You must be signed in to read the rest of this article.
Registration on CDEWorld is free. Sign up today!
Forgot your password? Click Here!
The vision of the American Dental Hygienists' Association is to support the integration of dental hygienists into the health care delivery system and improve the public's oral and overall health.1 Evidence-based practice (EBP) plays an important role in realizing this goal and should be incorporated into the education process to prepare dental hygienists to meet the needs of the public. While the importance of the EBP concept has been emphasized for a wide range of health professions including medicine, nursing, and dentistry,2-8 implementation and outcomes assessment in the dental hygiene curricula remains challenging.
Evidence-based dental practice as defined by the American Dental Association is an approach to oral healthcare requiring the systematic integration of relevant scientific evidence as it relates to the patient's oral and medical condition combined with the dentist's clinical expertise and the patient's treatment needs and preferences.9 The primary goal is optimal patient care, and an increasing emphasis has been placed on establishing an evidence-based approach to clinical care and treatment.10 However, it is important to identify factors that may influence a practitioners' ability to embrace EBP. Knowledge and experience of practitioner, educational environment and information overflow, among other factors may be perceived as barriers to implementing EBP,11-13 suggesting that developing positive perspectives towards EBP early in education process plays a key role in shaping attitudes towards EBP.
Dental hygiene students (DNHY) at Loma Linda University (Loma Linda, CA, USA) are taught to use an evidence-based approach to patient care throughout the two-year curriculum. Special emphasis on EBP is given during the 12-week research design and applied statistics course taught during the summer term. The research design course is notable in that both matriculating senior DNHY and third year dental students (D3) are taught the basic concepts and principles of conducting and evaluating research in dental and biomedical sciences together. The students also develop required skillsets to recognize clinical problems, search and review the literature, interpret results and draw appropriate conclusions based on the best evidence. The course is designed to enhance critical thinking skills and lay the foundation for the dental professionals' commitment to life-long learning in addition to meeting Commission on Dental Accreditation (CODA) standards.14
With the incorporation of EBP into the dental and dental hygiene curricula, a need was established for the development of an assessment tool to measure the outcomes effectiveness of EBP training. Hendricson et al., developed and validated a Knowledge, Attitude, Access and Confidence Evaluation (KACE) instrument to measure EBP education outcomes specifically for dentistry.15 Previous assessment tools have been designed for medicine. The KACE survey consists of 35 items measuring four EBP domains: knowledge of EBP concepts (10 items); attitudes about EBP (10 items); accessing evidence (9 items); confidence in critical appraisal (6 items).9 Overall, the KACE survey demonstrates sensitivity in regards to the type of training or experience, individual responsiveness, test-retest reliability, and internal consistency.15
There are a number of studies evaluating the four dimensions of EBP on dental students, dental faculty, and dental hygiene faculty.6,7,15,16 However there is a gap in the research in regards to dental hygiene students and EBP education outcomes. The purpose of this study was to evaluate the changes in EBP knowledge, attitudes, evidence-accessing methods and confidence in a mixed class of dental hygiene and dental students as measured over a short period (12 week course) of time.
Methods
The Loma Linda University Institutional Review Board (IRB #5160409) granted this study exempt status. All second-year DNHY (n=19) and D3 (n=96) enrolled in the Loma Linda University, School of Dentistry research design and applied statistics course during the 2016-17 academic year participated in the study. The Knowledge, Attitude, Access and Confidence Evaluation (KACE) survey instrument developed by Hendricson et al.15 was printed as a hard copy and distributed during the first class session. The survey consisted of 35 multiple choice questions addressing respondents' knowledge in determining levels of evidence, literature search strategies, analysis of study design and results, and the identification of PICO (problem, information, comparison, outcome) questions. All DNHY and D3 students completed the KACE survey on the first day of class; a second KACE survey was distributed as a post-test at the completion of the 12 week course.
The KACE assessment instrument was transferred to a survey distribution tool (Qualtrics, Provo, UT, USA). All of the knowledge responses were recorded by the research team into an excel data spread sheet as either incorrect (0) or correct (1) for appropriate data analysis. Questions assessing EBP attitudes, access and confidence utilized a 5-point Likert scale with the attitude questions scaled strongly agree=1 to strongly disagree=5; while the access of evidence scale ranged from: 1= very frequently to 5 = never. The confidence scale ranged from: 1=very confident to 5 = not at all confident.15 While the original KACE instrument was used for this survey, the scale was in reverse order so as to align positive responses first. Data entry into excel spreadsheets was cross-checked for the correctness of entry.
Descriptive statistics were conducted to profile all variables in the study. Fisher's exact test was used to evaluate knowledge, and the non-parametric Wilcoxon Rank Sum (Mann-Whitney) procedure was used to assess whether the two student groups differed at the pre and post-survey on attitude, access and confidence. Friedman's test was used to evaluate changes within each group in the four domains. Standard residual analyses were carried out to assess the validity of assumptions including residual plots and Shapiro-Wilk tests of normality. Analysis of the statistical models above including parameter and confidence interval estimation was accomplished using a statistical software program (IBM®; SPSS®v24). The level of significance was set at α=0.05 for all tests.
Results
All DNHY students (n=19) completed the pre- and post-KACE surveys; of the D3 students (n=96) enrolled in the research design course, 82% (n=79) completed both surveys. The survey responses are reported in the respective domains.
Knowledge Domain
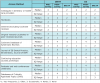
The mean percentage of correct responses to the knowledge of critical appraisal questions on the pre-test was 26% for DNHY as compared to 28% for D3 students; both DNHY and D3 had 38% mean for correct knowledge responses on the post-test. Within their respective groups, both DNHY and D3 students demonstrated a statistically significant increase in knowledge (DNHY: p=0.002 and D3: p<0.001). However, the difference in the knowledge domain on the post-test between the two groups (p=1.0) was not statistically significant. Correct responses by knowledge category are summarized in Table I.
Attitude Domain
Respondents attitudes regarding EBP on the pre-survey were not statistically different (p = 0.966) between the DNHY and D3 groups; both groups indicated negative attitudes towards EBP. DNHY and D3 students demonstrated statistically significant changes in attitude in a positive direction at the post-test (p < 0.001), as reflected by a positive delta value (Figure 1). Post-test results demonstrated statistically significant differences between the two groups; with DNHY students indicating more positive attitudes towards EBP (p < 0.001) than D3 students. Overall, students agreed or strongly agreed that EBP should be an integral part of the dental curriculum and that EBP will be valuable in their future to improve the quality of patient care. Attitude domain responses are summarized in Table II.
The pre- and post-survey descriptive summaries reported in Tables II-IV should be interpreted at the group level. Delta values were derived from individual scores rather than group-level summaries. Individual post-survey scores were subtracted from the pre-survey scores to derive the delta value and reflect the direction of change in score with respect to baseline (pre-survey). A zero value indicates no change in the respective domain while a negative value indicates a change in the negative direction. Thus, delta values do not correspond to a direct subtraction of post-survey scores from pre-survey scores. Changes in attitude, access, and confidence are illustrated as boxplots in Figure 1.
Access Domain
DNHY and D3 students did not demonstrate a significant difference in strategies for accessing evidence on the pre-survey (p= 0.110) however post-survey results showed a statistically significant difference (p = 0.004) between the two groups of students. D3 students demonstrated a change in their ability to access information (p < 0.001), while no changes were shown in the DNHY group (p = 0.609) as illustrated in Figure 1. Participant responses regarding frequency of accessing evidence are shown in Table III. Both DNHY and D3 groups reported using colleagues and searching the Internet for dental evidence. Podcasts or databases of critically reviewed topics were rarely used by either group.
Confidence Domain
Confidence levels in appraising various aspects of a published report were not statistically significant between DNHY and D3 groups on the pre-survey (p = 0.157). Both groups reported having moderate confidence on the pre-test and did not differ from each other on the post-survey (p=0.824). Neither group demonstrated a change in confidence that was statistically different (DNHY: p=0.070; D3: p= 0.559). Student responses regarding confidence in the various aspects of appraising the literature are summarized in Table IV.
Discussion
Evidence-based practice is a decision making process that should be considered the standard of care in dentistry and positive perspectives towards EBP should be cultivated early in the education process. The purpose of this study was to evaluate whether current educational strategies at a dental school in the United States made a difference in the dental hygiene and dental students learning outcomes in the four domains of EBP; knowledge, attitude, accessing evidence, and confidence. The study results demonstrated that there were no differences in the EBP domains between the DNHY and D3 groups at the beginning of the research design course; a finding that was noteworthy considering the different academic requirements of the two disciplines. These results were also in contrast to the studies of Stanley et al6 and Hendricson et al,15 both demonstrating positive associations between the degree level of education obtained and EBP knowledge, access to evidence and confidence. The collective responses of both student groups revealed that only a small number of respondents had a fundamental knowledge of pertinent EBP principles, findings similar to Straub-Morarend et al multi-institutional, cross-sectional study of 138 students from seven schools.16 In the area of EBP principles, participants in this study had the highest level of correct responses in being able to differentiate between the terms prevalence and incidence and in literature search strategies while the lowest level of correct responses was in determining the level of evidence and the necessary study design.
This study evaluated the change in EBP knowledge that occurred over a 12 week course and the survey results indicate that both DNHY and D3 student groups demonstrated the same increase in levels of knowledge. These findings were modest in comparison to Hendricson et al15 study findings where participants demonstrated a doubling of knowledge after an EBD training course as measured by the KACE survey instrument. It is noteworthy that the learning objectives of the EBD training were specifically addressed to all components of the KACE knowledge domain,15 whereas the research design course in the current study was an overview of the basic concepts and principles related to both evaluation and conducting research in dental education and biomedical sciences.
The attitudinal change towards EBP in dentistry in both student groups was significant. Both DNHY and D3 students started with a less positive perspective towards EBP and demonstrated transitioning to a more positive outlook. A positive perspective can impact behavior, as one is likely to achieve better in an area that provides enjoyment and views as useful.17 This concept is also supported by studies in other disciplines demonstrating that an attitude index may be used as a positive predictor for better behavior.18 Developing positive attitudes towards EBP are desirable learning outcomes since they may influence the future practitioner's implementation of EBP.
Participants in the study accessed a variety of sources in search for evidence and frequently referred to colleagues and other health care providers for evidence-based information. This is to be expected in an educational environment where classmates or faculty members are readily available for sharing opinions; however, these colleagues may not be accurate sources of evidence. Neither the DNHY nor the D3 groups demonstrated changes in confidence levels in the post-survey. Both groups remained only moderately confident in their ability to appraise various aspects of published research despite the increase in their knowledge and improved attitude. These findings are supported by other educational studies indicating no significant relationship between confidence and levels of knowledge or on the self-rated abilities of health care providers and teachers.19,20
Limitations of the study include the use of a convenience sample of students in a single institution; therefore the results are not generalizable outside of this institution. Additionally, although the two student groups took the research design and statistics course together during the 12-week summer term, there were differences in the overall didactic exposure during that period that may have affected the results. The DNHY students also took a cariology class during the same term that included EBP concepts while the D3 took the cariology course in the previous year. Areas for further study include multi-institutional, cross-sectional surveys of dental hygiene students and faculty on their perceptions of EBP, learning outcomes of EBP in the curriculum and readiness to incorporate EBP in the future.
Conclusion
This study evaluated the changes in knowledge, attitudes, evidence-accessing methods and confidence of EBP in dental hygiene and dental students over a short period of time at a U.S. dental institution. Within the limitations of this study, it can be concluded that dental hygiene and dental students increased their knowledge and developed more positive attitudes towards EBP following a 12 week research design and applied statistics course. Study results identified improvement areas for EBP knowledge acquisition including determining levels of evidence, analysis of study results, and evaluating the appropriateness of research study designs through the use of validated EBP survey instrument.
About the Authors
Victoria Santiago, RDH, BS; Melissa Cardenas, RDH, BS; Anne Laure Charles, RDH, BS; Estefany Hernandez, RDH, BS; are graduates from the Department of Dental Hygiene; Udochukwu Oyoyo, MPH is an assistant professor, Dental Education Services; So Ran Kwon, DDS, MS, PhD, MS is a professor and director of the Student Research Program, Center for Dental Research; all at Loma Linda University School of Dentistry, Loma Linda, CA.
Corresponding author: So Ran Kwon, DDS, MS, PhD, MS; sorankwon@llu.edu
References
1. American Dental Hygienists' Association. Policy manual [Internet]. Chicago: American Dental Hygienists' Association; c2017. [cited 2017 April 24] Available from: https://www.adha.org/resources-docs/7614_Policy_Manual.pdf
2. Sackett DL, Strauss SE, Richardson WS, et al. Evidence-based medicine: how to practice and teach EBM. London: Churchill Livingstone, 2000; p3-5.
3. Bertolami CN. Creating the dental school faculty of the future: a guide for the perplexed. J Dent Educ 2007 Oct;71(10):1267-80.
4. Hendricson WD, Cohen PA. Oral health care in the 21st century: implications for dental and medical education. Acad Med 2001 Dec;77(12):1181-206.
5. Brancato VC. An innovative clinical practicum to teach evidence-based practice. Nurse Educ. 2006 Sept-Oct;31(5):195-9.
6. Stanley JL, Hanson CL, Van Ness CJ, Holt L. Assessing evidence-based practice knowledge, attitudes, access and confidence among dental hygiene educators. J Dent Hyg. 2015 Oct;89(5):321-329.
7. Ciancio MJ, Lee MM, Krumdick ND, et al. Self- perceived knowledge, skills, attitudes, and use of evidence-based dentistry among practitioners transitioning to dental educators. J Dent Educ. 2017 Mar;81(3):271-77.
8. Werb SB, Matear DW. Implementing evidence-based practice in undergraduate teaching clinics: a systematic review and recommendations. J Dent Educ. 2004 Sept;68(9):995-1003.
9. American Dental Association. Center for evidence- based dentistry [Internet]. Chicago: American Dental Association; c2017. [cited 2017 April 24]. Available from http://ebd.ada.org/en/about.
10. McGlone P, Watt R, Sheiham A. Evidence-based dentistry: an overview of the challenges in changing professional practice. Br Dent J. 2001 Jun;190(12):636-9.
11. Kao RT. The challenges of transferring evidence-based dentistry into practice. J Evid Based Dent Pract. 2006 Mar;6(1):125-8.
12. Oxman A, Flottrop S. An overview of strategies to promote implementation of evidence- based health care. In Silagy C and Haines A (eds) Evidence based practice in primary care. London: BMJ Books, 1998; p 5-12.
13. Haines A, Donald A. Making better use of research findings. Br Med J. 1998 Jul;317(7150):72-75.
14. Commission on Commission on Dental Accreditation. Accreditation standards for dental hygiene education programs [Internet]. Chicago: American Dental Association.c2013. [cited 2017 April 24] Available from: http://www.ada.org/~/media/CODA/Files/dh.pdf?la=en.
15. Hendricson WD, Rugh JD, Hatch JP, et al. Validation of an instrument to assess evidence- based practice knowledge, attitudes, access, and confidence in the dental environment. J Dent Educ. 2011 Feb;75(2):131-44.
16. Straub-Morarend CL, Wankiiri-Hale CR, Blanchette DR, et al. Evidence-based practice knowledge, perceptions, and behavior: A multi-institutional, cross-sectional study of a population of U.S. dental students. J Dent Educ. 2016 Apr;80(4):430-8.
17. Eshun BA. Sex-differences in attitude of students towards Mathematics in secondary schools. Mathematics Connection. 2004 Jan;4(1):1-13.
18. Barroso V, Caceres W, Loftus P, et al. Hand hygiene of medical students and resident physicians: predictors of attitudes and behaviour. Postgrad Med J. 2016 Sep;92(1091):497-500.
19. Johnson-Lynn S, Townshend D. How knowledge relates to confidence in orthopedics and emergency medicine regarding return to sport and rehabilitation in foot and ankle trauma. J Surg Educ. 2017 July-Aug;74(4):748-753.
20. Stark HL, Snow PC, Eadie PA, Goldfeld SR. Language and reading instruction in early years' classrooms: the knowledge and self-rated ability of Australian teachers. Ann of Dyslexia 2016 Sept;66(1):28-54.