You must be signed in to read the rest of this article.
Registration on CDEWorld is free. Sign up today!
Forgot your password? Click Here!
Atherosclerotic vascular disease, or atherosclerosis, has been the leading cause of death in the United States for the past century. According to the US Centers for Disease Control and Prevention (CDC),1 someone has a heart attack every 40 seconds, and 630,000 Americans die from heart disease each year. Although major advances in the way that we treat cardiovascular disease have reduced mortality rates for certain patients, these statistics remain largely unchanged. Further progress in treating cardiovascular disease will require that the focus be shifted to prevention. This article outlines a method to improve the outcomes of patients with cardiovascular disease through the use of a cutting-edge preventive healthcare model that is built on collaboration between medicine and dentistry.
Association Between Oral and Systemic Inflammation
New and active research supports the finding that oral inflammation drives arterial inflammation, which subsequently drives the atherosclerotic process. A recent study revealed the pathways of specific bacteria from dental infections and showed how they can directly cause heart attacks and strokes. It concluded that it is necessary to classify periodontal disease as a contributory cause of atherosclerosis.2
There is also a clear association between arterial inflammatory markers (eg, lipoprotein-associated phospholipase A2 [Lp-PLA2]) and periodontal inflammation,3 and researchers have found that treating periodontal disease lowers Lp-PLA2 levels.4 Oral pathogens are significant players in driving the risk of a heart attack. A recent DNA analysis demonstrated that 75% of the arterial thrombi studied had oral pathogens from periapical abscesses and that 35% contained bacteria that cause periodontal disease. These data suggest that as many as 50% of heart attacks may be triggered by an oral infection.5 Although medical and dental providers are treating the same patients with the same diseases, medical providers do not treat periodontal disease; therefore, close collaboration between medical and dental professionals is a prerequisite for preventing cardiovascular events and is imperative for reducing the incidence of heart disease so that it is no longer the leading cause of death in the United States.
The BaleDoneen Method® is a scientifically founded and clinically proven method for the prevention of heart attacks, strokes, and diabetes. This method differs from the current standard of care in that it is based upon the identification of six key elements for assessment, disease determination, and precision disease treatment planning. The focus of the method is to reduce the inflammation in the arterial walls that creates the risk for atherosclerotic disease. According to the latest research, treating the various modifiable causes of inflammation, including periodontal and endodontic disease, attenuates the inflammatory process, which can slow, halt, and even regress atherosclerotic disease.6 A recent study conducted at Johns Hopkins University showed measurable improvements in patients during their first year of treatment by providers who used the BaleDoneen Method. There was a significant decrease in lipid-rich arterial plaques, triglycerides, low-density lipoprotein (LDL) cholesterol, and systolic blood pressure as well as a remarkable increase in high-density lipoprotein (HDL) cholesterol and the calcification of plaque. All of these markers are huge contributors to the reduction and stabilization of arterial plaque.7
HASPC of Central Ohio
The Heart Attack and Stroke Prevention Cen-ter (HASPC) of Central Ohio and Complete Health Dentistry of Columbus are two separate practices located in the same office in Worthington, Ohio. To date, the HASPC of Central Ohio is the only BaleDoneen Method practice in the country offering oral-systemic care and prevention under one roof. The mission of the clinicians is to utilize the BaleDoneen Method to determine the root causes of each individual patient's disease, treat those causes, and reduce the risk of a cardiovascular event.
The protocol employed involves some modification of the BaleDoneen Method because there is both a dentist and a cardiologist working in the same office to optimally manage the various causes of chronic inflammation, including periodontal disease and endodontic disease, which have been shown to drive the inflammatory process.8 The role that dental providers play in reducing oral-systemic inflammation is critical to the collaboration between the medical practice and the dental practice that achieves optimal patient outcomes.
Medicine is embracing the concierge practice model, which seeks to avoid letting insurance dictate the kinds of tests and procedures that are employed for diagnosis, treatment, and prevention. In the concierge model, doctors can spend whatever time is needed to care for their patients and run specialized tests that can detect early stages of disease.
The protocol followed at the HASPC of Central Ohio includes a thorough dental exam, saliva testing, carotid intima-media thickness (CIMT) testing, cone-beam computed tomography (CBCT) scans, genetic testing, and specialized blood and urine testing for inflammation to facilitate an improved understanding of the interrelationship between oral and vascular inflammation. With this information, the clinicians can determine the root causes of the disease, reduce and manage the risks, and calm inflammation in the mouth and vascular system. Heart attacks and strokes are potentially preventable if the root causes of the patient's cardiovascular disease are identified and treated. Periodontal disease, endodontic disease, and obstructive sleep apnea are three of the root causes of cardiovascular disease.9 Dental patients often present with these inflammatory oral diseases while battling inflammatory systemic diseases as well. Systemic conditions, such as diabetes, insulin resistance, hypertension, high cholesterol, and obesity, in addition to genetic predisposition, substantially increase a patient's risk of having a cardiovascular event and make the management of dental disease more challenging.10
The referral flow of the patients at the HASPC of Central Ohio originates from both medical and dental practices, as indicated by the individual patient's needs and based on his or her risk for a heart attack or stroke (See Table 1. Patient Flow Chart). As part of the initial assessment, all medical patients receive a comprehensive dental exam to determine if there is any oral inflammation that could be driving systemic inflammation. The cardiologist will also refer a medical patient for a dental screening if any of the laboratory test results for inflammation are out of the optimal range. Dental patients are referred to the medical practice when they present with risk factors for heart attack, stroke, or diabetes. These risk factors may include a family history of cardiovascular disease or root causes revealed by the oral exam, the CBCT scan, salivary diagnostics, or the sleep test.
Dental Protocol
The dental screening protocol includes a complete dental health evaluation, an objective diagnosis, and meticulous treatment of active disease. In addition to a medical, dental, and family history, the critical data collected in the dental exam includes a thorough oral cancer screening, an occlusal function evaluation, a hard-tissue exam, a full mouth series of radiographs, a CBCT scan, a periodontal evaluation, an oral pathogen saliva test, and a diagnosis determining the stage and grade of the periodontal disease based on the American Academy of Periodontology's periodontal disease classifications.11 The CBCT scan is used not only to diagnose dental pathology but also to identify any evidence of carotid artery calcification or airway restriction.12 The saliva test provides an objective diagnosis based on the identification of the key periodontal pathogens causing the disease. Pathogen identification is critical in determining personalized treatment plans and successful treatment measures.2
The periodontal therapy protocol at the HASPC of Central Ohio is based on a philosophy of testing, treating, and repopulating called the DHEmethod, which was developed by Dental Hygiene Excellence.13 In the protocol, clinicians utilize the objective saliva test results to prepare a personalized and targeted treatment plan, and depending on each individual patient's overall health, the specific oral pathogens present, and whether or not those pathogens are resistant to periodontal therapy, systemic antibiotics and probiotics may be utilized to reduce the most aggressive pathogens (See Table 2. Bacteria Resistant to Periodontal Therapy).14-16
The DHEmethod periodontal therapy protocol uses three phases of treatment to achieve the greatest possible reduction in oral inflammation. Phase I is completed in the dental office through nonsurgical therapy, which includes air polishing with erythritol or glycine and five-tip magnetostrictive instrumentation for scaling and root planing. Phase II consists of continued recare appointments and treatment at home involving the daily use of oral care probiotics to repopulate the biofilm control.17,18 Once a patient demonstrates periodontal stability, phase III maintenance begins with the continuation of oral care probiotics to maximize the effectiveness of treatment. A periodontal medicament carrier for administering a hydrogen peroxide gel may be utilized as well. All periodontal patients also take a nutritional supplement to help reduce their inflammation and heal.
Medical Protocol
Unlike the standard models of medical care, which only permit certain tests to be used to diagnose disease and an average of 9 to 15 minutes of patient-doctor time, the cardiologist at the HASPC of Central Ohio follows a concierge model and spends 3 to 4 hours with each patient for the initial medical assessment. The assessment includes a physical exam and a consultation to review medical and family history, current health issues, diet, and lifestyle. The physical exam includes a CIMT test, specialized blood and urine tests for inflammation, genetic tests, body composition measurements, an electrocardiogram (ECG), a blood pressure evaluation, and a thorough dental exam.
The CIMT test is the first test completed during the physical exam, and it is used to determine if patients have asymptomatic atherosclerosis. CIMT testing provides a measurement of the thickness of the inner layers of the carotid arteries, which is an indicator of atherosclerosis, and assesses for the presence of plaque. The screening measures several areas of the carotid arteries and provides an average measurement.19,20 This test also serves as a baseline, and the doctor will repeat it yearly to measure the effectiveness of interventions.
The prevention plan also utilizes genetic marker tests to establish each patient's risk of atherosclerotic disease as well as to help determine any changes to medication, diet, and lifestyle that may be necessary. The genetic markers utilized in the prevention plan include 9p21, KIF6, HAP2, APOE, Lp(a), and 4q25.
In addition, specialized inflammation tests are critical for measuring inflammation levels and can help identify "hidden" risks that may be overlooked when only standard lipid testing is employed.21 The specialized inflammation tests are processed by Cleveland HeartLaband are repeated quarterly, at a minimum, to monitor the patient's progress.22
The goal of this practice model is to determine a personalized prevention program for each patient, achieve measurable improvement during the first year of treatment, and continue the improvement, stabilization, or regression of the patient's disease over time. BaleDoneen Method providers guarantee the reimbursement of any fees paid during the first year if a patient should have a heart attack or ischemic stroke but only if the patient demonstrates that he or she has made every effort to reduce oral inflammation.
Case Report
The patient, who initially presented to the dental practice, was a 59-year-old male corporate executive with a history of major restorative dental treatment; previously diagnosed periodontal disease; previously diagnosed sleep apnea, which was being treated with an oral mandibular advancement device; a past heavy smoking habit; and a strong immediate family history of heart disease. A review of his medical history revealed untreated hypertension, gout, osteoarthritis, and high cholesterol.
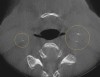
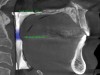
A comprehensive dental exam was performed that included a blood pressure test, an oral cancer screening, intraoral photographs, full mouth radiographs, a periodontal chart, a saliva test, and a CBCT scan. The exam confirmed the presence of active dental decay, periodontitis (ie, stage III, grade B), and areas of calcifications in his carotid artery (Figure 1 through Figure 3).
The dental treatment plan presented included nonsurgical periodontal therapy, composite restorations, and two crowns. The periodontal therapy involved advanced home care tools, a homeopathic healing gel and rinse, an oral care probiotic (ProBioraPro®, ProBiora Health®; alternatives include PRO-Dental®, hyperbiotics® and BioGaia® Prodentis, BioGaia) and systemic antibiotics to target the specific pathogens responsible for the periodontal infection as determined by the saliva test.
Due to a strong family history of cardiovascular disease and the presence of high-risk systemic inflammatory conditions, hypertension, carotid calcifications, and bacteria resistant to periodontal therapy, the patient was referred to the HASPC of Central Ohio for a CIMT test.19
Medical Assessment
The referred dental patient was in the primary stage of disease with no history of diabetes, myocardial infarction, cerebrovascular accidents, or transient ischemic attacks. The examination revealed that his blood pressure was elevated, his body mass index was 28.2, and his 12-Lead ECG results were normal. His CIMT test demonstrated an arterial age of 56; however, he did have a total of 8.6 mm of vulnerable plaque, which put him at a very high risk of experiencing an event, especially considering the presence of high-risk oral pathogens.19
The diagnosis from the initial risk assessment included atherosclerosis, essential hypertension, hyperlipidemia, insulin resistance, obstructive sleep apnea, periodontitis, and low vitamin D. The results of the blood tests and genetic marker tests provided insight for his prevention plan and medical directives.
Medical Directives
Based on all of the test results, the daily medical directives for the patient included starting a low dose prescription of ramipril for his hypertension, increasing his dose of rosuvastatin based on the KIF6 gene for anti-inflammatory therapy, starting a pioglitazone prescription for insulin resistance, starting an 81 mg aspirin regimen, and restarting his vitamin D and nutritional supplementation. In addition, he was directed to complete all recommended dental treatment, including taking his oral care probiotic to reduce the number of high-risk pathogens and repopulate the dental biofilm; undergo a salivary diagnostic posttest, which is critical for patients with high-risk pathogens and plaque burden; continue wearing his obstructive sleep apnea appliance nightly; consume a Mediterranean diet for his APOE genotype; exercise daily; and continue to listen to music for stress management. He was scheduled to return in 6 weeks for a reevaluation and to possibly take new laboratory tests to titrate the medications.
Case Results
The collaboration between the dental and medical providers resulted in a positive patient outcome. The patient completed his intensive active periodontal therapy, and at his 3-month recall visit, he exhibited improvement in the health of his periodontal tissues and a 52% reduction in the burden of periodontal pathogens. One high-risk pathogen (ie, Tannerella forsythia) and three moderate-risk pathogens (ie, Fusobacterium nucleatum, Fusobacterium periodonticum, Parvimonas micra) were still present; however, these are often difficult to reduce. Progressive improvements were anticipated in the next phase of his care, during which he was expected to attend regular maintenance visits with the dental hygienist and use oral care probiotics, homeopathic healing rinses, and hydrogen peroxide gel trays.
By addressing several root causes of disease within a 6-month period, dental therapy reduced the burden of oral pathogens while medical preventive care reduced the presence of systemic inflammation.
Conclusion
Medical and dental professionals have recognized the need for collaboration in the management of the modifiable state of oral disease as it relates to systemic vascular disease to achieve better patient outcomes. It is imperative that future efforts to enhance cardiovascular wellness incorporate oral health evaluations and therapies to control oral disease.
Acknowledgment
The authors would like to acknowledge Amy Doneen, RN, BSN, MSN, ARNP, DNP, medical director of the Heart Attack & Stroke Prevention Center in Spokane, Washington, and co-founder of The BaleDoneen Method, for her contribution to this article.
About the Authors
Eric Goulder, MD
Founder
The Heart Attack and Stroke Prevention Center of Central Ohio
Worthington, Ohio
Fellow
American College of Cardiology
Patti DeMatteis, ASDH, RDH
Co-Owner
Dental Hygiene Excellence LLC
The Heart Attack and StrokePrevention Center of Central Ohio
Worthington, Ohio
References
1. Division for Heart Disease and Stroke Prevention. Heart disease fact sheet. Centers for Disease Control and Prevention web site. https://www.cdc.gov/dhdsp/data_statistics/fact_sheets/fs_heart_disease.htm. Released December 2016. Reviewed August 23, 2017. Accessed September 13, 2019.
2. Bale BF, Doneen AL, Vigerust DJ. High-risk periodontal pathogens contribute to the pathogenesis of atherosclerosis. Postgrad Med J. 2017;93(1098):215-220.
3. Lösche W, Marshal GJ, Apatzidou DA, et al. Lipoprotein-associated phospholipase A2 and plasma lipids in patients with destructive periodontal disease. J Clin Periodontal. 2005;32(6):640-644.
4. Keller DC. Systemic Lp-PLA-2 cardiovascular marker response to direct medication delivery periodontal treatment. Cardiovasc Syst. 2014;2:8. doi: 10.7243/2052-4358-2-8.
5. Pessi T, Karhunen V, Karjalainen PP, et al. Bacterial signatures in thrombus aspirates of patients with myocardial infarction. Circulation. 2013;127(11):1219-1228.
6. Cheng HG, Patel BS, Martin SS, et al. Effect of comprehensive cardiovascular disease risk management on longitudinal changes in carotid artery intima-media thickness in a community-based prevention clinic. Arch Med Sci. 2016;12(4):728-735.
7. Feng D, Esperat MC, Doneen AL, et al. Eight-year outcomes of a program for early prevention of cardiovascular events: a growth-curve analysis. J Cardiovasc Nurs. 2015;30(4):281-291.
8. Teeuw WJ, Slot DE, Susanto H, et al. Treatment of perio-dontitis improves the atherosclerotic profile: a systematic review and meta-analysis. J Clin Periodontol. 2014;41(1):70-79.
9. Loke YK, Brown JW, Kwok CS, et al. Association of obstructive sleep apnea with risk of serious cardiovascular events: a systematic review and meta-analysis. Circ Cardiovasc Qual Outcomes. 2012;5(5):720-728.
10. Martínez-García MA, Campos-Rodríguez F, Catalán-Serra P, et al. Cardiovascular mortality in obstructive sleep apnea in the elderly: role of long-term continuous positive airway pressure treatment: a prospective observational study. Am J Respir Crit Care Med. 2012;186(9):909-916.
11. Tonetti MS, Greenwell H, Kornman KS. Staging and grading of periodontitis: framework and proposal of a new classification and case definition. J Periodontol. 2018;89(Suppl 1):S159-S172.
12. Leonardi Dutra K, Haas L, Porporatti AL, et al. Diagnostic accuracy of cone-beam computed tomography and conventional radiography on apical periodontitis: a systematic review and meta-analysis. J Endod. 2016;42(3):356-364.
13. Dental Hygiene Excellence. The DHEmethod. Dental Hygiene Excellence web site. https://www.dhemethod.com/. Accessed September 16, 2019.
14. Petersilka GJ, Ehmke B, Flemmig TF. Antimicrobial effects of mechanical debridement. Perio 2000. 2002;28:56-71.
15. Oral Systemic Health News Network. Oral bacteria become therapy resistant. Oral Systemic Health News Network web site. http://oshnewsnetwork.com/2014/08/27/oral-bacterium-becomes-therapy-resistant/. Published August 27, 2014. Accessed October 23, 2019.
16. Slots J, Ting M. Systemic antibiotics in the treatment of periodontal disease. Periodontology 2000. 2002;28(1):106-176.
17. Zahradnik RT , Magnusson I, Walker C, et alPreliminary assessment of safety and effectiveness in humans of ProBiora3, a probiotic mouthwash. J Appl Microbiol. 2009;107(2):682-690.
18. Gordon J. Christensen Clinicians Report.Clinicians Report November 2018, Volume 11 Issue 11. Clinicians Report web site. https://www.cliniciansreport.org/products/dental-reports/clinicians-report-november-2018-volume-11-issue-11.php. Accessed September 16, 2019.
19. Nicolaides A, Panayiotou AG. Screening for atherosclerotic cardiovascular risk using ultrasound. J Am Coll Cardiol. 2016;67(11):1275-1277.
20. Sun J, Zhao XQ, Balu N, et al. Carotid plaque lipid content and fibrous cap status predict systemic CV outcomes: the MRI substudy in AIM-HIGH. JACC Cardiovasc Imaging. 2017;10(3):241-249.
21. Myhre PL, Lyngbakken MN, Tveit SH, et al. Cardiac imaging and circulating biomarkers for primary prevention in the era of precision medicine. Expert Review of Precision Medicine and Drug Development. https://doi.org/10.1080/23808993.2019.1660162.
22. Cleveland HeartLab. Inflammation testing fromCleveland HeartLab. Cleveland HeartLab web site. http://www.knowyourrisk.com/. Accessed September 16, 2019.