You must be signed in to read the rest of this article.
Registration on CDEWorld is free. Sign up today!
Forgot your password? Click Here!
In recent years, different ceramic systems have been introduced for all types of indirect restorations, from conservative no-preparation veneers to multiple-unit posterior fixed partial dentures. With the variety of choices available, it can be difficult to analyze the advantages and disadvantages of the systems based solely on product literature. An analysis of the laboratory and clinical data along with knowledge of the material structure can provide the foundation to make intelligent choices for given clinical situations. Esthetics, preparation requirements, reliability, and mechanical properties may all be determined by the microstructure and processing of the material.
Ceramics are nonmetallic inorganic materials. Numerous materials are referred to as ceramics, including metal oxides, borides, carbides, and nitrides, as well as complex mixtures of these materials.1 The structure of these materials is crystalline, displaying a regular periodic arrangement of the component atoms, and may exhibit ionic or covalent bonding. Ceramics can be quite strong, but they are also extremely brittle-after minor flexure, they will experience catastrophic failure. Although the materials are strong in compression, they are weak in tension.2
Ceramics vary from translucency to opacity. In general, the glassier the microstructure (ie, noncrystalline), the more translucent the ceramic will appear, and conversely, the more crystalline the microstructure, the more opaque the ceramic will be. Other factors that affect translucency include particle size, particle density, refractive index, and porosity.3
A first step in choosing a material is to look at the mechanical and physical properties to see how a particular material may match the stress and preparation constraints for a specific clinical situation. The properties of a material may be simplified to derive from the interaction of fabrication method (processing), composition (material type), and microstructure (crystal, glass, etc). These components all play a role in determining the esthetics, fit, strength, biocompatibility, and reproducibility of a given restorative system. Furthermore, data of older materials can be examined to make predictions concerning new materials if there are similarities in the microstructure, processing, and composition. Presently, most all-ceramic systems fall into three major categories: conventional/reinforced feldspar-based, castable/machinable glass-ceramics, and high-strength machinable polycrystalline materials (zirconia, alumina).
Glass-Ceramics Structure (General Dentistry)
The microstructure of glass-ceramic materials consists of a glass matrix surrounding a second phase of individual crystals (Figure 1). The material starts out as a homogeneous glass. A secondary heat treatment nucleates and grows crystals, which gives this class of materials improved mechanical and physical properties because of the physical presence of the crystals and generation of compressive stress around the crystals due to crystal growth and often a slight mismatch of thermal expansion values.4 Glass-ceramics generally have improved properties such as increased fracture resistance, improved thermal shock resistance, and resistance to corrosion. Improvements in properties are dependent on the interaction of the crystals and glassy matrix, as well as on the crystal size and amount. Finer crystals generally produce stronger materials.
A fundamental method of improving strength and fracture resistance is to add a crystal to a glass material, which is known as dispersion strengthening. The crystals may act as roadblocks to crack growth. A crack growing from a defect must go through or around the crystal, which takes some energy away from the propagating crack and may stop it from continuing through the material.1Thus the restoration may continue to function instead of being cracked in half. In addition to the roadblock effect, compressive stresses around the growing crystals may also help pin cracks and further enhance fracture resistance. Therefore, glass-ceramics are used for cookware, missile nose cones, and even heat shields on space vehicles.
Although glass-ceramics may seem to be ideal materials, the composition and crystal structure must be correctly fabricated for the application or the improved properties will not develop. There are two methods of processing these materials into restorations: pressing and machining.
Processing: Pressable Ingots
Pressing of restorations uses a conventional lost wax technique, except crystallized ceramic ingots are used instead of metal, along with a special investment material. The ingots are supplied in several shades, including multicolor layered ingots. A choice of two techniques may be employed to fabricate the restoration. The restoration may be cast to its final contours and subsequently stained and glazed to provide an esthetic match.
Alternatively, a coping may be pressed on which porcelain is added to achieve the final shape and shade of the restoration. It should be noted that external colorations and glazes wear off clinically. Longevity is dependent on what the patient eats and drinks, along with the patient's tooth-brushing habits, including type of bristle and toothpaste. Laboratory-based and clinical longitudinal studies involving full-contour stained ceramic crowns placed anteriorly and posteriorly have demonstrated a color shift as early as 2 years later due to abrasion of the stain.5-7
During pressing, a "reaction layer" develops because of interaction between the molten ceramic and the investment material. It is very opaque and porous and must be removed entirely by the laboratory. What difference does this make clinically? A larger reaction layer may be more difficult to remove and potentially create defects that are not completely eliminated. These defects may subsequently open during function in the mouth, leading to early and unexpected failure of the entire restoration or chipping in the defect area (Figure 2).8,9 Additionally, different materials have variations in flow during pressing that may affect the accuracy of the restoration, particularly in thinner areas, such as the margin.10
Processing: Machining
CAD/CAM has become an efficient and reliable method of fabricating ceramic restorations. Glass-ceramics may be fabricated in block form and machined into final form from a digital file of the restoration, developed using intraoral scans of the preparation or cans of casts/physical impressions. Considerations for machined restorations include chipping of the material and post-machining processing. Some glass-ceramics require a firing cycle to crystallize the material after machining, while others are already crystallized and do not require a secondary heat treatment to complete crystal growth. Lithium-disilicate materials require crystallization after machining, whereas lithium-silicate materials do not require an additional crystallization cycle: they may be simply polished, but if desired, the lithium silicate may be heat treated to maximize strength.
Dental Glass-Ceramics Development
Historically, the first widespread use of glass-ceramics and full ceramic restorations was a fluoromica-based material called Dicor® developed by Corning Glass Works.11 Although this system is no longer available, much was learned from it regarding the handling of glass-ceramic materials. Dicor suffered from a high failure rate when cemented with zinc-phosphate cement, especially in the posterior region-as high as 70% within 5 years.12 However, when the Dicor was acid-etched and then cemented with a composite resin, cement failure rates dropped to roughly half those experienced with zinc phosphate.13Although present glass-ceramics in a higher thickness of 1.5 mm may be cemented without bonding (glass-ionomers/resin-ionomers), it is recommended that bonding procedures be followed for glass matrix-based materials, including leucite-reinforced feldspathic ceramics, particularly in thinner restorations.14,15 The author personally believes the additional reinforcement of both the restoration and the tooth with proper bonding techniques is worth the extra time that may be needed for this procedure.
Improvements in this class of materials have been based on increasing the crystal content of feldspathic porcelain. A leucite-crystal content of approximately 45% to 50% reinforces the glass matrix by helping deflect or pin cracks and prevent catastrophic failure of the material. The most widely used version is the pressable ceramic Empress® (Ivoclar Vivadent, ivoclarvivadent.com). Other products with properties and microstructure similar to Empress include Finesse® (Dentsply, dentsply.com), Authentic® (Jensen, jensendental.com), PM™9 (Vita, vident.com), and OPC® (Pentron, pentron.com). A machinable version, the Empress CAD (Ivoclar) system for high-leucite ceramics, has performed well clinically when used for posterior inlays and onlays, as well as anterior veneer and crown restorations. Paradigm™ C porcelain block (3M ESPE, 3mespe.com) has similar properties. Machinable and pressable systems have much higher fracture resistance than powder/liquid systems and have shown excellent clinical results for posterior inlay and onlay applications and anterior veneer and crown restorations.16-22
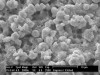
Research has continued to improve dental glass-ceramics. About 15 years ago, materials with a completely different chemistry and with higher fracture resistance were introduced based on a lithium-disilicate chemistry. Ivoclar introduced this material initially as Empress II and now in the form of IPS e.max® pressable and machinable ceramics. Increasing the crystal content to approximately 70% and refining the crystal size improved mechanical and physical properties. The glass matrix consists of a lithium silicate with μm-size lithium-disilicate crystals in between, which are sub-μm lithium-orthophosphate crystals (Figure 3). This structure creates a highly filled glass matrix.23 A lithium-disilicate material with similar properties and structure called 3G OPC is available as a pressable glass-ceramic from Pentron.
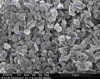
Recently, glass-ceramics with a different microstructure and chemistry have been developed to further refine crystal structure. The innovations in Celtra® Duo and Celtra Press (the newest pressable version of Celtra created for dental laboratories) (Dentsply Sirona) involve changes in the chemistry and crystal structure of lithium-based glass-ceramics. Other products in this category include Suprinity® (Vita). The material is a 10% zirconia silicate-reinforced glass-ceramic (ZLS). The lithium-silicate material has dissolved particles of zirconia that help decrease mean crystal size to approximately 0.5 μm, with even finer sub-μm crystals between the larger ones (Figure 4).24
Obsidian® is also a relatively new glass-ceramic based on lithium silicate. It is provided in a partially crystallized state that contains some zirconia but reportedly also contains germanium dioxide to aid in crystallization (Glidewell Laboratories, glidewelldental.com).25
In the creation of dental materials, manufacturers seek substances that resist crack growth. Among the primary goals is for restorations to behave like natural teeth that can sustain damage but also successfully exist for years without failure. When selecting materials, flexural strength is just one component to consider.
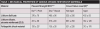
One of the principal concerns with using ceramic materials is their ability to resist stress in the mouth. Methods to examine this include flexural strength, fracture toughness, and failure load of actual crowns.26-29 Although zirconia-reinforced lithium silicate (ZLS) is a relatively new material, research has been done to examine these various areas. The mechanical properties of glass-ceramics have been tested using different methods according to ISO Standard 6872, fracture toughness, and load to failure of maxillary incisor crowns.4,26-29
The overall conclusion from the research is that the refined microstructure of ZLS appears to improve properties in all categories important to long-term clinical success. Of particular importance is toughness and load to failure of actual crowns. The geometry of restorations is very complex and cannot be replicated by disc and bar specimens used for standardized strength testing. Although bar testing and disc testing are helpful in evaluation, testing of crown failure resistance as used clinically is extremely important. ZLS has been shown to be highly resistant to aging, indicating a strong resistance to the stresses of oral activity over time (Table 1).4,26-31
Other properties to contemplate for a given clinical case include fracture resistance, color stability, polishability/gloss, margin integrity, and creation of a smooth "wear-kind" surface free of subsurface defects. From an esthetic standpoint, color stability and a chameleon effect are very important.
Color stability on firing of finished restorations is an important consideration for shade matching. It is often necessary to apply additional colorants (stains) to get the best match to the patient's teeth adjacent to the restorations. A key issue with glass-ceramics, or any ceramic, is to maintain both the structure and color on repeated firings.
In an examination of color stability, color was measured with a spectrophotometer to determine the values in color space: value, red-green, and blue-yellow. An equation was used to determine the position in color space, called ∆E. Color testing has shown that a ∆E value of 2 to 4 can be seen by most people as a clinically obvious difference in color.32 Additionally, gloss was measured of polished restorations and those subjected to prophylaxis that occurs routinely when patients visit the hygienist.33 ZLS material was shown to maintain color, even over repeated firings.32
In the processing of ZLS and lithium-disilicate materials, significant differences have been seen. With respect to pressing, the flow of ZLS appears to be improved, allowing finer structures to be produced. The amount of reaction layer is smaller for ZLS compared with lithium disilicate, resulting in less adjustment required by the laboratory. This layer is a function of material type and investment type due to a chemical reaction between the material and investment. Some investment materials claim reduction in the reaction layer, but the claims have not been independently proven. Some technicians also report that lowering the pressing temperature can reduce the layer; however, this may then affect the microstructure of the restoration. Overall, it is dependent primarily on the ceramic type. In general as the reaction layer decreases, surface finish improves and residual defects are decreased.8,9
Machinable versions also present different pathways, with variations in post-machining requirements and options. Lithium disilicate is machined in a low/partial-crystal state and must be heat-treated after grinding. Machining in the fully crystallized state is a lengthy process and creates excessive chipping damage.34,35 The cycle is critical, with hold time at the crystallization temperature of about 840°C being crucial for proper crystal and shade development as well as surface glazing.36 Also, refractory material support is needed to prevent distortion during the cycle. If timing is too short, under-crystallization may result in a soluble material and incorrect color. Therefore, using the proper cycle in a calibrated furnace is vital for achieving proper mechanical and optical properties.37,38 Pressable ingots are pre-crystallized, whereas the blocks are not and require a heat cycle to be fully crystallized. Thus for lithium-disilicate materials there is a large difference between the block form and press form.
In contrast, ZLS is provided fully crystallized, eliminating the requirement of a post-machining crystallization cycle. The material may be machined and then polished. Alternatively, it may be treated with a specified secondary heat cycle to maximize mechanical properties.39
Conclusion
Ceramic materials are in widespread use, with a myriad of choices available. The material that is selected should be designed to maximize the esthetics and longevity of the restoration for the patient. Glass-ceramics can provide reliable restorations with long-term success. Fabrication of restorations may be performed by pressing or machining. Research into these materials continues, with improvements in properties seen in the latest type, ZLS. New zirconia-reinforced glass-ceramics have refined microstructures designed to improve mechanical and physical properties that may enhance the ability to provide a reliable long-term positive clinical outcome for patients.
References
1. Kingery WD, Bowen HK, Uhlmann DR. Introduction to Ceramics. 2nd ed. New York, NY: John Wiley and Sons; 1976.
2. Anusavice KJ, Shen C, Rawls HR. Phillips' Science of Dental Materials. St. Louis, MO: Elsevier; 2014.
3. McLean JW, Hubbard JR, Kedge MI. The Science and Art of Dental Ceramics. Vol. 1: The Nature of Dental Ceramics and Their Clinical Use. Chicago, IL: Quintessence; 1980.
4. Frieman S. ASM Engineered Materials Handbook Vol 4: Ceramics and Glasses.ASM International; 1991.
5. Stappert CF, Guess PC, Chitmongkolsuk S, et al. All-ceramic partial coverage restorations on natural molars. Masticatory fatigue loading and fracture resistance. Am J Dent. 2007;20(1):21-26.
6. Garza LA, Thompson G, Cho SH, Berzins DW. Effect of toothbrushing on shade and surface roughness of extrinsically stained pressable ceramics. J Prosthet Dent. 2016;115(4):489-494.
7. Rodrigues CRT, Turssi CP, Amaral FLB, et al. Changes to glazed dental ceramic shade, roughness, and microhardness after bleaching and simulated brushing. J Prosthodont. 2017. doi:10.1111/jopr.12663
8. Park J, Anusavice KJ, Shen C. Influence of investment/ceramic interaction layer on interfacial crack propagation in veneered lithia-based ceramic [abstract]. J Dent Res. 2002 (spec iss A). Abstract 1179.
9. Daizaburo M, Tomohiro K, Tatsuya F, et al. Evaluation of surface roughness of two press ceramic systems [abstract]. J Dent Res. 2017;96(spec iss A). Abstract 3203.
10. Rampf M, Dittmer M, Ritzberber C, et al. Properties and crystallization phenomena in Li2Si2O5-Ca5(PO4)3F and Li2Si2O5-Sr5(PO4)3F glass-ceramics via twofold internal crystallization. Front Bioeng Biotechnol. 2015;3:122. doi:10.3389/fbioe.2015.00122.
11. Grossman DG. Tetrasilicic mica glass-ceramic material. U.S. Patent No. 3732087; 1973.
12. Ellison JA, Lugassy AA, Setcos JC, Moffa JP. Clinical trial of cast glass ceramic crowns, seven year findings. J Dent Res.1992;71(spec iss):207.
13. Malament KA, Grossman DG: Bonded versus non-bonded Dicor crowns. J Dent Res. 1992;71(spec iss):321.
14. Bindl A, Lüthy H, Mörmann WH. Strength and fracture pattern of monolithic CAD/CAM-generated posterior crowns. Dent Mater. 2006;22(1):29-36.
15. Preis V, Behr M, Hahnel S, Rosentritt M. Influence of cementation on in vitro performance, marginal adaptation and fracture resistance of CAD/CAM-fabricated ZLS molar crowns. Dent Mater. 2015;31(11):1363-1369.
16. McLaren EA, Giordano RA. Zirconia-based ceramics: material properties, esthetics, and layering techniques of a new veneering porcelain, VM9. Quintessence Dent Technol. 2005;28:99-111.
17. Wagner J, Hiller KA, Schmalz G. Long-term clinical performance and longevity of gold alloy vs ceramic partial crowns. Clin Oral Investig. 2003;7(2):80-85.
18. Brochu JF, El-Mowafy O. Longevity and clinical performance of IPS-Empress ceramic restorations-a literature review. J Can Dent Assoc. 2002;68(4):233-237.
19. Kraemer N, Frankenberger R. Clinical performance of bonded leucite-reinforced glass ceramic inlays and onlays after 8 years. Dent Mater. 2005;21(3):262-271.
20. Manhart J, Chen HY, Neuerer P, et al. Three-year clinical evaluation of composite and ceramic inlays. Am J Dent. 2001;14(2):95-99.
21. van Dijken JW, Hasselrot L, Ormin A, et al. Restorations with extensive dentin/enamel-bonded ceramic coverage. A 5-year follow-up. Eur J Oral Sci. 2001;109(4):222-229.
22. Höland W, Rheinberger V, Apel E, et al. Clinical applications of glass-ceramics in dentistry. J Mater Sci Mater Med. 2006;17(11):1037-1042.
23. Lien W, Roberts HW, Platt JA, et al. Microstructural evolution and physical behavior of a lithium disilicate glass-ceramic. Dent Mater. 2015;31(8):928-940.
24. Ramos Nde C, Campos TM, Paz IS, et al. Microstructure characterization and SCG of newly engineered dental ceramics. Dent Mater. 2016;32(7):870-878.
25. Internal company data. Glidewell.
26. Lawson NC, Bansal R, Burgess JO. Wear, strength, modulus and hardness of CAD/CAM restorative materials. Dent Mater. 2016;32(11):e275-e283.
27. Giordano R. Flexural strength of ceramic materials. In progress; 2017.
28. Badawy R, El-Mowafy O, Tam LE. Fracture toughness of chairside CAD/CAM materials - alternative loading approach for compact tension test. Dent Mater. 2016;32(7):847-852.
29.Schwindling FS, Rues S, Schmitter M. Fracture resistance of glazed, full-contour ZLS incisor crowns. J Prosthodont Res. 2017;61(3):344-349.
30. Apel E, van't Hoen C, Rheinberger V, Höland W. Influence of ZrO2 on the crystallization and properties of lithium disilicate glass-ceramics derived from a multi-component system. J Eur Ceram Soc. 2007;27(2-3):1571-1577.
31. Khalkhali Z, Marghussian VK. Mechanical and chemical properties of Zr and P-doped lithium disilicate glass ceramics in dental restorations. Int J Appl Ceram Technol. 2012;9(3):497-506.
32. Giordano R. Effect of repeated firing on color stability of ceramics. In progress; 2017.
33. Sugiyama T, Kameyama A, Enokuchi T, et al. Effect of professional dental prophylaxis on the surface gloss and roughness of CAD/CAM restorative materials. J Clin Exp Dent. 2017;9(6):e772-e778.
34. Song XF, Ren HT, Yin L. Machinability of lithium disilicate glass ceramic in in vitro dental diamond bur adjusting process. J Mech Behav Biomed Mater. 2016;53:78-92.
35. Fraga S, Amaral M, Bottino MA, et al. Impact of machining on the flexural fatigue strength of glass and polycrystalline CAD/CAM ceramics. Dent Mater. 2017;33(11):1286-1297.
36. IPS e.max Crystallization Cycle Update. Ivoclar Vivadent technical document; 2012.
37. Zhang Y, Kelly JR. Dental ceramics for restoration and metal veneering. Dent Clin North Am. 2017;61(4):797-819.
38. IPS e.max Information for Dentists. Ivoclar Vivadent, Inc; 2016.
39. Celtra Duo Technical Monograph. Dentsply Sirona Inc. http://www.celtraduo.com/content/dam/dentsply/microsites/celtra/CeltraDuo%20tech%20monograph.pdf. Published 2016. Accessed January 19, 2018.