You must be signed in to read the rest of this article.
Registration on CDEWorld is free. Sign up today!
Forgot your password? Click Here!
Choosing the right luting material is of vital importance to the longevity of dental restorative materials.1 There are two primary methods of cementation: conventional cementation and adhesive cementation. Conventional cementation means just filling a gap, whereby the majority of the retention comes from the preparation itself. Adhesive cementation means using adhesives and primers to create a bond. Using a less than ideal cementation protocol can negatively impact the result and longevity of the procedure.
Understanding Cements and Adhesives
The three most commonly used types of cement are conventional cement, self-adhesive cement, and adhesively bonded cement. The most commonly used conventional cements are resin-modified glass-ionomers (RMGIs). RMGIs have advantages of both composite resins and glass-ionomers. These materials have an acid-base reaction due to their glass-ionomer nature and can form a limited chemical bond with the substrate.2 They are dependent on mechanical retention, so sufficient preparation height and properly tapered preparation walls are critical. They are optimal when there is a large amount of retention and materials being used are strong enough.
The next step up, in terms of bond strength, is self-adhesive cement. With self-adhesive resin cements, the self-etching chemistry is built into the cement itself, so no separate etching or priming step is required. Although these cements provide chemical bonding and improved bond strength compared with conventional cements, their properties are inferior to adhesive cements.3
There are two categories of adhesive systems: self-etching resin cements and etch-and-rinse (the latter was formerly known as total etch). Self-etch adhesives contain acidic monomers, which etch and prime the tooth simultaneously.4 Etch-and-rinse systems contain phosphoric acid to treat the enamel and dentin before rinsing and subsequent application of an adhesive. Both etch-and-rinse and self-etch systems form a hybrid layer as a result of resins permeating the porous enamel and dentin.5 Generally, phosphoric acid creates a more pronounced and retentive etching pattern in enamel. Therefore, etch-and-rinse bonding systems are often preferred for preparations with little to no retention or when large areas of enamel are still present.4 Etch-and-rinse systems, however, can cause more postoperative sensitivity and make restorations harder to remove when they need to be replaced.
Adhesive cements may be further categorized as light-cure, self-cure, and dual-cure.6 Light-cured resin cements are indicated for thin, highly translucent ceramic restorations because they allow the transmission of light to reach through to the resin cement.7 These cements are comparatively more color stable than self- and dual-cure resin cements. Self-cure resin does not require light for polymerization and is indicated with opaque restorations because of the difficulty encountered when attempting to light-cure through an opaque restoration.7 Dual-cure resin cements can be light-cured or self-cured, but light-cure is generally recommended to achieve the best bond. Dual-cure resin cements are indicated when transmission of light through a restoration is doubtful.8
It is important to follow the manufacturer's instructions during adhesive cementation, including use of the manufacturer's adhesive and resin cement combination, because studies have found incompatibilities between some dual-cure resin cements and simplified adhesive systems.9
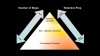
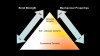
In summary, the conventional cements require the least amount of steps, but retentive preparation is extremely important. Additionally, compared with both adhesive and self-adhesive cements, conventional cements have a lower bond strength, fracture toughness, technique sensitivity, and moisture contamination (Figure 1 through Figure 3). Thus, not all restorations require the same protocol. The following sections will cover three important questions used to determine which type of cement, or adhesive, is best for each scenario.
Cementation Selection
• The three important questions to consider when determining the type of cement to use are:
• What type of restoration will be placed?
• What restorative material was used to create the restoration?
• How retentive is the preparation?
1. What type of restoration will be placed?
Indirect restorations are chosen by dentists based on the functional and esthetic requirements of the tooth being restored. Inlays and onlays are considered to be more conservative restorations because they minimize tooth structure removal when compared with a full crown. Ceramic veneers are also considered to be a more conservative restoration than a full crown for patients who desire to improve the appearance of their smile. Conservative restorations such as inlays, onlays, and veneers tend to be less retentive than full crowns and as a result are typically adhesively bonded. Veneers in particular must be adhesively bonded, due to both the non-retentive nature of the preparation and the need for an esthetic cement that will not affect the shade of the veneer. Full crowns can typically be conventionally cemented, but only if the flexural strength of the crown material is greater than 300 MPa. So a full crown fabricated with leucite-reinforced glass-ceramic (which has a flexural strength of 160 MPa) would need to be adhesively bonded even though it is a full crown.
2. What restorative material was used to create the restoration?
In addition to the type of restoration being fabricated, the restorative material selected by the clinician plays a role in selecting a cement. Historically, conventional cementation was the only choice available, and the predominant restorations of the time, cast gold and porcelain-fused-to-metal crowns, had more than enough strength to be conventionally cemented. It remains true today that any metal-based restorations can be conventionally cemented, although they can also be adhesively bonded if the preparation has inadequate retention.
With the introduction of glass-ceramic materials, the need to adhesively bond restorations became even more important due to their comparatively lower flexural strengths than metals. Most of the early all-ceramic materials were designed to be used as ceramic veneers, so adhesive resin cements needed to be esthetic and color stable over time.
With the introduction of lithium disilicate and zirconia oxide, dentists now had a tooth-colored restorative material that could be conventionally cemented if desired. However, if the preparation lacked retention or the material was thin enough that the cement would show through, an esthetic resin cement needed to be used for these otherwise high-strength materials.
3. How retentive is the preparation?
In addition to the type of restoration being prescribed and which material it is being fabricated from, the retentive features of the preparation itself must be taken into consideration. The primary considerations for the preparation are its vertical height and the degree of taper of the walls. For example, with an anterior tooth preparation that has 5 or 6 mm of preparation height, typically any method of cementation may be used. In contrast, with a lower molar, where it is common to see only 3 mm of preparation height and an overtapered proximal wall, an adhesive technique must be used. As shown in Figure 4, if there is a preparation height of 4 mm and preparation taper of 12 degrees or less, any desired cement may be used. At the same 4 mm of preparation height, if the taper is greater than 16 degrees, an adhesive cement should be used. Regardless of how strong a given restorative material may be, if the preparation lacks adequate retention, the restoration must be adhesively bonded. In this respect, question 3 is more important than the other two questions in determining which method of cementation will be used.
Treatment of the Restoration
In addition to choosing a proper cement for the restoration, the treatment of the restoration itself before cementation must be taken into account. The intaglio surfaces of feldspathic ceramics, leucite-reinforced ceramics, and lithium disilicate materials are etched by the dental laboratory with hydrofluoric acid before being sent to the dentist to remove portions of the glassy matrix and increase the bond strength between the cement and the restoration. This etching has contributed significantly to their high clinical success rates.10 Zirconia oxide cannot be etched with hydrofluoric acid because of the lack of a glassy matrix.11 As a result, the bond strength of resin cements to feldspathic ceramics, leucite-reinforced ceramics, and lithium disilicate materials is superior compared with zirconia oxide.
When the restoration is first tried in the patient's mouth, saliva comes in contact with the crown. As a result, the restoration needs to be decontaminated before placement of a silane or primer.
Historically, dentists have been taught to decontaminate glass-ceramic restorations after try-in with phosphoric acid, which works well for decontaminating lithium disilicate restorations. However, decontaminating a zirconia oxide restoration with phosphoric acid leads to predictable cement failures, especially with minimally retentive preparations. There are now multiple products on the market designed to decontaminate restorations while still allowing silanes and primers to work effectively.
For feldspathic ceramics, leucite-reinforced ceramics, and lithium disilicate materials, a ceramic silane is placed on the intaglio surface of the crown after disinfecting it, and this silane provides the bond from the resin cement to the restoration itself. Application of silane increases the wettability and chemical bond.12 For zirconia oxide restorations, a zirconia primer is placed inside the crown after disinfection. Although this increases the strength of the bond of the resin cement to the zirconia oxide material, this bond would be stronger if zirconia oxide could be etched with hydrofluoric acid, providing more micro-mechanical retention on the surface of the restorative material.
Conclusion
Clinicians must be aware and informed in order to choose the best method of cementation. As discussed, many factors are involved, but the three questions detailed in this article can be used to reach an appropriate decision.
References
1. Haddad MF, Rocha EP, Assunção WG. Cementation of prosthetic restorations: from conventional cementation to dental bonding concept. J Craniofac Surg. 2011;22(3):952-958.
2. Cardoso MV, Delmé KI, Mine A, et al. Towards a better understanding of the adhesion mechanism of resin-modified glass-ionomers by bonding to differently prepared dentin. J Dent.2010;38(11):921-929.
3.Shillingburg HT, Hobo S, Whitsett LD, et al. Fundamentals of Fixed Prosthodontics. 3rd ed. Chicago, IL: Quintessence; 1997.
4. Ozer F, Blatz MB. Self-etch and etch-and-rinse adhesive systems in clinical dentistry. Compend Contin Educ Dent. 2013;34(1):12-18.
5. Cekic I, Ergun G, Lassila LV, Vallittu PK. Ceramic-dentin bonding: effect of adhesive systems and light-curing units. J Adhes Dent. 2007;9(1):17-23.
6. Ladha K, Verma M. Conventional and contemporary luting cements: an overview. J Indian Prosthodont Soc. 2010;10(2):79-88.
7. Vargas MA, Bergeron C, Diaz-Arnold A. Cementing all-ceramic restorations: recommendations for success. J Am Dent Assoc. 2011;142(2 suppl):20S-24S.
8. Pegoraro TA, da Silva NR, Carvalho RM. Cements for use in esthetic dentistry. Dent Clin North Am. 2007;51(2):453-471.
9. Kanehira M, Finger WJ, Hoffmann M, Komatsu M. Compatibility between an all-in-one self-etching adhesive and a dual-cured resin luting cement. J Adhes Dent. 2006;8(4):229-232.
10. Della-Bona A. Important aspects of bonding resin to dental ceramics. J Adhes Sci Tech. 2009;23(7-8):1163-1176.
11. Ho CCK. Clinical techniques: assessment and minimal intervention. In: Wilson NHF, Millar BJ. Essentials of Esthetic Dentistry: Principles and Practice of Esthetic Dentistry. Elsevier; 2015:65-191.
12. Matinlinna JP, Lung CYK, Tsoi JKH. Silane adhesion mechanism in dental applications and surface treatments: a review. Dent Mater. 2018;34(1):13-28.