You must be signed in to read the rest of this article.
Registration on CDEWorld is free. Sign up today!
Forgot your password? Click Here!
Dental anxiety, or feeling stressed or uneasy at the thought of dental treatment, is a multi-faceted disorder that involves patients' somatic, cognitive, and emotional behavior responses.1-3 Multiple factors may contribute to a patient's susceptibility to developing dental anxiety. Approximately one out of every three adult women become anxious before, during, or after dental treatment, in a study conducted by Armfield et al.4 Traumatic dental experiences during childhood, family or media influences, certain psychological conditions, higher generalized fear level, low income, poor oral health literacy, and an inadequate perception of one's oral health status have all been associated with dental anxiety.4-8 Dierke et al. reported that heightened anxiety during dental care can result in delayed wound healing and severe oral inflammatory diseases.7 Adults identifying with higher levels of dental anxiety are 30% less likely to visit the dentist regularly and are more likely to avoid any dental procedures until emergency care is needed.8 Hmud et al. found that avoidance of dental treatment led to increased susceptibility of caries morbidity and decayed, missing, filled surfaces (DMFS) scores, decreased number of restored teeth, and significantly more missing teeth, as compared to patients without dental anxiety.6
Typically, once seated in the dental chair, anxious patients may appear to be irritable, uncooperative, have higher blood pressure, experience heightened sensitivities, have impaired social or cognitive function, and provide negative commentary.1-6 Anxious patients can also become fearful or cry without warning, become aggressive, have a greater chance of being self-medicated, and frequently cancel, delay, or reschedule appointments.1-10 Although these characteristic traits are commonly seen in this patient population, they are not evident in every patient with anxiety issues. However, these characteristics may be used as a guide in determining whether a patient has an undiagnosed dental anxiety.
The constructs within dental anxiety can be separated into three types: mild, moderate and severe. A patient exhibiting mild dental anxiety experiences an internal sensation that something is different and requires additional attention.11 Moderate dental anxiety is characterized when a patient only focuses on what is happening to them at the moment.12 Moderately anxious patients may experience a disturbing feeling that something is not right but are still able to learn and process new information.11 Patients experiencing severe dental anxiety are characterized as having a significant reduction in their perceptual ability.11,12 Identifying the different levels of dental anxiety allows the practitioner to make the appropriate adaptations to the patient's care.4
Dental anxiety questionnaires can provide practitioners with useful information prior to beginning patient care. Corah's Dental Anxiety Scale (DAS), the Modified Dental Anxiety Scale (MDAS), the Oral Health Impact Profile (OHIP), and Kleinknecht's Dental Fear Survey (DFS) are commonly used questionnaires. The DAS is comprised of four questions with a five-scale answering system designed to measure dental fear levels.13,14 Similar to the DAS, the MDAS incorporates a fifth question on local anesthesia.15 The OHIP is composed of forty-nine measures of oral health related quality of life questions, designed to measure patient's perceptions of the outcome of their dental disorders on their overall health and well-being.13-16 The DFS uses a five-point Likert scale to survey patients regarding their anxieties with twenty-seven specific situations.17 While use of an anxiety questionnaire does not guarantee the identification of all patients suffering from a dental anxiety, they can assist clinicians to better understand their patients' needs.
Options for treating patients with dental anxieties include rapport building, voice and movement modulation, distraction, modeling, guided imagery, environmental change, and enhancing the patient's sense of control.18 Distraction techniques can be performed by simply taking the patient's attention away from the cause of the symptoms.4,18 Modeling allows the patient to observe similar treatments prior to their own treatment appointment.4,18 Guided imagery consists of directing the patient into a dream-like state of mind and utilizes all of their senses to create an overall state of relaxation.4,18 Enhancing control allows the patient to feel more "in control" of what is happening during their dental appointment. This technique often includes the "Tell-Show-Do" method of first explaining each of the steps of the procedure, showing the procedure being performed, and then completing it on the patient.4,18
Additional treatment methods for patients with moderate dental anxiety include biofeedback, acupuncture, systematic desensitization, cognitive behavioral therapy (CBT), and hypnosis. Biofeedback utilizes instruments to measure, amplify and provide feedback on the patient's physiological status.18 Systematic desensitization, or exposure therapy, consists of encouraging the patient to talk about their dental anxiety; teaching basic relaxation techniques; and gradually exposing the patient to the source of the anxiety.4,18,19 CBT is the combination of cognitive therapy and behavioral therapy and utilizes the individual's ability to change negatively configured thoughts, or conditions, and their actions, or behaviors.4,18,19 Hypnosis is a non-invasive form of treatment that can promote deep relaxation in patients with dental anxiety. Hypnotherapy has been shown to demonstrate decisive, long-lasting effects on a patient's dental anxiety status.21
Pharmacological management, conscious sedation, and general sedation have been used successfully on patients with severe dental anxiety.22 Benzodiazepines are well suited for use in dentistry due to their anxiolytic, sedative, and amnesic qualities.22 Nitrous oxide gasses produce anoxiolytic, amnesic, and analgesic effects and are frequently used for conscious sedation during dental treatment.23,24 Most treatment techniques for patients suffering from severe anxiety are considered to be temporary solutions to the deeper underlying problem of dental anxiety.23-25
Fear of dental treatment is a significant problem in the United States with up to 80% of the population reporting having dental anxiety and about 5% of the population so fearful that they avoid dental care completely.1,4-6,25 Dental anxiety is also a burden on dental professionals with nearly 70% reporting that treating a patient with dental anxiety is a difficult challenge to their daily practice6 and the source of extensive physical, mental and emotional stress.4,25
Limited opportunities exist within either dental or dental hygiene education programs for students to gain clinical experience in identifying, assessing, and utilizing effective treatment measures for patients with dental anxiety.25 Hill et al. found that 46% of the dentists surveyed indicated interest in further training and believe that psychological treatment approaches could be successful in treating patients with dental anxiety.25 With 85% of dentists recognizing their responsibilities in treating all types of dental anxiety, clinicians need experience with multiple approaches to provide care for this population.25 While there is data on the level of knowledge, attitudes, and comfort level in treating patients with dental anxiety of dentists, data is lacking in regards to dental hygienists. The purpose of this study is to identify the already-acquired knowledge, attitudes, and level of confidence of practicing dental hygienists with respect to their treatment of patients with dental anxiety.
Methods
This study was deemed exempt by the Biomedical Institutional Review Board of the University of North Carolina, Chapel Hill (IRB #16-0992). A paper survey was developed by the authors included the following domains: demographics (6 questions) included certificates and degrees earned; practice setting (7 questions) included types of patients commonly seen and percentage of patients seen with mild, moderate and severe dental anxiety; practice behaviors (17 questions) included whether patients were screened for dental anxiety, types of questionnaires used, and dental anxiety treatment methods; dental anxiety awareness (17 questions) included common signs and symptoms of dental anxiety and knowledge-based questions; opinions and attitudes (13 questions) included confidence in treating patients with dental anxiety and educational preparation.
The survey was pilot tested by six practicing dental hygienists from the University of North Carolina School of Dentistry and revisions were made to the wording and on the face validity of each domain. Time required to complete the survey was reported by the pilot testers. The survey took approximately ten minutes to complete.
Dental hygienists attending a North Carolina state-wide annual continuing education course who were over the age of 18, had an active dental hygiene license and were currently practicing dental hygiene, were invited to participate in the study. The purpose of the paper-based survey was explained verbally prior to the start of the course and participants were asked to return the surveys at the end of the program. There were no personal identifiers on the survey and respondents were given the opportunity to include open-ended responses regarding the treatment of patients with dental anxiety.
Survey responses to the Likert scale, multiple choice and free response questions were entered by the principal investigator into an excel spreadsheet. All knowledge-based questions were captured based on the percentage of participants who answered each question correctly; confidence levels were recorded in the same manner. Descriptive statistics were used to identify any frequencies and to report distributive findings. For each respondent, the number of correct identification of symptoms was calculated (range = 0 to 6) as well as the correct number of knowledge items (range = 0 to 10). Bivariate analysis using the Mantel Baenszel row mean score test was used to assess whether the total number of correct responses to the list of symptoms and the total number of correct responses to the knowledge items differed among the level of education groups or among the years of experience groups. Probability was calculated using the data analysis.
Results
Demographics
Of the 157 surveys distributed, 153 met the inclusion criteria (n=153), yielding an overall response rate of 97%. The majority of the participants (68%) had an Associate's degree in dental hygiene, 25% a Bachelor's and 6% a Master's degree. Approximately one-third (30%) of the participants had been practicing for less than ten years and about one-quarter (24%) for over 30 years. A majority of the participants indicated a desire to learn more about treatment options and wanted to have more information regarding referral options for patients with dental anxiety.
Practice Setting
The majority (84%) of participants worked in private practice. Slightly more than a third reported working in a small town and another third were employed in a mid-sized city. When asked to respond regarding specific types of patients treated in a typical week, 96% reported working with adults and 68% included geriatric patients. A little more than two-thirds worked with pediatric populations, 50% with special needs patients, 24% with terminally ill patients, and 32% with immunocompromised patients.
Practice Behaviors
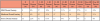
All respondents (n=153) reported treating patients with some type of dental anxiety. Over one third (34%) of respondents indicated that over 30% of their patients exhibit mild dental anxiety.
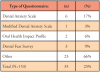
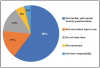
Patients exhibiting moderate or severe dental anxiety were treated less frequently by the respondents. Table I shows the various types of dental anxiety treated on a weekly basis. Fewer than one-fifth (19%) reported screening patients for dental anxiety issues. Of these, 17% utilize the DAS (Table II). Eighty-percent of participants answered "Never" or "Rarely" to using dental anxiety questionnaires and over half (60%) of the participants stated that they were unfamiliar with dental anxiety questionnaires. Data regarding the rationale for not using a dental anxiety questionnaire is shown in Figure 1.
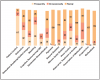
The most frequently reported service or counseling method offered by the participants was patient control (80%). The least frequently used methods of treatment were hypnosis (1%) and acupuncture (3%). One participant indicated interest in learning more about hypnosis as an option for treating an individual with dental anxiety. Figure 2 illustrates the range of services and strategies used while caring for a patient with a dental anxiety.
Dental Anxiety Awareness
Fewer than half (43%) of the participants identified all the possible signs and symptoms of dental anxiety correctly. While the average number of correct responses was not statistically significantly different among the 4 experience categories (p=0.98), all participants agreed that shortness of breath and fidgetiness/physical restlessness are symptoms of dental anxiety. Over 95% of respondents agreed, "Dental anxiety affects oral health care"; "Anxiety disorders can significantly impair daily functioning"; and "One of the leading causes of delayed dental care is dental anxiety." Fewer than one-third (31%) of participants were aware that females experience more dental anxiety than males and a little more than one-half (60%) understood the impact of dental anxiety on wound healing (Table III).
Level of dental hygiene education, Associate, Bachelor and Master's degree, was not demonstrated to be significant in regards to knowledge of dental anxiety symptoms (p=0.92). Several participants shared that, "Not enough information is available to students in their dental hygiene curriculum." However, level of education was demonstrated to be significantly different (p=0.03) among the three groups in regards to general knowledge score. Years of experience did not significantly impact knowledge scores (p=0.36).
Opinions and Attitudes
The vast majority of respondents, 98%, agreed with the statement, "Anxiety about dental treatment is a challenge for both the patient and the dental clinician." One participant added, "Anxiety in patients can cause anxiety in clinicians. Managing dental anxiety can help us treat patients better; we just need to know how to best treat these patients." Over 95% of participants agreed that dental hygienists are in a key position to screen and identify patients with dental anxiety (Table IV).
A little more than half (58%) of the participants believed that their dental hygiene education prepared them for treating patients with mild levels of anxiety; 38% felt prepared for moderate levels of anxiety; and 22% felt prepared to care for patients suffering from severe dental anxiety. Over three-quarters (78%) of the participants were specifically interested in learning more about dental anxiety questionnaires and 79% expressed interest in additional continuing education courses on treating patients with dental anxiety. A majority of the participants (82%) would like to learn more about treatment options for patients with severe dental anxiety such as where to refer them for more specialized care. The majority of the respondents (92%) indicated confidence in their abilities to perceive stress in their patients and 98% were confident in their ability to work with patients experiencing mild anxiety. Over three-quarters (77%) expressed confidence in their ability to work with patients experiencing moderate to high levels of dental anxiety.
Discussion
The majority of the respondents in this study believed that treating patients with dental anxiety is a stressful experience for both the patient and the provider, a significantly higher affirmation of the challenges of dental anxiety than previously identified by Dierke et al.7 In the Dierke et al. study, 19% of the German dentists surveyed regarding their knowledge of psychosomatic medicine indicated that treating a patient with dental anxiety was difficult. Preferred treatment options from the German study included reduced patient waiting times, shorter appointments, the use of local anesthesia, patient control techniques, and communication on fear.7 Relaxation techniques and hypnosis were used with the lowest frequency.7 The majority (95%) of the dentists surveyed in the Dierke et al. study believed that dental fear "strongly" or very "strongly" affected pain perception but only 20% believed that levels of anxiety impacted wound healing.7 Furthermore, fewer than half of the dentists in the Dierke et al. study participated in continuing education courses focusing on dental anxiety.7 In contrast, 60% of the participants in this study recognized the impact of anxiety on wound healing and 82% were interested in learning more about caring for patients with dental anxiety through continuing education courses. While there were significant differences in knowledge areas and interests in more education, some of these differences may be attributed to cultural influences between the two populations.
Educational training and experiences may play a role in a clinician's confidence and comfort levels when caring for the anxious dental patient. Hill et al. surveyed practicing dentists to determine their views and experience levels regarding the use of dental anxiety management techniques along with what was taught during dental school.25 While over half (51%) of the dentists indicated that they had received some training in treating patients with dental anxiety, 75% of the respondents indicated inadequate knowledge in the area of hypnotherapy and 65% indicated inadequacies in psychological techniques.25 A majority (85%) of the dentists in the Hill et al. study also felt a professional responsibility to treat the anxious patient.25 The majority (85%) of the dental hygienists in the current study felt well prepared by their education to treat patients with mild anxiety issues; however, they were less confident to treat moderate anxiety (57%) and severe anxiety (33%). Similar to the Hill et al study, the majority of the dental hygienists in this study expressed feelings of responsibility towards treating patients with dental anxiety.
Respondents in this study indicated a need for more educational preparation in treating patients with moderate to severe dental anxiety. The American Dental Education Association (ADEA) Compendium on Curriculum Guidelines for Allied Dental Education Programs states that dental hygiene programs should teach students to assess the pain management needs of patients and apply appropriate pain and anxiety management strategies.26 Commission on Dental Accreditation (CODA) Standard 2-12 states that graduates must be competent in assessing the treatment needs of patients presenting with special needs.27 Competency in this area requires patient experiences that include individuals whose medical, physical, psychological and social situations may require additional treatment strategies; patients struggling with dental anxiety issues come under this category. Knowledge in the areas of psychology and mental health are critical in identifying and treating a patient presenting with a dental anxiety. The majority of the dental hygienists in this study indicated the belief that dental anxiety impacts oral health and presents challenges for both the patient and clinician. Participants also indicated the need for more information on treating dental anxieties during their dental hygiene education experience. Curricular changes in dental hygiene programs specific to dental anxiety issues may assist future clinicians in playing a leadership role in the management of anxious patients.
Validated dental anxiety questionnaires provide clinicians with a useful means to identify patients with anxiety issues; however, only about 20% screened for dental anxiety and over half (60%) of the respondents were unaware of dental anxiety questionnaires. When questioned regarding the rationale for not using a questionnaire, respondents indicated a lack of knowledge in how to select a questionnaire, not having the time or not feeling it was their responsibility. In regards to time management concerns, it should be noted that the newly created Current Dental Terminology (CDT) codes address some of the issues related to providing additional levels of care for patients with dental anxiety.28 Dental care management-core coordination code, D9992, assists in the billing for additional time required to coordinate oral health care services with multiple interdisciplinary providers. A code for dental case management - motivational interviewing, D9993, was created to assist the oral health care provider in giving patient- centered, personalized counseling to identify and modify patient behaviors that can impact treatment outcomes.28 The dental case management-patient education to improve oral health literacy code, D9994, was created to establish an individualized approach to patient education with the goal of informed health care decision making.28 All three codes can be applied towards the additional time required to coordinate and plan for care of the patient with dental anxiety.
While the high response rate (97%) was a strength of this study, it is also limited by its small sample size from one state in the Southeastern United States. The validated, pilot-tested survey could be used in future studies in larger populations. The survey is useful for identifying anxiety management techniques of practicing dental hygienists as well as identifying areas that could be addressed in dental hygiene education programs and continuing education courses.
Conclusion
Dental hygienists are well positioned to play a key role to screen and care for patients with dental anxiety. Although the majority of dental hygienists in this study felt confident in their abilities to perceive stress in patients seeking dental care, they were less knowledgeable in recognizing the full range of signs and symptoms of dental anxiety. The majority of dental hygienists surveyed did not use validated questionnaires to identify the various degrees of dental anxiety and did not feel that their dental hygiene education had prepared them to treat patients experiencing severe dental anxiety. Increased curricular content and continuing education courses may be needed to provide practitioners with the necessary skills to treat patients with all levels of dental anxieties.
About the Authors
Lauren Kanzigg, RDH, MS is a graduate of the master's in dental hygiene education program; Ceib L. Phillips, PhD is a professor and associate dean for graduate/advanced education; Margot B. Stein, PhD is a clinical associate professor; Lynne C. Hunt, RDH, MEd, MS is a clinical assistant professor; all in the School of Dentistry, University of North Carolina, Chapel Hill, NC; Rebecca S. Wilder, RDH, MS is a professor and assistant dean for professional development and faculty affairs
Corresponding author: Rebecca S. Wilder, RDH, MS; Rebecca_Wilder@unc.edu
References
1. Gordan D, Heimber RG, Tellez M, Ismail AI. A critical review of approaches to the treatment of dental anxiety in adults. J Anx Dis. 2013 May; 27 (4):365-78.
2. Guzeldemir E, Toygar HU, Cilasum U. Pain perception and anxiety during scaling in periodontally healthy subjects. J Periodontol. 2008 Dec; 79 (12):2247-55.
3. Colgate Palmolive. What is dental anxiety and phobia? [Internet]. New Jersey: Colgate Palmolive; c2002-2017 [cited 2017 Sept 18]. Available from: https://www.colgate.com/en-us/oral-health/basics/dental-visits/what-is-dental-anxiety-and-phobia
4. Armfield JM, Heaton LJ. Management of fear and anxiety in the dental clinic: a review. Aus Dent J. 2013 Dec; 58 (4):390-407.
5. Gisler V, Bassetti R, Mericske-Stern R, et al. A cross-sectional analysis of the prevalence of dental anxiety and its relation to the oral health-related quality of life in patients with dental treatment needs at a university in Switzerland. Gerodontology 2010 Sep;29(1):e 290-96.
6. Hmud R, Walsh LJ. Dental anxiety: causes, complications and management approaches. J Minim Interv Dent. 2009; 2(1):67-77.
7. Diercke K, Burger GD, Bermejo JL, et al. The management of dental anxiety and impact of psychological factors on dentistry: is recent scientific research translated into German dental practices? J Health Psychol. 2013 Dec; 18(12):1519-28.
8. Sohn W, Ismail AI. Regular dental visits and dental anxiety in an adult population. J Am Dent Assoc. 2005 Jan; 136(1):58-66.
9. Rubin JG, Slovin M, Kockak M. The psychodynamics of dental anxiety and dental phobia. Dent Clin N Amer. 1988 Oct; 32(4): 647-56.
10. Gow, M. Dental anxiety, fear and phobia. Dentistry [Internet]. 2011Jun 1 [cited 2017 Sep 18]; 15(1):37-40. Available from: http://www.dentalanxiety.net/media/dentalphobia.pdf
11. Viedebeck SL. Psychiatric Mental Health Nursing. 5th ed. Philadelphia: Lippincott Williams & Wilkins; c2010. Chapter 13, Anxiety and stress-related illness; 239-66.
12. Stuart, Gail W. Principles and practice of psychiatric nursing. 10th ed. St. Louis: El Sevier; c2013. Chapter15, Anxiety responses and anxiety disorders; 217-40.
13. Corah, NL. Development of a dental anxiety scale. J Dent Res. 1969 Jul 1; 48(4):596.
14. Corah NL, Gale EN, Illig SG. Assessment of a dental anxiety scale. J Am Dent Assoc. 1978; 97(1):816-19.
15. Humphris GM, Freeman R, Campbell J, et al. Further evidence for the reliability of the modified dental anxiety scale. Int Dent J. 2000 Dec; 50(6):367-70.
16. Kleinknecht R, Klepac R, Alexander L. Origins and characteristics of fear and dentistry. J Am Dent Assoc. 1973; 86(1):842-8.
17. Slade GD, Spencer AJ. Development and evaluation of the oral health impact profile. Commun Dent Heal. 1994 Mar; 11(1):3-11.
18. Newton T, Asimakopoulou K, Daly B, et al. The management of dental anxiety: time for a sense of proportion? Brit Dent J. 2012 Sept; 213(1):271-4.
19. McMaster R, Garisto GA. Practical considerations for treating the anxious dental patient. Oral Heal [Internet]. 2012 Feb 1 [cited 2017 Sep18]; 102(2): e8. Available from: http://www.oralhealthgroup.com/features/practical-considerations-for-treating-the-anxious-dental-patient/.
20. Glaesmer H, Geupel H, Haak R. A controlled trial on the effect of hypnosis on dental anxiety in tooth removal patients. Patient Educ Couns. 2015 Sep;98(9):1112-5.
21. Allidin A. The wounded self: new approach to understanding and treating anxiety disorders. Am J Clin Hyp. 2014; 56(4):368-88.
22. Abdeshahi SK, Hashemipour MA, Mesgarzadeh V, et al. Effect of hypnosis on induction of local anaesthesia, pain perception, control of haemorrhage and anxiety during extraction of third molars: a case-control study. J Craniomaxillofac Surg. 2013 Jun; 41(4):310-5.
23. Donaldson M, Gizzarelli G, Chanpong B. Oral sedation: a primer on anxiolysis for the adult patient. Anesth Prog. 2007 Fall; 54(3):118-29.
24. Berge TI. Acceptance and side effects of nitrous oxide oxygen sedation for oral surgery procedures. Acta Odontol Scand. 199 Aug; 57(4): 201-6.
25. Hill KB, Hainsworth JM, Burke FJ, Fairbrother KJ. Evaluation of dentists' perceived need regarding treatment of the anxious person. Brit Dent J. 2008 Apr 26; 205(8):e13; discussion 442-3.
26. American Dental Education Association. Compendium of curriculum guidelines [Internet]. Washington, DC: American Dental Education Association. 2016-16 May [cited 2017 Sep18]. Available from: https://www.adea.org/cadpd/toolkit/
27. Commission on Dental Accreditation. Accreditation standards for dental hygiene education programs. Chicago: American Dental Association. 2018 [cited 2017 Mar1]. Available from: https://www.ada.org/en/coda/current-accreditation-standards
28. American Dental Association. Committee adds 11 new codes to CDT [Internet]. Chicago: American Dental Association. 2017 Jan [cited 2017 Feb]. Available from: https://www.ada.org/en/publications/ada-news/2016-archive/march/eleven-new-codes-added-to-cdt-2017