You must be signed in to read the rest of this article.
Registration on CDEWorld is free. Sign up today!
Forgot your password? Click Here!
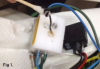
What we don’t know, or can’t see, can hurt us. Recently, the author’s dental technician called on the office for a routine service visit. A discussion started regarding water lines. The technician showed a photo of a contaminated block in a dental unit (Figure 1). Water that the office receives is filtered through these types of blocks and then enters the handpieces. Is this what should be delivered to patients?
Background
Over the last several years, water has been a focus of news reports. Approximately 63 million people nationwide have been exposed to potentially harmful water in the last decade.1 Contamination from nationwide dumping, water pipe deterioration, and pollution has affected water supplies. According to studies, many cities have violated the Environmental Protection Agency (EPA) standards for water, exposing people to contaminants such as lead, radium, and bacterial species such as the parasite cryptosporidium, which causes a diarrheal disease. Texas, Oklahoma, and California were the top states for EPA drinking water quality violations during the last de-cade. A recent environmental working group determined that Texas had the most wide-spread radium contamination in the country.2
Flint, Michigan, experienced one of the most widely publicized cases of contaminated water in recent years. In 2014 the city, in an attempt to cut costs, switched its water source from Lake Huron to the Flint River.3 The water was more corrosive from the Flint River than Lake Huron, thereby affecting the leaching of the lead from the pipes. In 2016, a federal state of emergency was issued due to lead contamination in the water from the pipes and lead solder in the pipes. As recently as August 2018, Detroit Public Schools shut off drinking water in school buildings due to lead and copper risk.4
Lead is not limited to Michigan, of course. For example, Wisconsin has many lead-lined service pipes that bring water to businesses and private homes.5 And lead is not the only substance that can appear in drinking water. Texas had water contaminated with both radium and arsenic6 in various areas, and Michigan had arsenic in private well water as recently as 2017.7 The state recommended private water testing for these wells.
Beyond prevention of lead and other environmental contaminants,8 other aspects of water used on a daily basis should be considered. The Centers for Disease Control and Prevention (CDC) recommends that dental unit water for non-surgical procedures measure less than or equal to 500 colony-forming units of heterotrophic bacteria per milliliter (≤500 CFU/mL), the standard set for drinking water by the EPA.9,10 In microbiology, CFU is a unit used to estimate the number of viable bacteria or fungal cells in a sample. Every city's water supply should have a report on the number of CFUs that are in a local area's water. Although levels are normally maintained, some areas of the country (especially rural and others with well water) have coliform bacteria at unsafe levels.
Water infected with Legionnaires' disease has become an issue in the last several years. From July 16 through August 15, 2012, a Chicago hotel reported eight people contracted the flu-like Legionnaires' disease from possible water sources, such as the pool, hot tub, and fountain areas. Eight guests were affected, and two died. The cause of this out-break was Legionnaires' disease present in a water source.11 Legionnaires' was also the cause of several deaths at a US Department of Veterans Affairs (VA) facility in Quincy, Illinois.12 Also, in November 2017, a cooling tower in Disneyland had to be shut down be-cause of one death and 11 cases of illness due to Legionnaires.13
In dentistry, the most pertinent case of infected water happened in Italy, where an 83-year-old woman died from Legionnaires after being treated at a dental office. In February 2011, the woman was admitted to the hospital with a fever and respiratory distress, which quickly denigrated to septic shock, and she died within 2 days. The Legionella strain found in the dental water lines matched what was found in the patient.14,15 This was the first confirmed case of infected dental water lines. Because of the favorable stagnant water temperature, dental water lines are conducive to Legionella growth found in the dental water lines matched what was found in the patient.14,15 This was the first confirmed case of infected dental water lines. Because of the favorable stagnant water temperature, dental water lines are conducive to Legionella growth.
In July 2017, a water outbreak in a dental clinic in Anaheim, California, caused a young girl to be hospitalized for a month due to contaminated water that was used during her pulpotomy. The girl, Mimi Morales, was the first child to be brought into the Orange County Children's Clinic with symptoms of swollen cheeks and an infection that spread to her gums and bone. Six more children were later infected with the same mycobacterial infection. The source was identified as contaminated water from the dental clinic. In the end, more than 70 children were affected. The dental clinic where this occurred was subsequently closed down.16
A bill was brought to the California state legislature that was spurred in part by the outbreak. Assembly Bill 1277, introduced by Tom Daly (D-Anaheim), called for the Dental Board of California to amend the regulations on the minimum standards for infection control for certain dental procedures that expose the dental pulp and may create an opportunity for infection. The bill, which is now part of the California Dental Practice Act,17 requires water or other methods used for irrigation to be sterile or contain recognized disinfecting or antibacterial properties when procedures that expose dental pulp are performed.
Dental Unit Water Lines
Dental unit water lines (DUWL) may be contaminated not only with biofilm but with external water. Water coming into the office is not sterile and may possibly contain waterborne bacteria and trace amounts of nutrients that may support the growth of bacteria in water lines. In a report on the diversity of bacteria in dental water lines,18,19 the presence of potentially pathogenic genera was discussed, including Pseudomonas and Legionella. Also found to be present in DUWL were emerging and opportunistic pathogenic bacteria, including Mycobacterium, Propionibacterium, and Stenotrophomonas; some of these cause fatal infections in immunocompromised patients.
Fortunately, major city sources use chlorine and other antimicrobial treatments to deliver drinking water that complies with the EPA standard of ≤500 CFU/mL.20,21 Water purification follows a basic path of decontamination, removing and filtering the dirt, and then applying chemicals (for example, chlorine, chloramine) to disinfect and kill any remaining parasites, bacteria, and viruses, as well as protecting the water from contamination during transport.22 Water from other sources, such as wells, is treated differently. The dentist should be aware of the source of the water in the office and the treatments provided.
The water in water lines23 flows quickly from the source (city or well water). Water also flows freely from sinks. DUWL are more like a pond than a river because the water sits stagnant for hours, rather than having a constant flow. When the dam is open, water is still stagnant because it is used so infrequently-less than an hour a day. Therefore, there are almost 23 ½ hours of stagnant water and potential bacterial growth lurking in the water lines.24
Biofilm in DUWL
Biofilm growing in stagnant water lines is a concern. The CDC has defined biofilm as a thin, slimy film of bacteria that sticks to moist surfaces, such as those inside DUWL. Biofilm occurs in DUWL because of the long, small-diameter tubing and low flow rates used in dentistry, the frequent periods of stagnation, and the potential for retraction of oral fluids. As a result, high numbers of common water bacteria can be found in untreated dental unit water systems. A few disease-causing microorganisms found in untreated dental unit water include Legionella, Pseudomonas aeruginosa, and nontuberculous mycobacteria. The Organization for Safety, Asepsis and Prevention (OSAP), a growing community of clinicians, educators, researchers, and industry representatives who advocate for safe and infection-free delivery of oral health-care, defines biofilm in the following manner: "Dental unit waterline contamination consists of slime-producing bacteria, fungi and protozoans. These microorganisms colonize and replicate on the interior surfaces of waterline tubing, inevitably resulting in adherent heterogeneous microbial accumulations"-not what anyone would want "living" in water lines.25
DUWL consist of approximately 6 feet of tubing that is 1 mm in diameter. Biofilm has a life cycle of its own. Biofilm bacteria adhere to the lining surface of water lines, a process that can occur continuously and is reversible. The attached bacteria will divide and excrete extra-cellular matrix within minutes of accumulation. The most harmful extracellular matrix comes from the gram-negative bacteria. As with all biofilm, the matrix forms an architecture to survive, creating further expansion and growth of the accumulated cells. Over the course of days or weeks, some of the outer bacteria are broken off and attach further down the line of the tubing. The planktonic water moves down these lines and becomes stagnant at any random point in the system, causing further reattachment, growth, and creation of new colonies of bacteria. These ever-moving bacterial colonies may create more than 200,000 CFU/ml within 5 days of installing new water lines, far above the ≤500 CFU/mL standard.23
Biofilm serves as a reservoir for more bacteria to accumulate. Imagine a shower. Think about the slime removed when shower walls are cleaned. A shower consists of a large amount of water that dries quickly, but the slime remains. Dental tubing is the perfect host.26,27 DUWL are never dry, and slime builds up. Consider the bacteria that adhere to the inside of the water-line tubing. The tubing supplies water to dental handpieces and may potentially contaminate patients.
In dentistry, biofilm forms on the walls of small-bore plastic tubing in dental units that deliver coolant water for high-speed dental handpieces, air-water syringes, and ultrasonic scalers. These instruments may harbor microbial biofilm. According to ProEdge Dental Water Labs, which performs tests on dental-unit water, approximately 70% of water-bearing instruments pass testing. Scalers and ultra-sonic units fail at a rate of approximately 43%. Air-water syringes fail at a rate of about 28%.28
Dentists are concerned about all patients, but immunocompromised patients in particular may be more affected than others by bio-film. Legionnaires' disease can result from the biofilm in DUWL. According to OSAP, "Numerous studies conducted over the last 30-plus years have identified the presence of waterborne opportunistic pathogens in dental unit water, and these findings pro-vide reason for potential concern. Many environmental organisms identified in dental treatment water have been associated with opportunistic infections in hospitalized or immunocompromised patients. For example, Pseudomonas species, non-tuberculous myco-bacteria, and Legionella species all have been isolated from dental unit water. Legionella, the causative agent of Legionnaires' disease, may pose a particular concern, as it appears to be transmitted by inhaling aerosols or aspirating water contaminated with the bacteria." Consequently, immunocompromised patients need special care and concern.14,29-32
Many bacterial species are found in DUWL (Table 1). Gram-negative bacteria found in dental water lines may produce potent endo-toxins. Untreated dental units may contain more than 2,500 endotoxin units per milliliter (EU/mL). High levels of endotoxin affect wound healing in periodontal surgery. Other side effects may occur, such as increased heart rate, fever, respiratory distress, and shock. These endotoxins have also been shown to create occupational asthma in dentists.9
Infection Control Measures
Dental water lines are an infection control issue.27,33 The American Dental Association (ADA), CDC, and OSAP have issued statements concerning the daily flushing of water lines.34-38 Water testing is now recommended by both the ADA and US Food and Drug Administration (FDA).35-38 According to the ADA statement, "The only way to ensure effectiveness of a dental unit waterline cleaning regimen is to actually test the water coming out of the unit…In-office testing kits as well as mail-in services are available for monitoring water quality. Some dental unit manufacturers provide a schedule for monitoring their equipment. Check with your manufacturer to see if they have a recommended schedule."38 Therefore, it is incumbent on all dental practices to test and treat their DUWL.39
On June 14, 2018, the FDA36 issued an up-dated statement on water lines, recommending treatment with commercial products such as chemical germicides to meet drinking water standards of ≤500 CFU/mL of heterotrophic bacteria. Sampling recommendations include the connection to the water source, the dental handpiece connection, and a midpoint between these. The FDA advises following the manufacturer's instructions for the recommended maintenance. Three agencies (OSAP, CDC, and FDA) now recommend water flushing for several minutes in the morning before seeing patients, 20 to 30 seconds between patients, and several minutes at the end of the day after patients are seen (Figure 2). Water flushing allows all the stagnant water to be pushed out of the lines prior to use. The air-water syringe, all high-speed handpieces lines, and ultrasonic/air/sonic polishing units all should be flushed to evacuate the water for the recommended several minutes at the beginning and end of the day and 20 to 30 seconds after patient care. These procedures should be incorporated into office policies.9,34-37
Water-line infection control consists of three components: testing, shocking the system to clean out the lines, and disinfection. Water testing should be a component of overall infection control strategies. It may be performed in the office or sent out to a service (Table 2).40 In-office testing offers screening for microorganism levels, although not all microorganisms may be identified. In-office testing may be considered more of a screening than a test because it may not indicate all levels of bacteria present in the lines.41 Laboratory testing offers a higher level of reliability, along with a more accurate assessment. Laboratory testing is not overly expensive when considering the level of assessment, but to achieve the best results, accurate sample evaluations will require following the service's written instructions.
There are also differences in testing due to the planktonic nature of the biofilm released at random points within the system. Biofilm matures at different rates and disburses at different times; it detaches and becomes planktonic in different sizes. It then reattaches downstream, and the cycle continues. Samples contain detached planktonic biofilm only, which explains the variance in results.42
In addition to water testing, the lines need to be disinfected and treated. Several methods are available to clean out DUWL. First, the equipment manufacturer should be consulted. The manufacturer may have suggestions or preferred methods of care for the disinfection. Some manufacturers may want the dental office to install an anti-retraction valve and an independent water reservoir, unless those are already present. These reservoirs allow the office to use the water of choice and facilitate use of water-line disinfectant treatments. To keep and maintain the closed system, a separate water reservoir is recommended.
Distilled or filtered water may be used; each manufacturer has its own preference. It de-pends partly on where the practice is located and what type of water it receives from the local municipality. As always, check with the manufacturer for suggested protocols. Regardless of what type of water is used in the office system, sterile water must always be used for surgical procedures. Finally, water heating is not recommended. Historically, water was warmed to accommodate patients' sensitivity levels. This procedure has been shown to be a breeding ground for more biofilm and is therefore discouraged.
It is recommended the lines be shocked first. A shock treatment is designed to completely dislodge an established biofilm from the length of DUWL tubing. After achieving complete removal of the biofilm, daily or weekly maintenance continues to slow or prevent new adherence.43 Shocking can be achieved by using 1:13 sodium hypochlorite solution with 8.25% household bleach. Chlorhexidine gluconate 0.12%, chlorine dioxide, 2% hydrogen, or citrus botanicals are also effective (Table 3).43,44 These four latter products remove biofilm but remain in post-treatment water. With bleach, the corrosiveness of the product must be considered; some research has questioned the use of bleach.43 It is important to follow the recommended procedure to avoid damaging the equipment. Also, the vehicle by which the disinfectant is delivered should be considered. Liquid is disbursed more easily throughout the lines; a tablet may need to dissolve. Residual particles of the tablet may be beneficial for longer-term protection but may also be a concern in the tiny orifices for the connectors and inside the handpieces. If dental water treatment products are not used, the biofilm cycle of regrowth and reattachment will occur within only 4 days after shocking the water lines. Shocking should be repeated every 60 days. ADA has an extensive list of available products that are accepted by both the FDA and EPA. As always, it is imperative to follow manufacturer's instruction before using any chemicals in the office.
For daily use, several manufacturers offer in-line water treatments; a variety of water treatments are available.45 The ideal water-line treatment should be antimicrobial, should be non-corrosive to metals, should have no (or minimal) lingering aftertaste, should cause no damage to internal lines or equipment, and should be nontoxic to the patient.33 Additionally, water treatments should be time efficient and sustainable, should not affect dental restorative materials, and should have no hormone disrupters. Several products may be needed to clean, disinfect, and then maintain the DUWL (Table 4).44
Some systems provide purified water delivered to units (eg, VistaClear™, Hu-Friedy, hufriedy.com; Sterisil System™, Sterisil, sterisil. com); others release a yearly dose of product into the line (Table 5).44 If using these purified water systems, in-line low-level antimicrobials such as tablets or straws are necessary. All units recommend initial and periodic shocking to remove biofilm from within the lines before use. Filters are available and are placed between the line and the delivery instrument. They block microorganisms but do not affect the buildup of biofilm inside the lines, so they may not remove endotoxins. They need to be replaced, and the lines may clog if they are not treated. As with any product, it is important to follow manufacturer's recommendations for long-term use. Some in-line water filters release iodine. Tablets may be used, but initial shock and constant monitoring are still required. Routine care products are available. The dental team should evaluate them after recommendations are made by the equipment manufacturer.
Other products for disinfection include ozone. Ozone has been the subject of many re-cent news reports. Although it cleans the water, there must be something to have residual microbial action in the lines. Silver impregnated into tubing has also been shown to have some microbial effect, but it will also need low-level antimicrobial maintenance with a straw or a tablet. Citrus botanicals have been used as a daily maintenance product. These products will need shocking every week if they are used alone. Iodine straws contain a good low-level antimicrobial but may need shocking more often than once a year; manufacturer instructions should be followed. Regardless of the method chosen, lines should be tested quarterly to ensure treatments are working.
Another method is to completely empty all the water in the lines (including the water bottle) and purge the lines with air. This method is recommended by several manufacturers and technicians. Although drying the lines by purging all the air and water out of them may have a marginal benefit, the lines will never be completely dry. Low-level disinfection is still necessary on a routine basis. Previous studies concluded that, because of the inability of the lines to be completely dry, drying the water lines for about 16 hours per day did not result in reduced counts of bacteria in water samples.46 If dry purging the system, using a straw system with constant delivery of the product or a tablet every 10 to 28 days, in addition to periodic shocking, is suggested.
The importance of training the dental team and having these infection control safeguards in office policies and procedures is critical, not only or the safety of patients, but the dental practice (Figure 3 and Figure 4).9 Whatever goes through the system not only goes through the water supply but the equipment; removing biofilm residue from expensive handpieces is a costly visit from a repair technician. Sludgy biofilm buildup in DUWL will not only enter the handpieces and the air-water syringe but will affect the functionality of the equipment and offset any previous infection control protocols by delivering water that has a higher CFU than deemed healthy.
Conclusion
Reflecting on water use in the office, practitioners must consider the source. Gooseneck pipes, lead solder, plumbing fixtures, and fittings are all potential sources of contaminants. For those who rent or did not build the office from the ground up, there may be issues lurking in the water lines beyond bacterial contamination. The presence of biofilm and particulate contaminants does not only affect the patient but may potentially affect the performance of dental equipment and handpieces. It is prudent for everyone to perform water testing and water-line treatments as part of routine infection control proto-cols in the office. Water-line testing and routine maintenance with low-level antimicrobial treatments are an inexpensive precaution for practices to ensure the water used is safe.
About the Author
Sheri B. Doniger, DDS
Private Practice; Lincolnwood, Illinois
Queries to the author regarding this course may be submitted to authorqueries@aegiscomm.com.
References
1. Philip A, Sims E, Houston J, Konieczny R. Millions consumed potentially unsafe water in the past 10 years. The Texas Tribune. https://www.texastribune.org/2017/08/16/millions-consumed-potentially-unsafe-water-past-10-years/. Published August 16, 2017. Accessed October 22, 2018.
2. Alfonso F III. Texas has the most radiated drinking water in the country, according to new report. Houston Chronicle. https://www.chron.com/news/houston-texas/texas/article/texas-most-contaminated-water-ewg-report-2018-12490763.php. Updated January 12, 2018. Accessed October 22, 2018.
3. Hanna-Attisha M, LaChance J, Sadler RC, Schnepp AC. Elevated blood lead levels in children associated with the Flint drinking water crisis: a spatial analysis of risk and public health response. Am J Public Health. 2016;106(2):283-290.
4. Frank A. Drinking water to be shut off at all Detroit public schools. Crain's Detroit Business. https://www.crainsdetroit.com/education/drinking-water-be-shut-all-detroit-public-schools. Published August 28, 2018. Accessed October 26, 2018.
5. Porter G Jr. Wisconsin's rate of lead poisoning worse than Flint, Michigan's. The Observatory. https://observatory.journalism.wisc.edu/2018/05/10/wisconsins-rate-of-lead-poisoning-worse-than-flint-michigans/. Published May 10, 2018. Accessed October 22, 2018.
6. Thorpe J. High levels of arsenic detected in South Texas water supply. Laredo Morning Times. https://www.mysanantonio.com/news/local/article/Webb-County-water-supplier-reports-high-levels-of-12718445.php. Updated February 28, 2018. Accessed October 22, 2018.
7. Arsenic in well water. Michigan Department of Environmental Quality. https://www.michigan.gov/documents/deq/deq-wd-gws-wcu-arsenicwellwater_270592_7.pdf. Accessed October 22, 2018.
8. Fact Sheets. US Environmental Protection Agency. https://www.epa.gov/safewater/mcl.html. Accessed October 22, 2018.
9. Kohn WG, Collins AS, Cleveland JL, et al; Centers for Disease Control and Prevention. Guidelines for infection control in dental health-care settings--2003. MMWR Recomm Rep. 2003;52(RR-17):1-61.
10. Recommended infection-control practices for dentistry, 1993. Centers for Disease Control and Prevention. MMWR Recomm Rep. 1993;42(RR-8)1-12.
11. Legionnaires' disease outbreak kills 2 at Chicago hotel. CNN. https://www.cnn.com/2012/08/28/health/chicago-hotel-legionnaires-disease/index.html. Updated August 28, 2018. Accessed October 22, 2018.
12. Zimmerman B. Troubled Illinois VA facility sees 4 Legionnaires' cases in February: 5 things to know. Becker's Hospital Review. https://www.beckershospitalreview.com/quality/troubled-illinois-va-facility-sees-4-legionnaires-cases-in-february-5-things-to-know.html Published February 21, 2018. Accessed October 22, 2018.
13. Karlamangla S. Anaheim Legionnaires' outbreak grows; 11 cases linked to Disneyland visits. Los Angeles Times. http://www.latimes.com/local/california/la-me-ln-legionella-disneyland-20171115-story.html. Published November 15, 2017. Accessed October 22, 2018.
14. Ricci ML, Fontana S, Pinci F, et al. Pneumonia associated with a dental unit waterline. Lancet. 2012;379(9816):684.
15. Atlas RM, Williams JF, Huntington MK. Legionella contamination of dental-unit waters. Appl Environ Microbiol. 61(4);1208-1213.
16. Kravarik J. Bacteria in dentist's water sends 30 kids to hospital. CNN. https://www.cnn.com/2016/10/11/health/california-dental-water-bacteria/index.html. Published October 12, 2016. Accessed October 25, 2018
17. AB-1277 Dentistry: Dental Board of California: regulations. (2017-2018) California Leglislative Information. https://leginfo.legislature.ca.gov/faces/billTextClient.xhtml?bill_id=201720180AB1277. Published October 2, 2017. Accessed October 22, 2018.
18. Costa D, Mercier A, Gravouil K, et al. Pyrosequencing analysis of bacterial diversity in dental unit waterlines. Water Res. 2015;81():223-231.
19. Understanding the Safe Drinking Water Act. US Environmental Protection Agency. www.epa.gov/sites/production/files/2015-04/documents/epa816f04030.pdf. Accessed October 22, 2018.
20. Singh R, Stine OC, Smith DL, et al. Microbial diversity of biofilms in dental unit water systems. Appl Environ Microbiol. 2003;69(6):3412-3420.
21. National primary drinking water regulations. US Environmental Protection Agency. www.epa.gov/ground-water-and-drinking-water/national-primary-drinking-water-regulations. Accessed October 22, 2018.
22. Community water treatment. Centers for Disease Control and Prevention. https://www.cdc.gov/healthywater/drinking/public/water_treatment.html. Accessed October 22, 2018.
23. Clean water doesn't equal clean water lines. Off the Cusp. https://www.offthecusp.com/clean-water-doesnt-equal-clean-waterlines. Published February 26, 2016. Accessed October 22, 2018.
24. Shearer BG. Biofilm and the dental office. J Am Dent Assoc. 1996;127(2):181-189.
25. Dental unit waterlines: dental unit water line fact sheet. OSAP. https://www.osap.org/page/Issues_DUWL_3/Dental-Unit-Waterlines-Dental-Unit-Water-Line-Fact-Sheet.htm. Accessed October 25, 2018.
26. Siebert K. Advances in water line infection control aid the hygienist's role in safety. RDH. https://www.rdhmag.com/articles/print/volume-33/issue-11/features/safe-water-delivery.html. Published November 12, 2018. Accessed October 22, 2018.
27. Dewhirst N, Molinari JA. (2018) Treating and monitoring dental water. Compend Contin Educ Dent. 2018;eBook:11-21. https://www.aegisdentalnetwork.com/cced/ebooks. Published May 25, 2018. Accessed October 22, 2018.
28. ProEdge Academy. ProEdge Dental Water Labs. https://proedgedental.com/dental-waterline-education/. Accessed October 26, 2018.
29. Depaola LG, Mangan D, Mills SE, et al. A review of the science regarding dental unit waterlines. J Am Dent Assoc. 2002;133(9):1199-1206.
30. Mills S. Are your waterlines safe? Keeping dental waterlines free from colonizing biofilms. Dimensions of Dental Hygiene. 2007;5(6):28-30.
31.Kelsch NB. Legionnaires disease waterlines. Dentistry IQ. https://www.dentistryiq.com/articles/2012/02/legionnaires-disease-waterlines.html. Published February 20, 2012. Accessed October 22, 2018.
32. Peralta G, Tobin-D'Angelo M, Parham A, et al. Notes from the field: Mycobacterium abscessus infections among patients of a pediatric dentistry practice--Georgia, 2015. MMWR Morb Mortal Wkly Rep. 2016;65(13):355-356.
33. Molinari JA. Dental water line infection control: a work in progress Dental Economics. https://www.dentaleconomics.com/articles/print/volume-107/issue-2/science-tech/dental-water-line-infection-control-a-work-in-progress.html. Published February 8, 2017. Accessed October 22, 2018.
34. Kelsch NB. Protocol for flushing water lines. RDH. https://www.rdhmag.com/articles/print/volume-38/issue-4/content/water-safety.html. Published April 1, 2018. Accessed October 22, 2018.
35. Rice EW, Rich WK, Johnson CH, Lye DJ. The role of flushing dental water lines for the removal of microbial contaminants. Public Health Rep. 2006;121(3):270-274.
36. Dental unit waterlines. US Food and Drug Administration. https://www.fda.gov/medicaldevices/productsandmedicalprocedures/dentalproducts/ucm610545.htm. Accessed October 22, 2018.
37. Dental unit waterlines: dental unit water line fact sheet. Organization for Safety, Asepsis and Prevention. https://www.osap.org/page/Issues_DUWL_3/Dental-Unit-Waterlines-Dental-Unit-Water-Line-Fact-Sheet.htm. Accessed October 22, 2018.
38. Dental unit water lines. American Dental Association. ada.org/en/member-center/oral-health-topics/dental-unit-waterlines. Updated October 12, 2018. Accessed October 22, 2018.
39. The importance of dental unit waterline maintenance - infection control. OSHA Review. https://oshareview.com/2017/02/the-importance-of-dental-unit-waterline-maintenance-infection-control/. Published February 22, 2017. Accessed October 22, 2018.
40. Stein JM. A perfect hurricane: dental waterline safety. RDH. https://www.rdhmag.com/articles/print/volume-38/issue-1/content/a-perfect-hurricane-dental-waterline-safety.html. Published January 1, 2018. Accessed October 22, 2018.
41. Morris BF, Vandewalle KS, Hensley DM, Bartolini JA Comparison of in-office dental unit waterline test kits. Mil Med. 2010;175(11):901-906.
42. Vlamakis H, Chai Y, Beauregard P, et al. Sticking together: building a biofilm the Bacillus subtilis way. Nat Rev Microbiol. 2013;11(3):157-168.
43. O'Donnell MJ, Boyle MA, Russell RJ, Coleman DC Management of dental unit waterline biofilms in the 21st century. Future Microbiol. 2011;6(10):1209-1226.
44. Synopsis of dental unit waterline treatment products and devices. USAF Dental Evaluation & Consultation Service. https://www.crosstex.com/sites/default/files/public/educational-resources/products-literature/usaf-study.pdf. Accessed October 26, 2018.
45. Cuny EJ, Eklund KJ. Management strategies for dental unit waterlines. Decisions in Dentistry. http://decisionsindentistry.com/article/management-strategies-dental-unit-waterlines/. Published April 4, 2017. Accessed October 22, 2018.
46. Fiehn NE, Larsen T. The effect of drying dental unit waterline biofilms on the bacterial load of dental unit water. Int Dent J. 2002;52(4):251-254.