You must be signed in to read the rest of this article.
Registration on CDEWorld is free. Sign up today!
Forgot your password? Click Here!
The Centers for Disease Control and Prevention (CDC) estimates that 1.2 million people age 13 and older are living with Human Immunodeficiency Virus (HIV) infection; one in eight are unaware of their infection.1,2 Nearly 40% of the individuals who are newly diagnosed have a high probability of having been infected years prior to diagnosis, present with advanced states of disease, and will progress to Acquired Immune Deficiency Syndrome (AIDS) within one year.1 Late diagnosis of HIV infection is common in the United States (U.S.) with 33% of people living with HIV developing AIDS within one year of their initial diagnosis.1,2
The number of persons living with HIV infection is growing, indicative of a chronic, manageable disease. New York City (NYC) continues to have one of the largest prevalence of HIV infections in the U.S.3,4 A reported 2,718 people were newly diagnosed with HIV infection in 2014 and 1,432 were diagnosed as having AIDS making a total of 119,550 people living with HIV/AIDS in NYC.4 Disparities in mortality and survival rates of persons living in impoverished neighborhoods are evident, verifying the health inequities across NYC and the need to focus further screening and testing options/opportunities particularly in these areas.4
Salivary components are being used to assist in the diagnosis of oral and systemic diseases.5 The U.S. Preventive Services Task Force (USPSTF) recommends routine HIV screening regardless of risk level, for all persons age 15 to 65 years.5-7 The USPSTF has designated HIV screening as Grade "A", which assures, with high certainty that the net benefit is substantial; currently there are four designated screening grades, with "A" being the highest to "D" being the lowest/not recommended.8 The CDC has expanded Rapid HIV Testing (RHT) initiatives including support for the home test for HIV and as a result, screening has become more accessible to the public.8 Treatment is also centered on prevention which includes routine screening, the use of pre-exposure prophylaxis (PrEP), a Food and Drug Administration approved preventative medicine taken daily, and the single-dose combination antiviral therapy for postexposure prophylaxis (PEP).5,7 Numerous studies have validated the significance of early detection, diagnosis and treatment of HIV-infected individuals resulting in reductions in morbidity and mortality.5,6,8 Additionally, these studies also support the high accuracy rate of the oral RHT method as a suitable screening tool.5,6,8
In support of early disease screenings for undiagnosed medical conditions, studies have been conducted using population data, estimates of chronic disease prevalence, and rates of medication adherence to determine the overall cost savings of early detection. Nasseh et al. investigated the short-term annual health care cost savings when oral health care providers included screenings for various chronic diseases such as diabetes and hypertension.10 Chronic disease prevalence and rates of medication adherence were used to estimate the cost savings for patients 40 years and older and who visited a dentist but had not visited a physician over a period of 12 months.10 Nasseh et al. found that medical screenings in the dental office could potentially save the healthcare system between $42.4 million to $102.6 million over 12 months time and long term monitoring could possibly achieve further savings and health benefits.10
Dental hygienists and dentists can play a significant role in administering chair side health screenings, including HIV and other chronic diseases, as preventive services to aid in early detection and treatment. Educating patients and promoting healthier lifestyles may increase their lifespan and may also reduce the overall burden of health care costs.
Issues regarding HIV testing conducted within dental practice settings has been reported in the literature.7,11 Dentists have expressed concerns about false-positive results, offending patients, view of HIV testing as outside the scope of licensure, low patient acceptance of HIV testing in the dental setting, inadequate reimbursement and potential negative impact on the dental practice.11 A recent survey of general dentists examined their willingness to conduct RHT screening and assessed perceived compatibility with their professional role.7 Significant findings include: 14 out of 1,802 respondents reported offering the RHT in their practices; fewer than one in eight dentists were familiar with 2006 revised CDC guidelines recommending routine HIV screening of patients in health care settings; African American dentists were more than twice as receptive to RHT as part of the dentist's role than Non-Hispanic White dentists.7
The Ryan White HIV/AIDS program is the largest federally funded HIV care and treatment program in the U.S., providing a "safety net" for medical and social services for those individuals affected by the disease with limited or no coverage for the costs of care.12 Ryan White areas are federally designated population centers that are the most severely affected by the HIV/AIDS epidemic.11 Dentists practicing in non-Ryan White areas were shown to be less willing to perform RHT. Results from the electronic survey also demonstrated that the number of training hours received in RHT and counseling correlated with both the willingness to provide and the acceptance of HIV testing as part of their professional role; dentists with more than eight hours of training had almost twice the odds of being willing to provide testing and also deemed testing to be part of their role as a dentist.
Dental hygienists regularly administer oral health assessments, screenings, dental hygiene care planning, education, in addition to providing preventive and individual treatment services. As oral health care providers, dental hygienists routinely screen for hypertension, oral cancer, nutritional habits, and oral manifestations of systemic disease. Their educational background includes a thorough foundation in communicable diseases, thus establishing the dental hygienist as an optimal provider to conduct RHT.13,14 The dental setting is a desirable non-traditional setting for RHT, as almost two-thirds of all Americans see a dental provider annually.15 A national survey measuring dental hygienists' knowledge and attitudes towards RHT determined that dental hygienists, with additional training in HIV prevention and counseling and diagnostic testing, are willing to conduct RHT and therefore may be an appropriate health care provider to conduct this screening.13 Approximately 75% (n=475) of respondents achieved a score of 75% or higher (‘high scorers' group) on the knowledge test, and those remaining, 25.1% had scores under 75% were designated ‘low scorers' group. The only significant difference between the two groups was the ‘higher scoring' group had a higher proportion of participants identifying themselves as White than the low-scoring group (73.3% versus 60.4%, P=0.01). Both groups showed little difference in their opinion of whether dental offices should offer RHT and whether they would be willing to obtain training on RHT administration and counseling. A majority (58.53%) of the high scoring group indicated willingness to conduct RHT if offered within their individual practice setting.
VanDevanter, et al.16 studied patients' attitudes towards HIV testing performed in the dental setting by conducting in-depth interviews of 19 new patients receiving dental care at a NYC University-based dental clinic. Patients were assessed for their attitudes, beliefs, and perceived acceptability of oral RHT in the dental clinic setting. Analysis of qualitative interviews revealed three themes related to patients' views on RHT in dental settings. In regards to acceptability and perceived advantages to HIV testing in dental settings, 74% reported they would accept screening if it were offered as part of the dental visit. Convenience, free of charge, and universally administered (to all patients) were other notable responses by interviewees. Secondly, there was congruence between HIV screening and patients' view of dental settings; many participants perceived it as going "hand-in-hand." Thirdly, there were logistical issues related to implementation including handling positive results, the need for professional counseling services, linkage to the provision of care for HIV-positive patients, privacy concerns and preventive educational materials. Caution is needed in generalizing VanDevanter's study results due to the small sample size, however the authors conclude that RHT in the dental setting is promising for individuals who are unable to access primary care services in traditional settings.
Patient-centered care is considered to be a gold standard in dentistry and is essential throughout treatment. A pilot study seeking to evaluate the patient perspective on RHT was conducted in 2007 in an urban free dental clinic serving a diverse patient population in Kansas City. Patients completed an attitude assessment survey on RHT prior to their treatment. One hundred and fifty uninsured adults living in zip codes with a high prevalence of HIV reported willingness to take a free RHT during their dental visit supporting patients' overall acceptance of HIV screening in the dental setting.17
Dental hygienists are committed health care professionals. There is evidence supporting dental hygienists' willingness and readiness to effectively conduct RHT when provided with the necessary training skill sets. The purpose of this study was to investigate patient acceptability, certainty of their decision, and willingness to pay for screening if RHT was offered in university-based dental hygiene clinics.
Methods
A cross-sectional survey was administered to 426 dental hygiene patients attending one of three NYC dental hygiene clinics representing all of the dental hygiene clinics in NYC. Eligibility criteria included being over 18 years of age and having the ability to read and write in English or Spanish. Data collection took place between November 2013 and February 2014. The survey was implemented by senior dental hygiene students who had completed the Responsible Institutional Conduct of Research (RCR) for Social and Behavioral Research via the Collaborative Institutional Training Initiative (CITI) human subjects' protection training. Participants also received additional training that included roleplaying with a faculty written script, emphasizing the critical nature of maintaining patient confidentiality. Institutional Review Board approval was granted by the University Committee on Activities Involving Human Subjects for New York University (IRB# 13-9662), the City University of New York for NYC College of Technology and Hostos Community College. (IRB#489808-01)
Routine clinical patient protocol which includes a comprehensive review of each patient's medical history was followed. The study was introduced by the student dental hygienist during the medical history review and each interested patient was provided a patient information document outlining the study protocol. Participants provided verbal consent before self-completing the paper-based, chairside survey.
The survey instrument consisted of 17 questions. Seven questions captured respondent demographics including age, gender, ethnicity, highest level of education and residential zip code. Five questions measured HIV testing preferences including acceptability to receive an HIV test in the dental setting, type of HIV test preferred, type of dental provider preferred, history of HIV testing and willingness to pay for an HIV test. Five questions measured the participant's certainty of their decision using the decisional conflict scale.18
Decisional conflict takes place when there is uncertainty about an action. In most cases, an individual becomes uncertain when they are confronted with decisions involving risks or uncertainty of the intended outcomes.18,19 Uncertainty is highest when an individual experiences the following: feels uninformed about the alternative options, risks and benefits; is unclear about their personal values used to make the decision; feels lack of support in making the decision or feels pressured to choose a particular option.18-20
The survey instrument utilized the SURE (Sure of myself, Understanding information, Risk-benefit ratio, Encouragement test version) decisional conflict questions commonly used in clinical settings.21 The four SURE items included: "Do you feel SURE about the best choice for you?; Do you know the benefits and risks of each option?; Are you clear about which benefits and risks matter most to you?; Do you have enough support and advice to make a choice?" The SURE items were summed; scores ranged from zero (extremely high decisional conflict) to four (no decisional conflict). Scores less than or equal to three indicated a decisional conflict.20
Face validity of the survey instrument was assessed by having dental hygiene students and other lay people review the draft tool, while content validity was tested by having oral health and HIV scholars and researchers assess the survey. Psychometric testing was performed on the SURE decisional conflict scale and the instrument was found to be acceptable, feasible and easy to administer. The validity alpha coefficient was found to be 0.86, while the internal reliability was moderate with a Cronbach α of 0.65.18,22
Data analyses were conducted using Statistical Analysis System (SAS) version 9.1. Differences between respondents who were and those who were not willing to have HIV testing in a dental setting were determined by a Chi-square tests statistic for categorical variables (gender, race and education). Age differences between participants who would or would not, or were unsure about receiving HIV testing in a dental setting, were determined by the analysis of variance (ANOVA). Differences in age between participants who had and those who had not been previously tested for HIV as compared to individuals willing to receive HIV testing in a dental setting, was determined by a t-test.
Results
The overall response rate (n=426) was 100%. Of the 426 respondents, nearly three quarters were willing to have HIV testing administered by a dental professional (Table I). Respondents indicating a willingness to accept testing in the dental hygiene clinic were asked follow-up questions; however, some participants chose not to answer all of the survey items. More than half of the respondents indicated having had HIV testing in the past. The testing methods preferred by 285 respondents included the fingerstick (4.91%, n=14), venipuncture (8.77%, n=25), and the oral RHT (85.26%, n=243). Two hundred ninety-three respondents indicated that if HIV testing were offered that they were willing to have testing done by a dentist (72.35%, n=212) or a dental hygienist (71.67%, n=210). Willingness to pay varied, with a third indicating they were not willing to pay for HIV testing (n=88), another third willing to pay $10 (n=87), a quarter were willing to pay $20 (n=69), and 15 percent were willing to pay $30 or more (n=43). Respondents stated they knew the benefits and risks of each testing option (n=216), and were clear about which benefits and risks were most important (n=248). More than half (n=243) believed they had enough support and advice from others to make a choice regarding testing and more than 90% (n=264) reported being sure about the best choice for themselves. The mean decision conflict score was 3.42 out of four (SD 1.08). (see Table I)
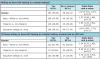
Over half of the study population was comprised of women (n=231), multiple racial groups and educational backgrounds (Table II, Table III). White vs. non-Whites and Hispanics vs. non-Hispanics were compared; individuals with a college education were compared to those without a college education. Demographic differences were determined between those who had and those who had not had HIV testing, in addition to those who were and were not willing to accept HIV testing in a dental clinic setting. Amongst those who would accept HIV testing in a dental clinic, there were no statistically significant differences between the yes, no, and unsure responses when comparing white and Hispanic participants.
There was a significant difference in racial/ethnic distribution between those who previously had HIV testing already and those who did not. Specifically, there were more Whites amongst those who reported having had HIV testing than those who reported never being tested, and more Hispanics amongst those who had received HIV testing than those who had not had testing. No other statistically significant differences were identified based on demographic characteristics of the sample population when comparing those who had been previously tested for HIV and those who had not been tested. (Table II, Table III)
Odds ratios were performed comparing demographic differences between individuals who have and those who have not had HIV testing, as well as those who are and are not willing to have testing in a dental setting. Results demonstrated that Hispanics were more willing to have HIV testing performed in a dental setting than non-Hispanics (OR=1.65, 95% CI: 1.03, 2.64, p= 0.04). No other demographic differences were found between those who were willing to have HIV testing in a dental setting and those who were not or were unsure. Of the individuals who were willing to have HIV testing performed in a dental setting, Whites were less likely than non-Whites to have already had previous HIV testing (OR=0.50, 95% CI: 0.31, 0.81, p= 0.01) and Hispanics were more likely to have been previously tested (OR=3.78, 95% CI: 2.25, 6.33, p= <.0001). (Table IV)
Discussion
Patient acceptance, perceptions and readiness to be screened for HIV is critical to RHT implementation. This study's findings indicate that the majority of dental hygiene clinic patients would be willing to accept HIV screening, perceive it as being important, and are agreeable to undergo screening if offered in the dental setting at no or low cost. The results of this study contribute to the previous research findings indicating patients' willingness to accept HIV screenings administered by dentists in dental clinics at no cost,2,5 as the majority of patients surveyed in these three NYC dental hygiene clinics indicated that they would accept HIV screenings by dental hygienists, and that they would be willing to pay a nominal ($10-$20) fee for this service.
In 2006 the CDC revised its recommendations for HIV screening and testing. Prioritizing settings (including alternative settings) and advocating for screening and testing to become a standard component of a healthcare visit were two important highlights.23 The CDC's inclusion of dental professionals in its preference provides a valuable alternative for patients. Studies on knowledge and willingness to conduct screenings by dentists and dental hygienists have determined the dental setting as an alternative site for consideration.7,14
The CDC estimates that 82.3% of children aged 2-17, 61.6% of adults aged 18-64 and 61.8% of adults aged 65 and older had dental visits in 2012.15 Dental care utilization studies have indicated that more people visit their dental professional on a regular basis than other health care providers, suggestive of dental health care professionals possibly being the only providers visited annually.24 A brief description of three types of HIV testing: venipuncture, a fingerstick for a blood sample and oral swab for saliva, were included in the survey administered in the three dental hygiene clinics and the majority of the respondents interested in HIV screening chose the rapid testing via the saliva collection. Saliva containing biomarkers have many advantages as a diagnostic tool that include: high sensitivity and specificity, simple to perform, rapid results, noninvasive, economical, versatile in handling, storage and transport, and appropriate at chairside when screening for other oral and systemic diseases.26
Hispanics in the study sample, were more willing to have HIV testing in a dental hygiene clinic, and among the participants who were willing to accept testing in a dental hygiene clinic. Hispanic and non-Whites in this study sample also had a higher odds of already having been previously tested for HIV; this finding is consistent with what has been reported in previous studies.17,23 HIV diagnoses, prevalence, care outcomes and survival rates in NYC continue to disproportionately affect certain racial populations; African American (black) are among the highest followed by Hispanic and White.4 Free or low-cost dental clinics serving diverse patient populations are ideal to offer and administer RHT in effort to reach racial groups with high prevalence,17 as demonstrated among the respondent/patient racial characteristics treated at these three NYC dental hygiene clinics.
Despite the findings of this study suggesting that patients would be willing to undergo RHT administered by a dental hygienist in the dental setting, a few limitations can be noted. While 71.7% of participants stated that a preference for RHT administration by a dental hygienist, it is possible these preferences were biased due to the survey being administered by dental hygienists and students in dental hygiene program clinic settings. A convenience sample was used for this study however, a diverse group of participants was involved. While the research instrument gathered participants' geographic information, the data was not evaluated for varied responses based on whether or not the participants resided in urban or suburban areas. It is also unclear if the sample size was an appropriate subset of the total number of dental hygiene patients seen at the three dental hygiene program clinics. Reasons for declining participation and demographics were not gathered from patients who declined to participate in the survey.
Future research should address barriers concerning administering HIV screenings at no or low cost. Further investigation and discussion is also needed to determine the feasibility of incorporating oral rapid HIV testing and education into dental and dental hygiene school curricula. HIV training for all dental professionals in didactic as well as clinical settings should include all aspects of the RHT process and become a permanent, delegable procedure incorporated as one of the professional roles of the oral health care provider.26-28 Patients surveyed in this and previous studies indicate acceptance of the potential offer for oral rapid HIV screening at no or low cost when provided in public dental hygiene clinics, however further investigation and comparison should be considered for those patients receiving care in private practice dental settings.16,17
Conclusion
Patients are willing to undergo oral RHT when offered as a service and provided by dental hygienists in the dental setting. These non-traditional settings have the potential to provide supplemental HIV screening avenues in an effort to increase early detection. Further research is needed to evaluate the public health benefits and logistical challenges facing the provision of HIV testing in the dental environment. Dental hygienists, with proper training can administer the RHT during routine, comprehensive patient care, and can play a significant public health role in the early diagnosis, treatment, longevity and improved quality of life for people living with HIV infections.
Acknowledgements
The authors would like to thank the management of the three dental hygiene clinics for supporting this research project as well as the senior dental hygiene students and the dental patients who participated in this study.
About the Authors
Susan H. Davide, RDH, MS, MSEd is an associate professor in the department of dental hygiene, New York City College of Technology, Brooklyn, NY; Anthony J. Santella, DrPH, MPH, MCHES, is an associate professor in the department of health professions, public health program, Hofstra University, Hempstead, NY; Winnie Furnari, RDH, MS, FAADH is a clinical professor in the dental hygiene programs, New York University, New York, NY; Petal Leuwaisee, RDH, MA is assistant professor in the department of allied health, dental hygiene program, Hostos Community College, Bronx, NY; Marilyn Cortell, RDH, MS, FAADH is associate professor in the department of dental hygiene, New York City College of Technology, Brooklyn, NY; Bhuma Krishnamachari, PhD, is an associate professor and assistant dean of research, New York Institute of Technology, Old Westbury, NY
Corresponding author Susan H. Davide, RDH, MS, MSEd; sdavide@citytech.cuny.edu
References
1. Monitoring selected national HIV prevention and care objectives by using HIV surveillance data-United States and 6 U.S. dependent areas-2010. HIV surveillance supplemental report [Internet]. Atlanta: Centers for Disease Control and Prevention. 2012 Jun [cited 2017 April 7];17(3, part A). Available from: https://www.cdc.gov/hiv/pdf/statistics_2010_HIV_Surveillance_Report_vol_17_no_3.pdf
2. HIV surveillance report 2014 [Internet]. Atlanta: Center for Disease Control and Prevention. 2015 Nov [cited 2017 Apr 7]; Available from: https://www.cdc.gov/hiv/pdf/library/reports/surveillance/cdc-hiv-surveillance-report-us.pdf
3. Trends in the U.S. HIV diagnoses, 2005-2014 [Internet]. Atlanta: Center for Disease Control and Prevention. 2016 Feb [cited 2017 Apr 7]. Available from: https://www.cdc.gov/nchhstp/newsroom/docs/factsheets/hiv-data-trends-factsheet-508.pdf?s_cid=cs_06
4. Surveillance Annual Report, 2014 [Internet]. New York: New York City Department of Health and Mental Hygiene. 2015 Dec [cited 2017 Apr 7]. Available from: https://www1.nyc.gov/assets/doh/downloads/pdf/dires/2014-hiv-surveillance-annual-report.pdf
5. Sherin K, Klekamp BG, Beal J, Martin N. What is new in HIV infection? Am Fam Physician 2014;89(4): 265-272.
6. Moyer, VA. Screening for HIV: recommendation statement. U.S. Preventive Services Task Force. Ann Intern Med. 2013 Jul 2;159(1): 51-60.
7. Pollack HA, Pereyra M, Parish CL, et al. Dentists' willingness to provide expanded HIV screening in oral health care settings: results from a nationally representative survey. Am J Public Health. 2014 May;104(5):872-80.
8. U.S. Preventive Services Task Force: Grade definitions. [Internet]. Rockville: U.S. Preventive Services; 2016 Jun [cited 2017 Apr 7]; [about 2 screens]. Available from: https://www.uspreventiveservicestaskforce.org/Page/Name/grade-definitions#grade-definitions-afterjuly-2012
9. Wilson E, Tanzosh, T, Malderelli, F. HIV diagnosis and testing: what every healthcare professional can do (and why they should). Oral Diseases. 2013 Jul;19(5): 431-9.
10. Nasseh K, Greenberg B, Vuljicic M, et al. The effect of chairside chronic disease screenings by oral health professionals on health care costs. Am J Public Health. 2014 Apr;104(4):744-50.
11. Siegel K, Abel SN, Pereyra M, et al. Rapid HIV testing in dental practices. Am J Public Health. 2012 Apr;102(4): 625-32.
12. About the Ryan White HIV/AIDS program [Internet]. Bethesda: Health Resources and Services Administration: HIV/AIDS programs. 2016 Oct [cited 2017 Apr 7] Available from: https://hab.hrsa.gov/about-ryan-white-hivaids-program/about-ryan-white-hivaids-program
13. Santella A, Davide S, Furnari W, et al. The role of dental hygienists in conducting rapid HIV testing. J Dent Hyg. 2012 Fall;86 (4):265-71.
14. Santella AJ, Krishnamachari B, Davide SH, et al. Dental hygienists' knowledge of HIV, attitudes toward people with HIV and willingness to conduct rapid HIV testing. Int J Dent Hyg. 2013 Nov;11(4): 287-92.
15. Health, United States, 2015: with special feature on racial and ethnic health disparities [Internet]. Hyattsville: National Center for Health Statistics. 2016 [cited 2017 Apr 7]. 449 p. Available from: https://www.cdc.gov/nchs/data/hus/hus15.pdf#078
16. VanDevanter, N, Combellick J, Hutchinson MK, et al. A qualitative study of patients' attitudes toward HIV testing in the dental setting. Nurs Res Pract [Internet]. 2012 Feb 16 [cited 2017 Apr 7]; 2012:1-6. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3306903/
17. Dietz CA, Ablah E, Reznik D, Robbins DK. Patients' attitudes about rapid oral HIV screening in an urban, free dental clinic. AIDS Patient Care and STDs. 2008 Mar; 22 (3): 205-12.
18. O'Connor AM. Validation of a decisional conflict scale. Med Dec Making. 1995 Jan-Mar;15(1):25-30.
19. O'Connor AM, Stacey D, Rovner D, et al. Decision aids for people facing health treatment or screening decisions. Cochrane Database Syst Rev. 2001;3. [cited 2017 Apr 7]. Available from: https://dx.doi.org/10.1002/14651858.CD001431
20. O'Connor A. Decisional conflict. In: McFarland GK, McFarlane EA, eds. Nursing Diagnosis and Intervention. Toronto, Canada: Mosby; 1997. P 486-96.
21. Légaré F, Kearing S, Clay K, et al. Are you SURE? Assessing patient decisional conflict with a 4-item screening test. Can Fam Physician. 2010 Aug;56:308-14.
22. Ferron Parayre A, Labrecque M, Rousseau M, et al. Validation of SURE, a four-item clinical checklist for detecting decisional conflict in patients. Med Dec Making. 2014 Jan;34(1):54-62.
23. Survey of Americans on HIV/AIDS [Internet]. Menlo Park: Kaiser Family Foundation. 2012 Jul [cited 2017 Apr 7]. Available from: http://kff.org/hivaids/poll-finding/2012-survey-of-americans-on-hivaids/
24. Brown LJ, Lazar V. Dental care utilization: how saturated is the patient market? J Am Dent Assoc. 1999 Apr;130: 573-80.
25. Bednarsh H. Oral health care providers can help in early detection of HIV. Access. 2011;25: 14-9.
26. Chapple I L. Periodontal diagnoses and treatment - where does the future lie? Periodontology 2000. 2009 Jan;51(1):9-24.
27. Rogers TC, Zaninovic P, Urankar YR, et al. An innovative HIV training program for dental students. J Dent Educ. 2011 Nov;75: 1426-33.
28. Zaninovic, P, Natto ZS, Turner RL, et al. An innovative HIV training program for dental hygiene students. J Dent Hyg. 2013 Feb;87: 47-55.
29. National Dental Hygiene Research [Internet]. Chicago: American Dental Hygienists' Association. 2016 May 9 [cited 2017 Apr 7]. 13p. Available from: https://www.adha.org/resources-docs/NDHRA.pdf