to know its pH prior to buffering. The label on the multidose vial of Na+ bicarbonate lists the pH as 7.8. However, in parentheses it states that the pH may range from 7.0 to 8.5. Being that pH is a logarithmic scale, each increase or decrease in pH value represents a significant change in the acidity of the fluid or tissue being tested.
Dentists who have tried DIY have also had varying results. Using a 1.0-mL tuberculin syringe, a volume of LA (commonly 0.2 mL) is removed from the cartridge with an equal volume of Na+ bicarbonate added-also called "remove and replace." The pH of the cartridge is now that of the buffering agent.
Anecdotal reports from a number of dentists using DIY buffering have described the occurrence of edema (in one instance "about the size of a golf ball") at the site of buffered LA injection.25,26 In one instance the dentist had used a bottle of 8.4% Na+ bicarbonate successfully and without complication, with the edema occurring following the first injection from a "new" bottle of Na+ bicarbonate.25 A possible cause of the edema is that the pH of the new Na+ bicarbonate bottle was significantly higher than that of the original bottle. Injection of LA at a pH greater than 7.58 produces edema by causing water to diffuse out of cells.
Several commercial buffering options also exist. One such uses multidose Na+ bicarbonate and multidose lidocaine.27 Similar to DIY (unknown pH of the bicarbonate), this system limits the dentist to the use of one local anesthetic (lidocaine 2% with 1:100,000 epinephrine), as well as requiring the use of a plastic syringe for the delivery of the LA injection. Another system, introduced in 2010, permits buffering of any local anesthetic cartridge.28 It rapidly and consistently buffers the LA cartridge to a pH of 7.4. The multidose bicarbonate cartridge allows for the buffering of 20 dental LA cartridges and may be used over a period of 5 days.
Conclusion
Clinical trials17,18 have demonstrated that, done properly-achieving the desired pH (~7.4)-the administration of a buffered local anesthetic provides a more rapid onset of more profound anesthesia, comfortably, and with less post-injection soreness. The authors of this paper recommend that all dental local anesthetic injections using articaine, lidocaine, mepivacaine, and prilocaine be buffered prior to injection.
About the Authors
Mic Falkel, DDS
Founder and Chief Medical Officer, Onpharma Company, Carson City, Nevada; Private Practice, Monterey, California; Adjunct Clinical Professor, University of the Pacific Dugoni School of Dentistry, San Francisco, California
Stanley F. Malamed, DDS
Dentist Anesthesiologist, Emeritus Professor, Ostrow School of Dentistry of U.S.C., Los Angeles, California
References
1. Communication with Septodont NA. Lancaster, PA, May 2016.
2. Communication with Septodont Holding. Saint Maur des Fosses. Cedex, France. May 2017.
3. Malamed SF. Clinical action of specific agents. In: Handbook of Local Anesthesia, 7th edition, Malamed SF, ed. St. Louis: Elsevier; 2020:58.
4. Cannell H, Walters H, Beckett AH, Saunders A. Circulating blood levels of lignocaine after peri-oral injections. Br Dent J.1975;138(3):87-93.
5. Carr RR, Decarie D, Ensom MH. Stability of epinephrine at standard concentrations. Can J Hosp Pharm. 2014;67(3):197-202.
6. Communication with Novocol Pharmaceutical. Cambridge Ontario, Canada. March 24, 2020.
7. Fernandez C, Reader A, Beck M, Nusstein J. A prospective, randomized, double-blind comparison of bupivacaine and lidocaine for inferior alveolar nerve block. J Endod. 2005;31(7):499-503.
8. Carbocaine 3% (mepivacaine hydrochloride, Drug package insert. Cook-Waite. Manufactured for Carestream Health, Inc, by Novocol Pharmaceutical of Canbada, Inc. Cambridge, Ontario, Canada. June 2013.
9. Monheim L. Local Anesthesia and Pain Control in Dental Practice.St. Louis: CV Mosby; 1957.
10. Santa Clara Dental Society. Survey of dental assistants. June 2010.
11. Malamed SF, Falkel M. Buffered local anaesthetics: the importance of pH and CO2. SAAD Dig. 2013;29:9-17.
12. de St Georges J. How dentists are judged by patients. Dent Today. 2004;23(8):96-99.
13. Lai TN, Lin CP, Kik SH, et al. Evaluation of mandibular block using a standardized method. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2006;102(4):462-468.
14. Dal Santo FB, Throckmorton GS, Ellis E 3rd. Reproducibility of data from a hand-held digital pulp tester used on teeth and oral soft tissue. Oral Surg Oral Med Oral Pathol. 1992;73(1):103-108.
15. Jespersen JJ, Hellstein J, Williamson A, et al. Evaluation of dental pulp sensibility tests in a clinical setting. J Endod.2014;40(3):351-354.
16. Alghaithy RA, Qualtrough AJ. Pulp sensibility and vitality tests for diagnosing pulpal health in permanent teeth: a critical review. Int Endod J. 2017;50(2):135-142.
17. Malamed SF, Tavana S, Falkel M. Faster onset and more comfortable injection with alkalinized 2% lidocaine with epinephrine 1:100,000. Compend Contin Educ Dent. 2013;34(spec issue 1):10-20.
18. Kattan S, Lee SM, Hersh EV, Karabucak B. Do buffered local anesthetics provide more successful anesthesia than nonbuffered solutions in patients with pulpally involved teeth requiring dental therapy? A systematic review. J Amer Dent Assoc.2019;150(3):165-177.
19. Vent A, Surber C, Graf Johansen NT, et al. Buffered lidocaine 1%, epinephrine 1:100:000 with sodium bicarbonate (hydrogen carbonate) in a 3:1 ratio is less painful than a 9:1 ratio: A double-blind, randomized, placebo-controlled, crossover trial. J Am Acad Dermatol. 2020: doi: 10.1016/j.jaad.2019.09.088.
20. Best CA, Best AA, Best TJ, Hamilton DA. Buffered lidocaine and bupivacaine mixture - the ideal local anesthetic solution? Plast Surg (Oakv). 2015;23(2):87-90.
21. Gostimir M, Hussain A. A systematic review and meta-analysis of methods for reducing local anesthetic injection pain among patients undergoing periocular surgery. Ophthalmic Plast Reconstr Surg. 2019;35(2):113-125.
22. Afolabi O, Murphy A, Chung B, Lalonde DH. The effect of buffering on pain and duration of local anesthetic in the face: A double-blind, randomized controlled trial. Can J Plast Surg.2013;21(4):209-212.
23. Hinshaw K, Fiscella R, Sugar J. Preparation of pH-adjusted local anesthetics. Ophthalmic Surg. 1995;26(3):194-199.
24. E-mail from Dr. Christopher J Parker, Columbus, Ohio. 11 January 2017. Subject: Precipitate with mepivicaine hydrocholride with 7.5% Sodium Bicarbonate causing trismus.
25. E-mail from Dr. Hassan Mustafa, London, Ontario, Canada. 3 May 2016. Subject: Buffered anaesthetics and the Toronto ODA Convention.
26. E-mail from Dr. James Fetner, Ashboro, NC. 30 September 2019. Subject: Help with 2 patients.
27. Anutra Medical. https://anutramedical.com/dental/. Accessed May 14, 2020.
28. Onpharma Company. Onset Buffering System. https://onpharma.com/. Accessed May 14, 2020.