You must be signed in to read the rest of this article.
Registration on CDEWorld is free. Sign up today!
Forgot your password? Click Here!
In the past 20 years there has been a dramatic change in the way dental practices operate. While the principles of prophylactic and operative dentistry remain essentially unaltered, advances in instrumentation and technology coupled with material research and development have elevated both patient care and practice growth.
Many new technologies allow for common procedures to be completed more efficiently. Because of the time saved on each procedure, additional work that needs to be done can sometimes be completed during the same appointment. Practitioners then do not have to clear time in their schedule for another procedure and patients do not need to delay treatment. For example, during a routine hygiene check, if a small amount of occlusal decay is found, a hard tissue laser can be used to remove it without the need for anesthesia or an additional appointment.1
New technology can also increase the scope of what practitioners are capable of in regards to new procedures. For example, a cone-beam computed tomography unit (CBCT) and computer-assisted design/computer-assisted manufacturing (CAD/CAM) technology could allow a general practitioner-with appropriate training-to expand into the discipline of implant placement via treatment planning software and surgical guides. CBCT can also be used to evaluate canals for endodontic procedures, plan orthodontic procedures, and even to check for anatomical abnormalities that may contribute to breathing disorders, while CAD/CAM can design appropriate appliances to help treat sleep apnea resultant from such disorders.2-5
Lastly, adopting new technology has the potential to attract new patients as well as improve retention rates and case acceptance. There are many people who go out of their way to buy and use the latest technology, and in many instances they are looking for cutting-edge technology in their health care as well. Offering a wide array of procedures incorporating different types of technology can be a differentiator between practices, and could even be the difference maker in long-term practice success. This article will review some of these technologic and material innovations and their application in general practice.
Technology to Aid in Detection
Digital radiography has already had a widespread impact on dentistry with approximately 60% of dental practices in the United States using digital radiography to produce 2-dimensional images.2 Diagnostically comparable to film images, the advantages of digital radiography over the traditional analog model include:2
• secure digital storage and transfer of records
• instantaneous availability of the image files
• absence of labor-intensive chemical processing
• increased patient comfort.
As an adjunct to 2-dimensional digital radiography systems, the use of 3-dimensional radiographs can present an attractive option. A CBCT system can be used to produce a 3-dimensional image to enhance or augment diagnostic capabilities.3 While adherence to the ALARA (as low as reasonably achievable" principle for all ionizing radiation modalities is the clear best practice to minimize patient radiation exposure, CBCT units impart doses approximately the same as 2-dimensional digital units, and indeed all digital imaging technology for oral healthcare produce far less exposure than medical CT units.3 When used as appropriately indicated, both 2-dimensional and 3-dimensional digital radiographic technology provide practitioners access to oral and maxillofacial information that can be beneficial in the diagnosis of osseous degradation, root pathologies, fractures, and pathologies, as well as the aforementioned capacity to expand into implant surgical, orthodontic, or endodontic procedures.3-5
For practitioners interested in non-ionizing solutions to enhance diagnostic capabilities, another adjunctive tool to help aid in detection is a transillumination device. Transillumination technology can be used as a supplement to the clinical and/or radiographic examination to find interproximal and occlusal caries and to evaluate fractures, as well as to illuminate root canals and periodontal lesions.6 Transillumination can also be used to minimize exposure to ionizing radiation or with patients who are radiographic or X-ray phobic and do not want any kind of ionizing radiation used.6 A consent form may be needed, but because the patient will not be exposed to ionizing radiation there is rarely refusal.
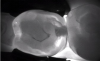
Transilluminating technologies emit light at the base of the tooth at the gingival area and transmit light up through the tooth. At the applied wavelength, enamel starts to absorb fewer photons and water starts to absorb more photons, so lesions appear as dark areas on a monitor.6-8 This visualization can be helpful not only for the clinician to identify and diagnose problematic areas (Figure 1), but it also allows patients to see all aspects of their mouth including their cheek, tongue, and tooth, as well as the areas that have decay, thereby potentially assisting in case acceptance.
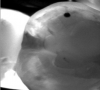
Transillumination can be used in interproximal, occlusal, and anterior surfaces.5 In many cases the technology is able to show how expansive the decayed area is on occlusal areas that may only have a minimal pit that would not allow a probe to be used (Figure 2 through Figure 4). Visualizing the interproximal regions of posterior teeth is possible as well although this may require a specialized fiber-optic tip.6
One of the main benefits that transillumination provides is the ability to be flexible in practice. Decay and problems can be seen at an earlier stage than with radiography, 6 which allows the practitioner to be aware of the clinical situation and decide what the best course of action is: whether to monitor for follow-up or proceed with treatment.
Tools to Aid in Removal of Diseased Tooth Structures
Once relegated to soft tissue procedures, advances in dental laser technology have ushered a paradigm shift in their capability to assist clinicians in hard tissue procedures. Hard tissue and all-tissue lasers include erbium (Er,Cr:YSGG and Er:YAG), and more recently CO2 9,300 nm models. The ablating action of lasers occurs via the evaporation of water within tissues, achieved via chromophoric absorption of specific wavelengths of light.1 The principal chromophores in dental hard tissues are water and hydroxyapatite. Erbium lasers have the highest absorbance in hydroxyapatite and high water absorption, making them the primary choice for hard tissue procedures.1,9
All-tissue lasers typically do not require the use of local anesthesia in the tooth, and in many cases with use in soft tissue, there is predominantly no bleeding.10,11 All-tissue lasers allow for 4- quadrant dentistry, same-day fillings, and fewer bite adjustments.11,12 Its use in practice also allows for new procedures to be performed, including fibromas, gingivectomies, crown lengthenings, and periodontal surgeries.10
Utilizing lasers in practice also increases efficiency. Consider a subgingival class V-a procedure that in the author's experience can take up to 35 minutes (Figure 5). The treatment includes administering anesthetic, waiting for the anesthesia to take effect, subsequently removing soft tissue with either high- or low-speed electrosurgery or with a diode laser to get tissue out of the way to create a clean margin on the gingival aspect of that restoration, removing decay, achieving hemostasis, and finally restoring the tooth. This process can result in swelling, soreness, or sensitivity for the patient, in addition to the potentially off-putting experience of the noise and vibration created by the turbine.
Utilizing a laser, however, the author has consistently reduced the procedure time down from 35 minutes to approximately 10 minutes (Figure 6). This is possible because the wait time while the anesthetic takes effect is mitigated as well as because the laser can remove tissue at the same time as decay.12 In addition, the author reports bite adjustments rarely need to be done because the patient is not numb so they are able to accurately articulate the bite and how it feels. Not relying on anesthesia also allows the dentist to work on multiple quadrants at one time, further increasing efficiency and freeing up chairtime for other patients and procedures.12
New Composites to Aid in Restoration
Among other things, flowable composite resins are useful for minimally invasive occlusal Class I and interproximal Class II restorations, Class V abfractions; pit and fissure sealing; and as cavity liners.13 In the traditional posterior restoration model, the flowable is placed in the bottom of the preparation and a composite is layered incrementally over the top, curing each layer, to provide strength and wear resisitance.13 Critical to success in these restorations completely cured before moving on, which can induce stresses and voids.14,15 Therefore, the author believes that one of the most important aspects when choosing a composite material, whether its anterior or posterior, is finding something that cures quickly and is single increment. Utilizing one material to fill up the entire box minimizes the possibility of voids which is why a bulk fill placement is becoming increasingly popular.16
One option that combines the strength of a bulk fill with the maneuverability and control of a flowable is to use a sonicated composite. Sonicated composites take a specialized composite material and impart sonic energy into it so that it comes out initially like a flowable and penetrates hard to reach areas, then when the energy has taken off, it resorts back to a more dense or more viscous composite.17 This type of deposit allows for a high depth of cure up to 5 mm at a time as well as a decrease in shrinkage.17,18 In the author's opinion, the aesthetics of the material are also much improved over traditional bulk fill materials, making it appropriate for both posterior restorations and also anterior/esthetic dental work (Figure 7 through Figure 9).
Conclusion
Dental technology and materials continue to evolve and revolutionize clinical options for delivery of care. In the hands of trained and experienced clinicians, technology such as digital imaging, lasers, and next-generation composites can pay dividends not only in practice efficiency and practice growth, but-most importantly-in improved clinical outcomes as well as optimal patient care and experience.
About the Author
Scott Coleman, DDS, is a clinical adjunct professor at the University of Texas Health Science Center at Houston. He maintains a private practice in Houston, Texas.
References
1. Verma SK, Maheswari S, Singh RK, Chaudhari PK. Laser in dentistry: an innovative tool in modern dental practice. Natl J Maxillofac Surg. 2012;3(2):124-132.
2. Farman AG. Digital radiography in dental practice. Inside Dentistry.2016;12(11):26-27.
3. Serota K. Cone beam computed tomography: how safe is CBCT for your patients. Dental Economics. 2011;101(1). Available at: https://www.dentaleconomics.com/articles/print/volume-101/issue-1/features/cone-beam-computed-tomography-how-safe-is-cbct-for-your-paitents.html. Accessed May 27, 2018.
4. Surapaneni H, Yalamanchili PS, Yalavarthy RS, Reshmarani AP. Role of computed tomography imaging in dental implantology: an overview. J Oral Maxil Radiol. 2013;1(2):43-47.
5. Tally T. AAE/AAOMR recommendations for the use of CBCT in endodontics. Inside Dentistry. 2017;13(9):40-47.
6. Strassler HE, Pitel ML. Using fiber-optic transillumination as a diagnostic aid in dental practice. Compendium. 2014;35(2):80-88.
7. Friedman J, Marcus MI. Transillumination of the oral cavity with use of fiber optics. J Am Dent Assoc. 1970;80(4):801-809.
8. Wenzel A. Dental Caries. White SC, Pharoah MJ, editors. , Oral radiology: principles and interpretation. UK, PA: Mosby Elsevier; 2008. pp 270-281
9. Kumar G, Rehman F, Chaturvedy V. Soft tissue applications of Er,Cr:YSGG laser in pediatric dentistry. Int J Clin Pediatr Dent. 2017;10(2):188-192.
10. Academy of Laser Dentistry. Laser overview. Available at: https://www.laserdentistry.org/index.cfm/patients/Patient%20Laser%20Overview. Accessed June 13, 2018.
11. Weintraub JP. The versatility and practicality of an all-tissue dental laser. Inside Dentistry. 2016;12(10):62-63.
12. Spector AM. The benefits of using a CO2 all-tissue laser in dentistry. Dentistry Today. 2017. Available at: http://www.dentistrytoday.com/news/todays-dental-news/item/2689-the-benefits-of-using-a-co2-all-tissue-laser-in-dentistry. Accessed June 13, 2018.
13. Baroudi K, Rodrigues JC. Flowable resin composites: a systematic review and clinical considerations. J Clin Diagn Res. 2015;9(6):ZE18-ZE24.
14. Davidson CL, Feilzer AJ. Polymerization shrinkage and polymerization shrinkage stress in polymer-based restoratives. J Dent Res. 1997;25:435-40.
15. Millar BJ, Nicholson JW. Effect of curing with plasma light on the properties of polymerizable dental restorative materials. J Oral Rehabil. 2001;28:549-52.
16. Olitsky J. No shrink? No stress? No problems. Dental Economics. 2017. Available at: https://www.dentaleconomics.com/na/ivovlar-vivadent/no-shrink-no-strees-no-problems.html. Accessed June 13, 2018.
17. Jarisch J, Lien W, Guevara PH, Greenwood WJ, Dunn WJ. Microcomputed tomographic comparison of posterior composite resin restorative techniques: sonicated bulk fill versus incremental fill. Gen Dent. 2016;64(5):20-23.
18. Christensen GJ. Advantages and challenges of bulk-fill resins. Clinicians Report. 2012;5(1):1-2.