You must be signed in to read the rest of this article.
Registration on CDEWorld is free. Sign up today!
Forgot your password? Click Here!
The key to the success of soft-tissue ablative dental lasers is their ability to simultaneously cut and coagulate the tissue. Although the optical, structural, and thermodynamic properties of soft tissue (including optical absorption and scattering and photothermal ablation and coagulation) have been studied extensively,1-13 a discrepancy remains between: (a) the industry-propagated notion about efficient near-infrared (IR) 800-nm to 1,100-nm laser ablation of the oral soft tissue14-16; and (b) studies reporting inefficient near-IR absorption/ablation of the oral soft tissue.2-5,7,9,17,18
To address this discrepancy, based on the known optical absorption coefficient spectra of the oral soft tissue and the known heat transfer dependencies, the authors discuss the pulse- and wavelength-dependent differences between diode, erbium, and CO2 laser ablation and coagulation processes.
Photothermal Laser Ablation
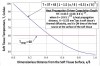
The process of photothermal vaporization of intra- and extracellular water heated by the laser light within the irradiated soft tissue is the most efficient soft-tissue laser ablation (as well as incision and excision).2-5 Water vapors quickly steam out of the strongly laser-heated soft tissue, carrying cellular ashes and other various by-products of this swift boiling and vaporization process with them. To understand how the laser light cuts the soft tissue, clinicians should examine how its absorption coefficient spectrum1-5 applies to the three wavelength groups of practical dental lasers presented in Figure 1: circa 1,000 nm (diodes and Nd:YAG laser); circa 3,000 nm (erbium lasers); and circa 10,000 nm (CO2 lasers). The near-IR diode and Nd:YAG laser wavelengths circa 1,000 nm are highly inefficient and spatially inaccurate photothermal laser ablation devices because of their weak absorption and strong scattering by the soft tissue.2-5,7 Conversely, as a result of their high absorption by the soft tissue, mid-IR erbium (circa 3,000 nm) and IR CO2 (circa 10,000 nm) laser wavelengths are very efficient and spatially accurate laser ablation tools2-5 with a low ablation fluence threshold (Figure 1).
Laser pulsing is as important for soft-tissue surgery as the laser wavelength. Highly efficient heating of the irradiated tissue occurs when the energy of a laser pulse is high and the duration of the pulse is much shorter than the thermal relaxation time (TRT),4-6 which is also presented in Figure 1. If time duration between laser pulses is much greater than the TRT, it yields the most efficient cooling of the tissue adjacent to the ablated zone. Such laser pulsing is referred to as superpulse. Because of its ability to minimize the depth of coagulation, superpulse is an essential feature of any soft-tissue surgical CO2 laser.4
Photothermal Laser Coagulation
Coagulation transpires in the 60°C to 100°C temperature range,5 which significantly reduces bleeding (and oozing of lymphatic liquids) on the ablated tissue margins during laser ablation (including incision and excision) procedures. Because blood is contained within and is transported through blood vessels, blood vessel diameter, B, (ranging from 21 µm to 40 µm)8 is a crucial spatial parameter that impacts the efficiency of the photocoagulation process. Photothermal coagulation is also joined by hemostasis because of the contraction of the walls of blood and lymphatic vessels through the shrinking of collagen at increased temperatures. Relative to the blood vessel diameter, B, the photothermal coagulation depth, H, is a key criterion of coagulation and hemostasis efficiency. The coagulation depth, H, (for the 60°C to 100°C temperature range below the ablation margins) was shown4 to be proportional to the absorption depth, A, (an inverse of the absorption coefficient presented in Figure 1), and is also presented in Figure 1 for short pulse conditions.
For ablative photothermal settings, the depth of coagulation is determined by the photothermal coagulation depth H (Figure 1) only if H is significantly shorter than the depth of ablation, which is often the case for practical cutting lasers in surgery and dentistry such as erbium and CO2 lasers (and not for diode lasers):
As illustrated in Figure 2 (a and b), just like a sharp scalpel, a laser beam with short photothermal coagulation depth (H << B, such as erbium lasers) is not capable of stopping bleeding from a severed blood vessel, because photothermal coagulation takes place on a relatively short spatial scale. Such wavelengths are excellent scalpels but poor coagulators.
A laser beam with an excessively long photothermal coagulation depth (H >> B, such as diode and Nd:YAG laser wavelengths [Figure 1]) is capable of coagulating multiple blood vessels over extended volumes of the soft tissue. Such wavelengths are excellent coagulators but poor scalpels.2-5,7
When H ≥ B (CO2 laser wavelengths [Figure 1]), coagulation reaches just deep enough into a severed blood vessel to stop the bleeding. In other words, the high coagulation efficiency of the CO2 laser is because of the close match between the photothermal coagulation depth of approximately 50 µm4 and the diameters of the oral soft-tissue blood capillaries of approximately 20 µm to 40 µm.8
For nonablative long-pulse settings, the heat propagation-driven coagulation depth, HT, can be derived from the temperature profile inside the tissue, approximated as T = 37 + 63 (1 – 1.5 (x/δ) + 0.5 (x/δ)3)9-12 and illustrated in Figure 3 (for the ablation temperature of 100°C, coagulation temperatures of 60°C to 100°C, and body temperature of 37°C, where δ = (8 K t)½ is the heat propagation distance,9-12 K ≈ 0.155 mm2/sec is the soft-tissue thermal diffusivity,4 and t is the pulse duration or the “ON” time of the heat source at the surface of the tissue) for HT >> H conditions. The heat propagation-driven coagulation depth HT = 0.45 (8 K t)½ contains the 60°C to 100°C tissue temperatures as indicated in Figure 3. For long-pulse erbium lasers (short depth of photothermal coagulation H = 3 µm to 10 µm [Figure 1]), the heat propagation-driven coagulation depth HT can exceed 20 µm (ie, HT >> H) for pulse durations of 2 msec and longer. For long-pulse CO2 lasers (depth of photothermal coagulation H = 50 µm [Figure 1]), the heat propagation-driven coagulation depth distance HT can exceed 200 µm (ie, HT >> H) for pulse durations of 200 msec and longer.
Dental Diode Hot Glass Tip
Dental diode near-IR laser wavelengths are not suitable for oral soft-tissue cutting.2-5,7 Instead, the tissue is cut thermomechanically on contact with a charred glass “hot tip.” First, an optically dark carbonized material,17,18 or “char” (eg, organic matter, burnt ink, or burnt corkwood), is deposited on the very end of the glass tip. The optical energy of the diode laser heats the charred tip of the glass fiber up to 900°C to 1,500°C.17,18 As a result, the soft tissues are heated up through the heat conduction/diffusion from the hot glass tip to and through the soft tissue, as illustrated in Figure 2. The cutting speed of such a charred hot glass tip is limited by its disintegration19 at elevated temperatures (up to 1,500°C), thus raising concerns about biocompatibility20,21 of the burnt tip’s cladding chemicals and thermally fractured glass (not sapphire tips,2 which are more rugged).
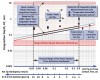
The ideal 100%-optically black hot tip acts as a nonlaser, wavelength-independent ablation thermal device (similar to electrocautery) with an approximate temperature profile in the soft tissue shown in Figure 3.9 Figure 4 presents calculated9,13 constant tip temperature (red line) and constant tip power (blue line) coagulation depths, which are compared to measurements17 for constant temperature (red circles) and are under constant power (blue circles) conditions. Figure 4 illustrates that the hot glass tip noticeably reduces the coagulation depth to less than 1 mm versus the multi-millimeter near-IR photothermal coagulation depth shown in Figure 1. Also seen in Figure 4, the hot-tip coagulation depth is affected by the tip–tissue contact time (or by the surgeon’s hand speed, ie, by the surgeon’s skill and training), but still significantly exceeds the gingival blood vessel diameters.
The coagulation process, as well as the cutting capabilities of the hot tip, strongly depends on the properties of the char on the diode’s glass tip. The insufficient charring reduces the tip temperature (which prompts sterility compliance concerns22) and increases the risk of the near-IR-induced subsurface thermal necrosis7; it also heightens the risk of bleeding due to tissue trauma by sharp edges of the glass tip.
Summary
Erbium laser wavelengths circa 3,000 nm are extremely energy efficient and spatially accurate for photothermal ablation; their photothermal coagulation depths are much shorter than gingival blood vessel diameters. CO2 laser wavelengths circa 10,000 nm are highly effective and spatially accurate photothermal ablation tools with exceptional coagulation ability as a result of the close match between photothermal coagulation depth and the diameters of oral soft-tissue blood capillaries. In nonablative applications, coagulation depth can be increased for long pulses with extended heat propagation-driven coagulation depth in excess of the photothermal coagulation depth.
Unlike CO2 and erbium lasers, the soft-tissue ablative dental diodes are contact thermomechanical cutting devices. Their coagulation depth depends on the degree of the diode’s glass tip charring and can range from sub-millimeter (heat propagation-driven coagulation for significantly charred tips) to multi-millimeter (photothermal radiant coagulation for poorly charred tips).
Disclosures
Dr. Peter Vitruk is the owner of LuxarCare, Aesculight, and Light Scalpel, LLC. Dr. Levine has no financial relationships to disclose.
Acknowledgments
The authors greatly appreciate help from Anna (Anya) Glazkova, PhD, in preparing this material for publication.
References
1. Jacques SL. Optical properties of biological tissues: a review. Phys Med Biol. 2013;58(11):R37-R61.
2. Fisher JC. Basic laser physics and interaction of laser light with soft tissue. In: Shapshay SM, ed. Endoscopic Laser Surgery Handbook. New York, NY: Marcel Dekker; 1987:96-125.
3. Fisher JC. Qualitative and quantitative tissue effects of light from important surgical lasers. In: Wright VC, Fisher JC, eds. Laser Surgery in Gynecology: A Clinical Guide. Philadelphia, PA: W.B. Saunders; 1993:58-81.
4. Vitruk P. Oral soft tissue laser ablative and coagulative efficiencies spectra. Implant Practice US. 2014;7(6): 19-27.
5. Vogel A, Venugopalan V. Mechanisms of pulsed laser ablation of biological tissues. Chem Rev. 2003;103 (2):577-644.
6. Svaasand LO. Lasers for biomedical applications. In: Driggers RG, ed. Encyclopedia of Optical Engineering. Vol 2. New York, NY: Marcel Dekker; 2003;1035-1041.
7. Willems PWA, Vandertop WP, Verdaasdonk RM, et al. Contact laser-assisted neuroendoscopy can be performed safely by using pretreated ‘black’ fibre tips: experimental data. Lasers Surg Med. 2001;28(4):324-329.
8. Yoshida S, Noguchi K, Imura K, et al. A morphological study of the blood vessels associated with periodontal probing depth in human gingival tissue. Okajimas Folia Anat Jpn. 2011;88(3):103-109.
9. Vitruk P, Convissar R, Romanos G. Near-IR laser noncontact and contact tip-tissue thermal interaction differences. Paper presented at: Academy of Laser Dentistry 21st Annual Conference and Exhibition; February 27, 2014; Scottsdale, AZ.
10. Rathore MM, Kapuno RRA. Engineering Heat Transfer. 2nd ed. Sudbury, MA: Jones & Bartlett Learning; 2011:406.
11. Ozisik MN. Heat Conduction. New York, NY: Wiley; 1980:352.
12. Faghri A, Zhang Y, Howell J. Advanced Heat and Mass Transfer. Columbia, MO: Global Digital Press; 2010:260.
13. Braga WF, Mantelli MBH, Azevedo JLF. Analytical solution for one-dimensional semi-infinite heat transfer problem with convection boundary condition. AIAA. 2005:4686:1-10.
14. Coluzzi DJ. Fundamentals of lasers in dentistry: basic science, tissue interaction, and instrumentation. J Laser Dent. 2008;16(spec iss):4-10.
15. Graeber JJ. Diode lasers: a primer. PennWell. January 2014. http://www.ineedce.com/courses/2564/PDF/1401ceiGraeber_rev3.pdf. Accessed May 13, 2016.
16. King J. Profitability built into one small tool–980nm diode laser. The Profitable Dentist. Winter 2015(253):40.
17. Romanos GE. Diode laser soft-tissue surgery. Compen Contin Educ Dent. 2013;34(10):752-757.
18. Romanos GE, Belikov AV, Skrypnik AV, et al. Uncovering dental implants using a new thermo-optically powered (TOP) technology with tissue air-cooling. Lasers Surg Med. 2015:47(5):411-420.
19. Vitruk P. Soft tissue cutting with CO2 diode lasers. Veterinary Practice News. November 2012:24.
20. Medical devices with sharps injury prevention features. Guidance for industry and FDA staff. Rockville, MD: US Dept of Health and Human Services, Food and Drug Administration, Center for Devices and Radiological Health, General Hospital Devices Branch; August 9, 2005:1-17.
21. ISO. Biological evaluation of medical devices–Part 1: Evaluation and testing within a risk management process. ISO 10993-1:2009. 4th ed. October 13, 2009.
22. Updated 510(k) sterility review guidance K90-1; Final guidance for industry and FDA. US Dept of Health and Human Services, Food and Drug Administration, Center for Devices and Radiological Health, Office of Device Evaluation; August 30, 2002:1-6.
About the Authors
Peter Vitruk, PhD, MInstP, CPhys, DABLS, MALD
Founder
LightScalpel LLC
Woodinville, Washington
Director
American Board of Laser Surgery
Robert Levine, DDS
Director of Laser Dentistry
Arizona School of Dentistry & Oral Health
Mesa, Arizona
Founder
Global Laser Oral Health LLC
Scottsdale, Arizona