You must be signed in to read the rest of this article.
Registration on CDEWorld is free. Sign up today!
Forgot your password? Click Here!
Though esthetic dentistry is largely considered to be a fairly modern innovation, the early history of esthetic restorative materials can be traced back to 1843 with the discovery of acrylic acid by Josef Redtenbacher, a German chemist.1 By 1900, this simple compound led to the synthesis of methacrylic acid and, more importantly, its methyl ester, methyl methacrylate (Figure 1). Like the monomers found in most modern resin composites, liquid methyl methacrylate can be induced via free radical initiation to polymerize at its C=C double bond into a solid polymer referred to as poly (methyl methacrylate). Poly (methyl methacrylate) found its first use in dentistry in the early 1930s in indirectly processed dental laboratory materials such as denture bases and later for indirect tooth-colored filling materials.2
Polymers are typically large molecules composed of repeating smaller subunits called monomers. Although there is no absolute requirement as to the physical states of a monomer or polymer, monomers used in dentistry are normally liquids that transform into a solid polymer during a chemical reaction called “polymerization.” The polymerization reaction typically requires some type of catalyst system or infusion of heat or energy that alters the monomer molecules to an unstable thermodynamic or electronic state, such as that of a free radical. Once destabilized, they polymerize to reach a more stable electrochemical state. The extent to which the monomers can be transformed into a polymer is called the “degree of conversion.” Thus, if all available monomer molecules could be induced to polymerize, there would theoretically be 100% degree of conversion. For current dental polymers, the degree of conversion is usually much less than 100%. “Polymerization shrinkage” occurs when the molecules of a liquid monomer take up less space as they change from the liquid state into a solid polymer state.
More History and Development
When the benzoyl peroxide-tertiary amine initiator reaction was discovered, it allowed methyl methacrylate-based materials to cure at room or oral temperatures and paved the way for using them in direct filling restorations. Unfortunately, direct restorations made with methyl methacrylates had a disappointing clinical performance, including high wear rates, high incidence of secondary decay, poor color stability, and adverse pulpal reactions. Two deterrents to using methyl methacrylates for direct restorations are their low conversion rate, which leads to a high content of unset residual monomer, and the fact that they have no real adhesion or watertight seal to tooth structure. In 1955, Buonocore published his now famous paper that suggested the acid treatment of enamel to improve the adhesion of direct acrylic fillings.3 Despite improvements, the majority of observed clinical problems can be directly attributed to or have been influenced by the very high polymerization shrinkage of methyl methacrylates. Unfilled methyl methacrylate monomer has an unprecedented shrinkage of ~25% during setting. The incorporation of fillers into the monomers lowers overall shrinkage to about 7% (although the monomer to polymer shrinkage remains the same). This 7% shrinkage is still clinically unacceptable, especially in the absence of a sound marginal bond or seal.
In response to the compromised clinical performance of methyl methacrylates, Bowen began investigating the use of epoxy resins4 in dentistry. Epoxy resins draw their name from the fact that they contain three member epoxide rings where two ring members are carbon atoms and one member is an oxygen atom (Figure 2, see glycidyl methacrylate). The epoxide functional groups are somewhat unstable and prone to ring opening, which allows polymerization with other molecules. Moreover, ring opening polymerization almost always results in a lower polymerization shrinkage than linear polymerization, which occurs in methyl methacrylate. When the epoxide base material is mixed with polyamine hardener, an autocuring polymerization reaction is initiated. Epoxy resins held early promise for dentistry because they cure at room temperatures with little volumetric shrinkage, can be loaded with inert fillers, and show good adhesive properties to most solid surfaces. Though they proved useful for some indirect dental applications, epoxy resins were ultimately abandoned because of questionable biological compatibility and because they set too slowly to be used for direct restorations. In 1956, Bowen synthesized an important new monomer that was a reaction product of bisphenol A and glycidyl methacrylate, which became known as bis-GMA and led to the development of the modern composite resin. Bis-GMA ultimately proved highly useful in dentistry due to its many clinical and technical advantages over acrylics and epoxy resins. As a result of the molecular length between the acrylate groups, it polymerized rapidly at room temperature with moderately low overall polymerization shrinkage. It could also be induced to polymerize with ultraviolet (UV), photo, or chemical initiators. As a very large molecule, it has a low volatility and produces a strong, rigid polymer when set. However, bis-GMA has a fairly high viscosity, which limits the incorporation of reinforcement fillers and makes the unset composite paste thick and difficult to handle clinically. To overcome this, formulations made with bis-GMA usually must be diluted with other dimethacrylate comonomers, which are smaller and of lower molecular weight. Examples include HEMA (hydroxyethyl methacrylate), TEGDMA (triethylene gylycol dimethacrylate), and EGDMA (ethylene glycol dimethacrylate). Unfortunately, these lower molecular weight comonomers have higher volumetric shrinkages than bis-GMA. For example, the most commonly used comonomer, TEGDMA, has a polymerization shrinkage of ~15%. Dilution monomers can also be used to modify the hydrophilicity and handling properties of the composite resin and significantly increase the amount of filler that can be incorporated, but most tend to increase overall polymerization shrinkage. Thus, there must be a delicate balance between the various amounts of each monomer.
As the clinical usage of direct esthetic restorative materials advanced, the overall importance of polymerization shrinkage and shrinkage stresses was recognized. Bis-GMA itself has a reported volumetric shrinkage of about 5%.5 With the incremental addition of higher shrinking dilution monomers, early macro- and microfilled composites could have had a total volumetric shrinkage as high as 7.1%.6 Improvements in more recent products have successfully reduced this value; however, including both conventional hybrid and flowable composite resins, modern methacrylate-based composites still have polymerization shrinkage values ranging from about 1.78% to 5.7%.7 Depending on the bond strength of the interface between composite and tooth, a shrinkage of this magnitude can readily lead to clinical problems such as marginal gap formation and leakage, debonding at the restoration/tooth interface, cuspal deflection, and microfractures of the tooth structure surrounding the outline form of the cavity.
Strategies for Reducing Polymerization Shrinkage
Reducing Monomer Percentage through the Addition of Inorganic Fillers
Polymerization shrinkage is normally measured and reported as a volumetric change. It occurs because the monomer molecules in the liquid state are spaced at Van der Waals distances, but during polymerization into the solid state, covalent bonds are formed, reducing interatomic distances. Solid fillers, conversely, maintain a constant volumetric dimension during the polymerization reaction. As such, one of the earliest strategies was simply to reduce the total amount of monomer content through the addition of solid fillers. It is well understood that the introduction of inorganic fillers can improve clinical performance by increasing durability and reducing wear of the mostly organic resin monomers, but more significantly, as filler density increases, overall polymerization shrinkage decreases because shrinkage is confined exclusively to the monomer phase.
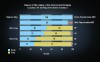
Figure 3 shows graphically how 50% and 70% filler additions can dramatically reduce shrinkage as compared with a cured monomer resin alone. Assuming a 10% volumetric shrinkage for the monomer phase, the addition of a 50% filler fraction results in a 50% reduction in shrinkage for an overall shrinkage of 5%, while a 70% filler fraction reduces it to 3%.
Utilizing Multiple-Sized Filler Particles
Total filler loading is also dependent on the “packing” properties of the solid fillers. To achieve the greatest density or loading of irregularly shaped filler particles, an assortment of particle sizes and shapes is needed where progressively smaller sized particles can fill the interstices between the larger particles (Figure 4). This has fostered the growth of hybrid composites, which utilize multiple size fillers to achieve this objective. As will be discussed in the next section, the addition of non-bonded, micro-, or nanofillers may also help reduce polymerization stresses.8,9 However, as the quantity of micro- and nanofillers increases, the overall viscosity of the final composite product is dramatically increased and some of the physical properties may be adversely affected. Thus, their amounts must always be optimized.
Utilizing Prepolymerized Filler Particles
Another common approach that has been applied to reducing shrinkage is the use of “prepolymerized fillers.” These specialized fillers are manufactured by adding inorganic micro- or nanofillers at very high concentrations to a resin monomer under conditions of high heat and pressure. Once cured, the resultant blocks are ground into macrosized filler particles, which typically range in size from about 30 µm to 65 µm for most microfilled and nanofilled composite resins10 (Figure 5). The restorative material is made up by dissolving a heterogenous mixture of these larger macrosized filler particles and individual microfillers in a quantity of uncured monomer. This significantly reduces the amount of uncured, free monomer that can contract during polymerization, thus decreasing overall shrinkage. Yet another benefit is the reduction in the interparticle distances, which increases frictional contact between particles during polymerization of the resin monomer (Figure 6).
Synthesis and Utilization of Low-Shrinking Monomers
Changes in filler configuration offered only limited reductions in polymerization shrinkage. Researchers, therefore, next began to examine ways to modify the matrix and monomer chemistry. Of early interest were non-shrinking or expanding monomer/polymer systems. In 1975, Bailey proposed using bicyclic monomers, where both of the rings opened during polymerization.11 Thus, the shrinkage for each Van der Waals distance converted to a covalent bond was offset partially or entirely by the opening of two cyclic rings. This is capable of leading to no change in set volume or possibly even slight expansion. As was pointed out previously, “ring opening polymerization” almost always results in less setting shrinkage than simple “linear addition polymerization.” Because they are chemically compatible with methacrylate chemistry, the group of “bicyclic” monomers that has received the most attention is the spiro orthocarbonates (SOCs). The technical challenge of using SOCs in clinical resin composites is that they are mainly crystalline at room temperature and somewhat unreactive. Since some SOCs can copolymerize with methacrylates, Thompson and Bailey attempted to overcome their limitations by grinding them into fine particles and creating a slurry of the crystalline SOCs with the traditional liquid bis-GMA monomers.12 However, the SOCs and the traditional monomers did not cure simultaneously, leading to a high percentage of unreacted crystalline SOC in the final polymerized resin. Additionally, they were only able to achieve a slight reduction in the total polymerization shrinkage. Later work by Stansbury and Bailey utilized SOCs with lowered melting points and greater compatibility with standard dental monomers. Unfortunately, they were still unable to show anything other than modest improvements in polymerization shrinkage with copolymers as high as 33% SOC by weight.13,14
In 2007, an interesting new ring opening monomer was introduced called Silorane (3M ESPE), which is named for the two chemical subunits that make up the molecule: siloxanes and oxiranes. Siloxanes provide an inorganic backbone of alternating silicon and oxygen atoms (–Si-O-Si-O-) that has either a hydrogen or an organic side group attached to the Si atoms. Siloxanes can be branched, unbranched, or cyclic and are best known for imparting hydrophobic properties. In Silorane, the siloxane backbone is cyclic and the organic side groups are oxiranes. Oxiranes are three member rings consisting of two carbons and one oxygen, which is the simplest epoxide, and as pointed out previously are members of the epoxy resin group. Polymers formed from oxiranes are known for low shrinkage and excellent physical properties. Siloranes polymerize via cationic ring opening of the oxirane groups, leading to very minimal overall shrinkage. According to the manufacturer, the volumetric shrinkage obtainable with the silorane-based composite is approximately 0.9% when evaluated by the bonded disc method, also known as the Watt’s method.15 This is significant because it is the first time a commercially available direct composite has reported a shrinkage factor < 1. However, when using other generally accepted test methods, the actual polymerization shrinkage may not be significantly lower than that possible with more conventional resin-based composites. Also, Silorane chemistry is still new,* so no long-term clinical data is available as compared with methacrylates. It also requires at least twice the polymerization time as methacrylate resin for a 2-mm increment and has poor compatibility with the methacrylate-based adhesives and composite products; therefore, it requires its own proprietary adhesive and related complementary products. Most importantly, however, lowered polymerization shrinkage does not necessarily translate into a lowered stress applied to the tooth or higher bond strengths, as will be discussed in the section on polymerization stress below.
*Editor's note: Since the original publication of this article, 3M has changed the chemistry of its low-shrink composites from Silorane ring opening composites to addition fragmentation monomer (AFM) and aromatic urethane dimethacrylate (AUDMA).
Reducing the Total Number of Covalent Bonds Formed
With only limited success in the use of ring opening monomers, recent efforts to reduce shrinkage have focused on yet another strategy. Since volumetric shrinkage has been linked to molecular sites where there is a conversion of an electrostatic Van der Waals interaction to a covalent bond, it stands to reason that reducing the total number of such conversions should effectively reduce the total volumetric shrinkage. This can be accomplished by utilizing monomer molecules with higher molecular weights, which also typically occupy a larger volume of space. With fewer total monomer molecules to occupy the same potential space compared to smaller monomers, there is a reduction in the number of covalent bonds formed per unit space. This will ultimately reduce the total polymerization shrinkage and shrinkage stress.
An example of this strategy is found in Kalore™ (GC America Inc.), which was introduced in 2009. Kalore is 82% filled by weight and has a reported volumetric shrinkage of approximately 1.7% (by mercury dilatometer). It replaces the bis-GMA monomer with DX-511, a new lower shrinking monomer chemically related to urethane dimethacrylate (UDMA) that has been developed by Dupont. Thus, Kalore is able to retain full methacrylate compatibility. DX-511 has a much higher molecular weight (895) than bis-GMA (513) and has both stiff and flexible segments in the monomer, the latter of which reduces the monomer viscosity, permitting lower amounts of diluent monomers to be used in the formulation.
Clinical Significance
Polymerization Shrinkage Vs. Polymerization Stress
Based on the previous information presented, one might conclude that a reduction in the volumetric/polymerization shrinkage of the restorative material would almost always be accompanied by a reduction in the stress applied to the tooth. However, polymerization shrinkage and its associated stress do not always parallel one another. Polymerization stress is a local physical state, not a basic material property. As such, its final value is dependent upon the system geometry and boundary conditions.16 Some of the moderating factors are physicochemical, and some are clinical. Polymerization stress development seems to result from a complex interaction of cavity geometry, volumetric shrinkage, degree of conversion, reaction kinetics, and viscoelastic properties of the restorative material.17 To understand this, consider the dynamics of the curing reaction, as follows.
At the very initiation of polymerization, the monomers are all in a fluid or “sol state,” and the composite resin behaves like a viscous solution. During active polymerization, liquid monomers are gradually converted to solid polymer with an accompanying reduction in volume. However, as long as there is still a sufficient quantity of unset, liquid monomer readily available, any polymerization shrinkage of restorative composite within the dental cavity can be partially offset by the flow of unset monomer, ie, as the set material contracts, the gap is immediately filled with unset fluid material. This is referred to as the pre-gelation phase. No significant stress builds up within the restorative material itself and none is applied to the walls of the cavity. However, once the majority of the liquid monomer is consumed by the polymerization reaction, the “gel phase” is initiated. Continued shrinkage can no longer be offset by free monomer, and stress begins building up internally within the restorative material. If the restoration is adhesively bonded to a wall or walls of the tooth, this stress can also transfer from the restoration to the tooth. Depending on the magnitude of the stress, this may result in a deflection of the cuspal walls, an adhesive failure of the bond between tooth and restoration, or a cohesive failure (fracture) within the adhesive layer, the restorative material, or the tooth itself. All of these adverse event results may shorten the life of the restoration and the tooth.
Determinants of Polymerization Stress
Cavity Geometry
One key factor in how much polymerization stress will be transferred “to the tooth” by the restorative material is the cavity geometry. More specifically, it is only at the sites where the restoration interfaces with and is adhesively bonded to the tooth that the stress can be transferred. Restoration surfaces that have no contact with or are not bonded to the cavity walls can deflect during polymerization, allowing for internal dissipation of stress forces (ie, confined only to the restorative material). If none of the restoration’s surface area is bonded to the tooth, it can shrink and move freely within the cavity confines. However, if a single cavity wall is bonded, stress will be applied to the tooth at that one site and is dissipated at the others. If two walls are bonded, stress is applied to the two sites, and so on. Since most direct esthetic restorations are adhesively bonded, the exact cavity geometry and number of bonded and nonbonded surfaces becomes a key factor to polymerization stress. A convenient way to describe this is the ratio of the bonded walls to the nonbonded walls, which provides a quantifiable measure of where and how much stress can be applied directly to the tooth and cavity. This ratio has been referred to as “Configuration Factor” or “C-Factor” for short18:
Bonded Cavity Walls
-––––––––––––––––––––––––––– = Configuration Factor = C-Factor
Nonbonded Cavity Walls
Cavities with a high C-Factor would tend to have higher potential stress than those with a lower number. Though C-Factor numerically uses simple integers representing cavity walls because it is an easy value for the clinician to assess, an important assumption is that all walls must be of relatively equal surface area. A much more accurate and appropriate calculation for C-Factor would be:
Bonded Surface Area
––––––––––––––––––––––––––– = Configuration Factor = C-Factor
Nonbonded Surface Area
One can readily understand the importance of using this second formula (which exchanges rational numbers for pure integers) when examining a flowable resin-based liner for a Class I cavity. By taking the cavity walls as the basis for the calculated C-Factor, it would have to be:
Bonded Walls (Buccal + Lingual + Mesial + Distal + Pulpal)
–––––––––––––––––––––––––––––––––––––––––––––––– = 5 = C-Factor
Nonbonded Walls (Occlusal)
A C-Factor of 5 is quite high and would normally lead to very high stresses on the tooth. However, for a thin cavity liner applied to the pulpal floor, the buccal, lingual, mesial, and distal surfaces contribute relatively little to the total bonded surface area in comparison to the pulpal surface. Dropping the four negligible surfaces yields a C-Factor of 1, which is very low:
Bonded Walls (Pulpal)
–––––––––––––––––––––––––––––––––––––––––––––––––– = 1 = C-Factor
Nonbonded Walls (Occlusal)
This explains why using a higher shrinking flowable composite resin liner can actually help buffer against shrinkage stress and reduce postoperative sensitivity.
It is important for a clinician to consider the C-Factor of a dental cavity because those with higher C-Factors tend to have more stress-related, postoperative sequelae. This can explain why a small Class I direct composite restoration that is nowhere near the pulp can trigger significant post-restorative pain. Based on the formula above, a normal depth Class I cavity has a C-Factor of 5, which is the highest possible.
Incremental Layering Vs. Bulk Placement
To help reduce the effects of shrinkage stresses caused by cavity configuration, incremental layering instead of bulk placement of the direct restoration has been broadly advocated and accepted by clinical dentistry.19 Layering has also been recommended to improve bond strength20 and reduce interfacial microleakage,21 cuspal deflection,22 and even postoperative sensitivity.23 Although the use of some type of incremental placement with light-cured composites may be necessary for adequate light penetration and to achieve maximum depth of cure, its disadvantages include the possibility of trapping voids or contamination between layers and increased chair time.24 Different incremental placement techniques have been proposed with the rationale that oblique increments applied first to the cuspal inclines would help reduce the C-Factor and the stress applied to buccal and lingual cusps by horizontal increments that bridge them together during curing. To date, the literature has not shown conclusively that incremental layering definitively helps reduce the effects of shrinkage stress versus bulk placement. For example, a study by Abbas showed that using multiple increments caused greater cuspal deflection in premolars than a single bulk increment,25 while a more recent but similar study by Lee showed just the opposite.26 In two other studies that used finite element analysis (FEA) to study different incremental filling techniques, the results were also dichotomous. Versluis concluded that incremental filling increased the deformation of the restored tooth and led to a more highly stressed tooth–composite structure,27 while an FEA study by Kuijs concluded that using a chemically cured composite did result in lowered stress, but when considering light-cured composites, none of the layering techniques was significantly different from each other or bulk filling.28
The trend of contradictory studies is also found for the issue of oblique versus horizontal layering techniques. One study of the microtensile bond strengths to the dentin in deep Class I cavities found multiple horizontal layers to be the most promising way to get a good bond to the cavity floor.29 A later study by Nui showed that oblique layering produced higher bond strengths.30 Park et al also considered bulk filling versus horizontal and oblique layering. Their study utilized aluminum molds instead of natural teeth to exclude significant specimen variance. It found that bulk-filling techniques with light-cured composite yielded significantly more cuspal deflection than the incremental filling techniques, but found no significant differences between the horizontal and oblique incremental methods.31 Thus, it is rather difficult to draw definitive conclusions as to whether incremental layering is actually beneficial or which clinical layering technique is superior. This ambiguity has prompted manufacturers to develop and offer direct composites that are intended mainly for bulk-filling or modified bulk-filling placement techniques. (Early commercially available products for this approach include SureFil SDR® flow, DENTSPLY Caulk, and Venus® Bulk Fill, Heraeus Kulzer). The actual technique being recommended is a modified bulk-fill procedure where a horizontal layer of up to 4 mm of low-modulus flowable composite is used to fill the bulk of cavity but is capped by a 2 mm layer of more traditional, universal composite. The term “bulk-fill base” has been used to describe this procedure. Of course, should the cavity become very deep, more than one increment of the low-modulus base may still be required to assure adequate depth of cure.
Degree of Conversion and Reaction Kinetics
It would seem intuitive and it has been confirmed in the literature that a direct relationship exists between the degree of conversion and the volumetric shrinkage of a methacrylate-based composite.32,33 For a specific composite, lowering the degree of conversion will also lead to a lower shrinkage strain and interfacial stress.34 Unfortunately, lowering the degree of conversion generally has a negative impact on the physical properties of the set material; therefore, this is not a practical way to reduce stress. However, it is practical and possible to reduce polymerization stresses by altering the rate/kinetics of the polymerization reaction. The rate of cure is actually the degree of conversion per unit time (DC/s). It has been shown that slowing down the rate at which the polymer network is formed allows more of the unset material to flow and compensates for the volumetric change and even allows for a molecular level rearrangement to occur in the developing polymer. This reduces or delays the buildup of internal and interfacial stresses.35
One of the earliest methods recognized to reduce polymerization kinetics was the use of self-curing composite materials rather than photoinitiated versions. Because the polymerization reaction occurs much more slowly with self-curing composites, it provides an extended “pre-gelation stage,” which translates into higher flow and lower stress levels.36,37 However, auto-curing composites often have a lower degree of conversion and lowered physical properties when compared with light-cured composites. Thus, there is some controversy as to whether the stress reductions are actually due to an altered rate of cure or the lowered degree of conversion. Auto-cure composites also require higher amounts of tertiary amine co-initiators than light-cured composites to catalyze the setting reaction. This combined with the lesser degree of conversion leads to more unreacted monomer and greater color instability. This has discouraged a more general use of auto-cure composites.
The polymerization kinetics for light-cured composites can be favorably reduced without impacting final conversion by varying the concentration of photoinitiators or a common polymerization inhibitor, butylated hydroxytoluene (BHT), which is used to help prevent premature setting and extend the shelf-life of the product.38 Since the curing rate of light-cured composites is proportional to the square root of the power density (PD = mW/cm2), modulation of the power density delivered in the early stages of the photo-activation period or by the use of a low power density for extended exposure times has also been advocated to decrease stress without affecting the final degree of conversion. This early work by Bouschlicher and Reuggeberg39 led to a number of advanced curing lights that offer “soft start,” “ramped,” stepped, and low power modes designed to reduce the power density at the beginning of the polymerization reaction and increase it over time. While these modified curing modes have received widespread acceptance from manufacturers and practitioners, there are conflicting studies as to their overall benefits. Some studies have reported they were effective in reducing the contraction stress rate or improving the strength of the bonded interface,40 while others determined the predominant reason for decreased shrinkage stress with “soft start” or “pulse curing” was due to a modest decrease in the final conversion percentage.41 Fleming reported that soft-start polymerization did not significantly reduce marginal leakage or cuspal deflection nor increase the degree of conversion.42 Chan showed no differences in postoperative sensitivity or decreased signs of marginal stress after a 24-month clinical trial.43 A recent paper may have proposed a plausible explanation for these discrepancies. According to Ilie, soft-start polymerization may produce a valid benefit when the cavities are 2-mm deep or less, but when cavities reached depths of 6 mm or higher there was a significant drop in degree of conversion.44
Emergence of Lower Shrinkage Stress Monomer Chemistry
As discussed earlier, the development of low-volumetric shrinkage monomers such as Silorane or DX-511 has not necessarily led to a comparable reduction in shrinkage stresses. This has, in turn, stimulated developments in “lower contraction stress” monomers. One such monomer is found in the aforementioned SureFil SDR flow, which uses an oligomeric resin monomer made of a dimethacrylate, a polyisocyanate, and a reactive monomer with photoresponsive moiety derived from a photoinitiator. The resultant monomer has a higher molecular weight of 849 g/mol when compared with bis-GMA (513 g/mol). This offers the previously discussed advantage of reduced polymerization shrinkage due to fewer covalent bonds per unit of volume. However, according to the manufacturer, the high molecular weight and the conformational flexibility around the centered polymerization modulator imparts an optimized flexibility and network structure to the cured resin, which allows it to dissipate more energy (and store less) during polymerization.
Another novel low-shrinkage/stress monomer is TCD-DI-HEA (bis-(acryloyloxymethyl)tricyclo[5.2.1.02,6]decane) (which is found, for example, in Venus Diamond® Nanohybrid Composite [Heraeus Kulzer]). The TCD monomer utilizes several strategies to help reduce volumetric shrinkage and shrinkage stress. First, it possesses a very rigid backbone similar to bis-GMA, which helps reduce molecular vibrations due to Brownian motion. It also lacks the polar hydroxyl groups found in bis-GMA. Both of these properties help reduce the intermolecular distances between monomer molecules in the uncured state. Therefore, the change between the uncured and cured states is minimized, which would help impart lower volumetric shrinkage behavior to the TCD. However, the monomer also possesses highly elastic urethane side chains, which allows the molecule to internally absorb stress and better compensate for the already reduced volumetric shrinkage. Numerous studies have demonstrated that TCD is highly effective in reducing both volumetric shrinkage and the resultant shrinkage stress.45,46
Viscoelastic Effects
As previously discussed, increasing the total amount of inorganic filler has been used in restorative composites to help increase fracture toughness and resistance to wear and to reduce their overall polymerization shrinkage. It has also been shown that there is a strong correlation between filler volume and the elastic modulus or stiffness of the restorative material.47 Unfortunately, the increased stiffness of the more heavily filled materials has been found to play a major role in determining the amount of polymerization stress that is ultimately produced in the system.48 On the basis of that study it appears that using lower modulus or less heavily filled composites where clinically appropriate might be preferable, because they tend to produce lower levels of polymerization stress. While it may not be ideal to use a low-filled composite under posterior occlusal loading, it can be especially useful when restoring nonstress-bearing surfaces such as Class III or Class V lesions.49 One useful formulation modification for higher filled hybrids is the inclusion of nonbonded microfiller particles, which are thought to produce significant decreases in polymerization stress by acting as localized stress-relieving sites within the composite.50
Conclusions
Though much has already been accomplished to better understand and manage the shrinkage behavior and resultant stresses inherent in direct placed composite restorations, this continues to be a challenge. Fully comprehending all of the factors involved and their complex interactions has, to date, proven to be very difficult. For some concepts there are conflicting studies. Further research is needed to provide clinical guidance in materials and techniques for various direct restorative configurations.
Resin manufacturers have already done much to significantly lower volumetric shrinkage and are now beginning to make progress in reducing the resultant stresses to the tooth that can cause many adverse clinical sequelae. Nontraditional monomers and innovative clinical techniques offer the promise of minimizing shrinkage and stresses to far less significant levels.
DISCLOSURE
The author declares no financial affiliation with any of the companies mentioned in this article.
ACKNOWLEDGMENTS
The author wishes to acknowledge the assistance of Zach Turner of Blue Motion Studios, LLC for the creation of the drawings for this article.
ABOUT THE AUTHOR
Mark L. Pitel, DMD
Associate Clinical Professor of Operative Dentistry, Director of Predoctoral and CDE Esthetic Studies, Columbia University College of Dental Medicine, New York, New York
REFERENCES
1. Peutzfeldt A. Resin composites in dentistry: the monomer systems. Eur J Oral Sci. 1997;105(2):97-116.
2. Paffenbarger GC, Rupp NW. Composite restorative materials in dental practice: a review. Int Dent J. 1974;24(1):1-17.
3. Buonocore MG. A simple method of increasing the adhesion of acrylic filling materials to enamel surfaces. J Dent Res. 1955;34(6):849-853.
4. Bowen RL. Use of epoxy resins in restorative materials. J Dent Res. 1956;35(3):360-369.
5. Patel MP, Braden M, Davy KW. Polymerization shrinkage of methacrylate esters. Biomaterials. 1987;8(1):53-56.
6. Bausch JR, de Lange K, Davidson CL, et al. Clinical significance of polymerization shrinkage of composite resins. J Prosthet Dent. 1982;48(1):59-67.
7. Norris C, Burgess JO. Polymerization shrinkage of seventeen composite resins [abstract]. J Dent Res. 2002;81(spec iss A). Abstract 3435.
8. Condon JR, Ferracane JL. Reduced polymerization stress through non-bonded nanofiller particles. Biomaterials. 2002;23(18):3807-3815.
9. Condon JR, Ferracane JL. Reduction of composite contraction stress through non-bonded microfiller particles. Dent Mater. 1998;14(4):256-260.
10. Albers HF. Tooth-Colored Restoratives: Principles and Techniques. 9th ed. Hamilton, Ontario, Canada: BC Decker Inc.; 2002:114.
11. Bailey WJ. Cationic polymerization with expansion in volume. Journal of Macromolecular Science, Part A: Pure and Applied Chemistry. 1975;9(5):849-865.
12. Thompson VP, Williams EF, Bailey WJ. Dental resins with reduced shrinkage during hardening. J Dent Res. 1979;58(5):1522-1532.
13. Stansbury JW, Bailey WJ. Evaluation of spiro orthocarbonate monomers capable of polymerization with expansion as ingredients in dental composite materials. ACS Symposium on Progress in Biomedical Polymers: 1988, Los Angeles, CA. In: Gebelein CG, Dunn RL, eds. Progress in Biomedical Polymers. New York, NY: Plenum Press; 1990:133-139.
14. Eick JD, Byerley TJ, Chappell RP, et al. Properties of expanding SOC/epoxy copolymers for dental use in dental composites. Dent Mater. 1993;9(2):123-127.
15. Watts DC, Cash AJ. Determination of polymerization shrinkage kinetics in visible-light-cured materials: methods development. Dent Mater. 1991;7(4):281-287.
16. Tantbirojn D, Versluis A, Pintado MR, et al. Tooth deformation patterns in molars after composite restoration. Dent Mater. 2004;20(6):535-542.
17. Pfeifer CS, Ferracane JL, Sakaguchi RL, Braga RR. Factors affecting photopolymerization stress in dental composites. J Dent Res. 2008;87(11):1043-1047.
18. Carvalho RM, Pereira JC, Yoshiyama M, Pashley DH. A review of polymerization contraction: the influence of stress development versus stress relief. Oper Dent. 1996;21(1):17-24.
19. Donly KJ, Jensen ME. Posterior composite polymerization shrinkage in primary teeth: an in vitro comparison of three techniques. Pediatr Dent. 1986;8(3):209-212.
20. He Z, Shimada Y, Sadr A, et al. The effects of cavity size and filling method on the bonding to Class I cavities. J Adhes Dent. 2008;10(6):447-453.
21. Tjan AHL, Bergh BH, Lidner C. Effect of various incremental techniques on the marginal adaptation of class II composite resin restorations. J Prosthet Dent. 1992;67(1):62-66.
22. Kim ME, Park SH. Comparison of premolar cuspal deflection in bulk or in incremental composite restoration methods. Oper Dent. 2011;36(3):326-334.
23. Ward DH. Treating patients with CARE (comfortable aesthetic restorations): reducing postoperative sensitivity in direct posterior composite restorations. Dent Today. 2004;23(8):60, 62, 64-65.
24. Campodonico CE, Tantbirojn D, Olin PS, Versluis A. Cuspal deflection and depth of cure in resin-based composite restorations filled by using bulk, incremental and transtooth-illumination techniques. J Am Dent Assoc. 2011;142(10):1176-1182.
25. Abbas G, Fleming GJ, Harrington E, et al. Cuspal movement and microleakage in premolar teeth restored with a packable composite cured in bulk or in increments. J Dent. 2003;31(6):437-444.
26. Lee MR, Cho BH, Son HH, et al. Influence of cavity dimension and restoration methods on the cusp deflection of premolars in composite restoration. Dent Mater. 2007;23(3):288-295.
27. Versluis A, Douglas WH, Cross M, Sakaguchi RL. Does an incremental filling technique reduce polymerization shrinkage stresses? J Dent Res. 1996;75(3):871-878.
28. Kuijs RH, Fennis WM, Kreulen CM, et al. Does layering minimize shrinkage stresses in composite restorations? J Dent Res. 2003;82(12):967-971.
29. Nikolaenko SA, Lohbauer U, Roggendorf M, et al. Influence of c-factor and layering technique on microtensile bond strength to dentin. Dent Mater. 2004;20(6):579-585.
30. Niu Y, Ma X, Fan M, Zhu S. Effects of layering techniques on the micro-tensile bond strength to dentin in resin composite restorations. Dent Mater. 2009;25(1):129-134.
31. Park J, Chang J, Ferracane J, Lee IB. How should composite be layered to reduce shrinkage stress: incremental or bulk filling? Dent Mater. 2008;24(11):1501-1505.
32. Venhoven BA, de Gee AJ, Davidson CL. Polymerization contraction and conversion of light-curing BisGMA-based methacrylate resins. Biomaterials. 1993;14(11):871-875.
33. Silikas N, Eliades G, Watts DC. Light intensity effects on resin-composite degree of conversion and shrinkage strain. Dent Mater. 2000;16(4):292-296.
34. Ferracane J, Greener EH. The effect of resin formulation on the degree of conversion and mechanical properties of dental restorative resins. J Biomed Mater Res. 1986;20(1):121-131.
35. Braga RR, Ferracane JL. Contraction stress related to degree of conversion and reaction kinetics. J Dent Res. 2002;81(2):114-118.
36. Krejci I, Lutz F. Marginal adaptation of Class V restorations using different restorative techniques. J Dent. 1991;19(1):24-32.
37. Feilzer AJ, de Gee AJ, Davidson CL. Setting stresses in composites for two different curing modes. Dent Mater. 1993;9(1):2-5.
38. Payne MD, Ferracane JL, Sakaguchi RL. Monitoring curing of composites with varied BHT levels using DMA and PhotoDSC [abstract]. J Dent Res. 2001;80(spec iss). Abstract 250.
39. Bouschlicher MR, Rueggeberg FA. Effect of ramped light intensity on polymerization force and conversion in a photoactivated composite. J Esthet Dent. 2000;12(6):328-339.
40. Cunha LG, Alonso RC, Pfeifer CS, et al. Modulated photoactivation methods: Influence on contraction stress, degree of conversion and push-out bond strength of composite restoratives. J Dent. 2007;35(4):318-324.
41. Lu H, Stansbury JW, Bowman CN. Impact of curing protocol on conversion and shrinkage stress. J Dent Res. 2005;84(9):822-826.
42. Fleming GJ, Cara RR, Palin WM, Burke FJ. Cuspal movement and microleakage in premolar teeth restored with resin-based filling materials cured using a ‘soft-start’ polymerisation protocol. Dent Mater. 2007;23(5):637-643.
43. Chan DC, Browning WD, Frazier KB, Brackett MG. Clinical evaluation of the soft-start (pulse-delay) polymerization technique in Class I and II composite restorations. Oper Dent. 2008;33(3):265-271.
44. Ilie N, Jelen E, Hickel R. Is the soft-start polymerization concept still relevant for modern curing units? Clin Oral Investig. 2011;15(1):21-29.
45. Marchesi G, Breschi L, Antoniolli F, et al. Contraction stress of low-shrinkage composite materials assessed with different testing systems. Dent Mater. 2010;26(10):947-953.
46. Cadenaro M, Codan B, Navarra CO, et al. Contraction stress, elastic modulus, and degree of conversion of three flowable composites. Eur J Oral Sci. 2011;119(3):241-245.
47. Braem M, Van Doren VE, Lambrechts P, Vanherle G. Determination of Young’s modulus of dental composites: a phenomenological model. J Mater Sci. 1987;22:2037-2042.
48. Condon JR, Ferracane JL. Assessing the effect of composite formulation on polymerization stress. J Am Dent Assoc. 2000;131(4):497-503.
49. Tyas MJ. The Class V lesion: aetiology and restoration. Aust Dent J. 1995;40(3):167-170.
50. Condon JR, Ferracane JL. Reduction of composite contraction stress through non-bonded microfiller particles. Dent Mater. 1998;14(4):256-260.
Related Content:
For more information, read Composite Resins in 2013: An Update on Their Progress at dentalaegis.com/go/cced454