You must be signed in to read the rest of this article.
Registration on CDEWorld is free. Sign up today!
Forgot your password? Click Here!
The specialty of endodontics is constantly evolving. It has been said that root canals are not what they used to be. Perhaps the greatest transformation is occurring within the realm of technology. New advancements in technology have provided practitioners with a better understanding of the complex anatomies found in root canal systems, which can provide new insights into how endodontists can most effectively treat them.
Since its founding in 1990, Amarillo Endodontics has provided care based on a simple guiding principle, one that is revealed in the practice's slogan: "With your comfort in mind… always." This commitment to comfort extends beyond simply providing a physically comfortable experience for patients. The clinicians recognize that patients often come to the practice with some trepidation, knowing root canal treatments have developed a reputation for being unpleasant experiences. Therefore, the clinicians have been motivated to work more diligently, seeking to provide every patient with the highest level of care and fostering peace of mind before, during, and after a patient's time in the chair. Whenever they weigh the possible directions in which to take the practice, they look to the practice's guiding principle and seek to offer comfort to patients however possible.
This philosophy extends to the integration of technology. Although the authors have always considered themselves to be early adopters of worthy technology, they have never invested in any technology for the sake of technology itself without asking themselves the following questions:
• Most importantly, is it safe and effective for patients?
• Does it make the practice better?
• Does it make the practice more efficient?
• Does it make the practice more productive?
• Does it set a new standard in endodontics?
When the clinicians discuss the various ways that investing in appropriate technology has led to better experiences for patients, they do so through the lens of the endodontic triad (Figure 1). The endodontic triad focuses on the intersection between instrumentation, disinfection, and obturation and their cumulative effect on the patient experience.1
Improving Instrumentation: The Benefits of Technology
It has been more than 100 years since Walter Hess, MD, DDS, injected over 3,000 teeth with vulcanized rubber and demonstrated in numerous examples the unique nature of the root canal system.2Endodontists understand that root canals are far more complex than a simple tube or funnel. They are instead an intricate system of webbing, fins, and anastomoses, and when they are infected with bacteria, they must be thoroughly cleaned and disinfected so that symptoms can become manageable and the tooth, as well as the patient, can return to a healthy, functional state. Endodontists have also come to realize that instrumentation alone is insufficient to deliver this cleaning and disinfection.
This understanding was borne out as endodontic practices, including that of the authors, began integrating cone-beam computed tomography (CBCT) technology into their diagnostic process. CBCT technology provides a way to visualize, in 3 dimensions, complex anatomies and periradicular pathologies. CBCT has allowed the ability to more thoroughly diagnose and treat cases. For the first time, endodontists have been able to see complex anatomies in all dimensions, rather than in the simple 2-dimensional (2D) view from a conventional periapical radiographic image.3,4
Thorough endodontic diagnosis involves the patient's chief complaint, medical and dental history, and clinical and radiographic examination.5 Accurate data lead to better treatment decisions and potentially more predictable outcomes.6 In May 2015, an updated joint position statement of the American Association of Endodontists and the American Academy of Oral and Maxillofacial Radiology was published. Based on recommendation 2 of the CBCT Position Statement, limited fields of view (FOV) CBCT should be considered the imaging modality of choice for diagnosis in patients who present with contradictory or nonspecific clinical signs and symptoms associated with untreated or previously endodontically treated teeth.7Limited FOV is the most ideal for use in endodontic applications because it is capable of providing sufficient images at a low radiation dose.5 CBCT imaging has the capability of detecting periapical pathology before it is apparent through radiography.8 Findings of clinical studies showed that periapical radiolucency was detected in 20% of cases using radiographs, compared with 48% using CBCT.9
The effective radiation dose for patients when using CBCT is higher than conventional 2D radiography, and the benefit to the patient must outweigh any potential risks, especially in children.10,11However in many instances, several angled 2D preoperative images may be required to obtain the same information that a single CBCT can provide. Several studies have evaluated the use of CBCT in endodontics and found that its use overcomes many of the limitations of periapical radiography.12-14 The value of CBCT in endodontics has been well established, but its use should be determined on an individual basis. Dentists should use referral to an endodontist as part of the dental team because endodontists use the latest diagnostic imaging and techniques to ensure the patient benefits from their diagnostic and treatment-planning expertise.5
As CBCT technology has continued to improve understanding of the intricacies of the root canal system, it has also underscored the idea that Dr. Hess first posited in 1917: this system is too complex to be truly disinfected through instrumentation alone.2 Figure 2, from research carried out by Ove A. Peters, DMD, PhD, amply demonstrates the shortcomings of instrumentation alone.4,15 The red in the image represents areas that have been touched by instruments, and the green represents areas that have not been touched. Inability to reach all the complex anatomy in the root canal system is why cleaning and disinfection are central to the endodontic process.
Delivering Disinfection and Debridement: Integrating New ADVANCEMENTS
Because bacteria are responsible for endodontic disease,16 to achieve optimal outcomes, bacteria must be eliminated or significantly reduced to a level that ensures patients are able to heal. The authors also recognize that sodium hypochlorite is the only irrigant currently available that adequately debrides and disinfects the root canal.16 In combination with ethylenediaminetetraacetic acid (EDTA), sodium hypochlorite has been shown to optimize intracanal cleanliness suitable for success.17,18
It is also known that, for irrigants to effectively reach the apical third, the endodontist must prepare a continuously tapering funnel within the canal space, taking care not to overprepare. Any coronal interferences must be removed so that straight-line access to the apex of the tooth can be achieved. This process allows the irrigants to penetrate the apical third of the canal if a minimum size of at least a #30 instrument has been used.19 Conventional irrigation using a syringe is called positive pressure irrigation, meaning that the irrigants are placed into the access opening and into the canal, to essentially flush debris from the canal. The effectiveness of this passive irrigation is limited because the static reservoir of irrigants in the apical third prevents treatment fluids from fully reaching all areas of the canal anatomy. Full penetration, particularly in the apical areas, is restricted unless the apical area is larger than normal.20-23
A contrasting method of irrigation, called active irrigation, involves fluid dynamics. In this method, an energy source is used to move the irrigants throughout the canal space, which ensures better and more thorough disinfection and debridement. There are two basic methods of activating these fluids, sonic or ultrasonic. Regardless of which technique is used, the canals must be generously shaped to allow deeper penetration into canal areas. Here again, instrumentation imposes limits on the treatment's efficacy. After the tip of the instrument engages any portion of the canal, the activation becomes neutralized.20-23
While efforts to improve on the irrigation process, and consequently provide better debridement and disinfection, have continued to move forward, an apical negative pressure irrigation system has been introduced. This technology, available commercially as the EndoVac™ system from Kerr (kerrdental.com), has helped increase the potential for disinfection in the apical third with minimal extrusion. More recently, technology that employs advanced fluid dynamics and broad-spectrum acoustic energy has increased the endodontist's ability to debride and disinfect the entire root canal, all the way into the apical third, with minimal need for instrumentation. This technology, available commercially as the GentleWave® System from Sonendo (sonendo.com), uses a unique mechanism of action. In the first stage of the process, procedure fluids are degassed, and their concentration is adjusted to the optimal level. This approach is in contrast with needle irrigation, where gas bubbles in the fluid may create vapor lock and actually inhibit the ability to reach the entire root canal system.20-23
The fluids are then circulated through the entire root canal system, constantly being refreshed throughout the process. During the next stage, useful cavitation and vortical flow are induced for maximum debridement and dissolution. Tissue dissolution occurs in approximately 7 to 8 minutes. Because this advanced fluid dynamics and broad-spectrum acoustic energy system uses minimal instrumentation, dentin is preserved. Consequently, internal tooth structures are able to be maintained, and the risk of treatment failure over time is greatly lessened.20-23
Two studies illustrate this system's potential for improved healing times.20,24 The first study was a 12-month follow-up on 75 patients, with an overall success rate of 97.3%. A total of 96.2% of patients had no postoperative discomfort. For the 3.8% of patients who experienced pain, it resolved after 2 days. None of these patients experienced pain at 14 days or 6 months, or even at 12 months.24 The second study was a follow-up on 45 patients, with a success rate of 97.7%. The teeth of these patients had complete resolution of symptoms; no patients experienced moderate or severe pain at 2, 7, or 14 days.20
Optimizing Obturation: Employing Best Practices
The third tenet of the endodontic triad, obturation, is the area that has changed the least. In the practice, it is believed that the vertical condensation of warm gutta-percha allows the ability to capture and seal the complex anatomy that is present in every tooth treated.
Advances in Technology and the Endodontic Process
As stated above, the authors' practice has been an early adopter of new technology. With all the advancements that have been incorporated into the practice since its founding nearly 30 years ago, treatment has evolved accordingly, although some aspects have remained consistent.
At the practice, treatment begins with the removal of all caries during the access. Any gingival overgrowth-for example, into a mesial box-is addressed at that time. Proper hemostasis is achieved. Next, all the canals are located. The authors frequently use the Dentsply Sirona ProTaper® SX instrument (dentsplysirona.com; comparable to EdgeEndo® and EdgeTaper™ Platinum, EdgeEndo, edgeendo.com) to allow initial access into the canal spaces and then use an apex locator to establish working length.
Typically, the clinicians have an armamentarium of several files, which they use throughout the procedure, including an .02 instrument, an .04 instrument, and a variably tapered rotary instrument. They instrument from 1.0 mm to 1.5 mm short of working length. The outer tooth surface or crown is cleaned with alcohol and completely dried, making sure saliva is controlled. Sonendo SoundSeal™ (comparable to Kool-Dam™, Pulpdent, pulpdent.com), which is a light-cure resin, is used with a matrix to establish a platform on which the Procedure Instrument is placed.
The technology the clinicians employ has several software selections, depending on whether they are treating a necrotic or a vital tooth, or performing a retreatment. Finally, the clinicians dry the tooth and, even though the canal spaces are smaller, their principles of obturation remain the same.
The authors are now asking patients to return in 3 months for follow-up. In the past they would normally schedule a 6-month follow-up, but with the reports of reduced healing times due to incorporation of the new technology, they felt it would be beneficial to assess healing much sooner.
Technology Case Studies
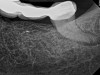
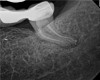
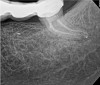
In the first case study, a young female patient was told she had a tooth (tooth No. 2, Figure 3) that should be extracted due to extensive bone loss. Using CBCT, the clinician was able to identify a large lateral canal within the palatal root. Despite the bone loss, the patient was eager to save her tooth. He offered to treat the tooth with the broad-spectrum acoustic technology. As shown in Figure 4, the preparation space was much smaller, which he was able to obturate efficiently. In addition, the small pinpoint of sealer in the middle of the palatal root indicated that the palatal lateral canal had been addressed (Figure 5). In the clinician's opinion, this area was likely the primary source of much of the bone loss.
Figure 6 through Figure 8 demonstrate that, 5 months after the procedure, complete healing had occurred, notably on the distal, where the probing had resolved to 2 mm. The patient then had a crown placed by her general dentist. Given her positive experience with the technology, she was eager to return as needed for continued follow-up.
The second case study is that of a healthy 88-year-old woman who presented with significant bone loss on the mesial and apical aspect of tooth No. 18, which would suggest potentially a vertical fracture in the tooth (Figure 9 and Figure 10). The clinician had initially recommended extraction, which they informed the patient would likely be the best course of action, especially given that she had plenty of bone anterior to the tooth to place implants. When the recommendation of extraction was made to the referring dentist, he had some resistance because both he and the patient were interested in saving the tooth. Although the clinician initially stood firm on the recommendation, he received a call from the general dentist about a month later. He further expressed their desire to save the tooth, and he asked if the endodontist thought the new technology, the GentleWave Procedure, could be a solution. The informed consent was obtained and the patient was scheduled for treatment. Because the canal was quite calcified apically, a defined working length could not be determined. Obturation was performed using warm vertical condensation of gutta-percha.
As indicated in Figure 11, the mesial aspect of the distal canal was never touched by instruments, yet he was able to clean, evidenced by the postoperative image. In the past, a case with this level of difficulty would have required at least two appointments, with an interim medication of calcium hydroxide, but the case was treated in a single-visit appointment. As observed 7 months later (Figure 12), the patient returned completely asymptomatic, and complete bone healing had occurred that exceeded initial expectations.
Conclusion
Staying technology-driven not only provides endodontists with better ability to diagnose and treat patients, but also communicates that a practice is on the leading edge, which in turn provides the practice with a clear differentiator in the eyes of patients and referring practices. As technology advances, often secondary benefits extend beyond the primary function. With the advanced fluid dynamics and broad-spectrum acoustic technology of the GentleWave System, for example, the authors have seen very little to no postoperative discomfort and fewer postoperative check appointments. With fewer patients returning, the office has greater availability for emergency patients. With minimal need for pain management, the practice has also eliminated the need for opioids completely, and the need to prescribe nonsteroidals is greatly reduced.
In addition, the integration of new technologies can enhance efficiency, productivity, and outcomes, and it can also lead to a more rewarding everyday experience for the practitioner. Each day, for example, the authors see that this technology results in thorough debridement and disinfection of entire canal spaces in a way that they were not able to experience before-which has actually even brought a new element of fun to day-to-day activities. As noted earlier, it has been said that root canals are not what they used to be-that we are in a time of technology evolution-though perhaps in this case, a breakthrough technology revolution, and in the authors' practice, that is especially evident.
About the Authors
James C. Douthitt, DDS, MS, FACD
Kirk A. Coury, DDS, MS, FICD, FACD
Private Practice
Amarillo, Texas
References
1. Cohen S, Hargreaves KM. Pathways of the Pulp, 9th ed. St. Louis, MO: Mosby; 2006.
2. Hess W. The Anatomy of Root-Canals of the Teeth of the Permanent Dentition.New York, NY: William Wood and Co.; 1925.
3. Khademi JA, Carr GB, Schwartz RS, Trudeau M. Advanced CBCT for Endodontics: Technical Considerations, Perception, and Decision-Making. Hanover Park, IL: Quintessence Pub Co; 2017.
4. Peters OA, Schönenberger K, Laib A. Effects of four Ni-Ti preparation techniques on root canal geometry assessed by micro computed tomography. Int Endod J. 2001;34(3):221-230.
5. Fayad MI. The impact of cone beam computed tomography in endodontics: a new era in diagnosis and treatment planning. American Association of Endodontists. Endodontics: Colleagues for Excellence.Spring 2018.
6. Liang YH, Li G, Wesselink PR, Wu MK. Endodontic outcome predictors identified with periapical radiographs and cone-beam computed tomography scans. J Endod.2011;37(3):326-331.
7. Special Committee to Revise the Joint AAE/AAOMR Position Statement on Use of CBCT in Endodontics. AAE and AAOMR joint position statement: use of cone beam computed tomography in endodontics 2015 update. Oral Surg Oral Med Oral Pathol Oral Radiol. 2015;120(4):508-512.
8. de Paula-Silva FW, Wu MK, Leonardo MR, et al. Accuracy of periapical radiography and cone-beam computed tomography scans in diagnosing apical periodontitis using histopathological findings as a gold standard. J Endod.2009;35(7):1009-1012.
9. Patel S, Wilson R, Dawood A, Mannocci F. The detection of periapical pathosis using periapical radiography and cone beam computed tomography - part 1: pre-operative status. Int Endod J.2012;45(8):702-710.
10. Farman AG, Farman TT. A comparison of 18 different x-ray detectors currently used in dentistry. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2005;99(4):485-489.
11. Farman AG. ALARA still applies. Oral Surg Oral Med Oral Pathol Oral Radiol Endod.2005;100(4):395-397.
12. Patel S, Durack C, Abella F, et al. Cone beam computed tomography in endodontics: a review. Int Endod J.2015:48(1):3-15.
13. Cotton TP, Geisler TM, Holden DT, et al. Endodontic applications of cone-beam volumetric tomography. J Endod.2007;33(9):1121-1132.
14. Nair MK, Nair UP. Digital and advanced imaging in endodontics: a review. J Endod.2007;33(1):1-6.
15. Peters OA. Current challenges and concepts in the preparation of root canal systems: a review. J Endod.2004;30(8):559-567.
16. Siqueira JF Jr, Rôças IN. Clinical implications and microbiology of bacterial persistence after treatment procedures. J Endod.2008;34(11):1291-1301.
17. Byström A, Sundqvist G. The antibacterial action of sodium hypochlorite and EDTA in 60 cases of endodontic therapy. Int Endod J.1985;18(1):35-40.
18. Torabinejad M, Handysides R, Khademi AA, Bakland LK. Clinical implications of the smear layer in endodontics: a review. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2002;94(6):658-666.
19. Chow TW. Mechanical effectiveness of root canal irrigation. J Endod.1983;9(11):475-479.
20. Sigurdsson A, Garland RW, Le KT, Rassoulian SA. Healing of periapical lesions after endodontic treatment with the GentleWave procedure: a prospective multicenter clinical study. J Endod.2018;44(3):510-517.
21. Plotino G, Pameijer CH, Grande NM, Somma F. Ultrasonics in endodontics: a review of the literature. J Endod. 2007;33(2):81-95.
22. Salzgeber RM, Brilliant JD. An in vivo evaluation of the penetration of an irrigating solution in root canals. J Endod.1977;3(10):394-398.
23. Mathew J, Emil J, Paulaian B, et al. Viability and antibacterial efficacy of four root canal disinfection techniques evaluated using confocal laser scanning microscopy. J Conserv Dent. 2014;17(5):444-448.
24. Sigurdsson A, Garland RW, Le KT, Woo SM. 12-month healing rates after endodontic therapy using the novel GentleWave System: a prospective multicenter clinical study. J Endod.2016;42(7):1040-1048.