You must be signed in to read the rest of this article.
Registration on CDEWorld is free. Sign up today!
Forgot your password? Click Here!
Orthodontics begins with teeth that are in a maintainable condition restoratively and periodontally. The restorative dentist must control these issues before the orthodontist places appliances. The above list includes the shared goals of the team and the duties of the orthodontist. With advances in the understanding of sleep apnea, it may also be appropriate to add airway to this list.2
Dental Esthetics
Most orthodontists have studied dental esthetics relative to tooth positioning. While there are many aspects of ideal dental esthetics,7,8 components that the orthodontist must evaluate and consider include:
- Maxillary dental midline
- Proportions of the anterior teeth (golden proportion)
- Axial alignment
- Contact point location
- Gingival margin and zenith location
The dental midline can be improved within limits by restorative procedures. However, if orthodontic alignment is to be performed, the orthodontist plans treatment to ensure the position and vertical axis of the midline is harmonious with the facial esthetics (Figure 1).
The proportions of the teeth make a significant difference in the balance of the smile. Most restorative dentists are keenly aware of the importance of the golden proportion (Figure 2). When the maxillary lateral incisors are pegged or undersized, the orthodontist should be asked to redistribute the spaces. By positioning teeth properly, the restorative dentist can fabricate restorations to ideal proportions. When anterior teeth are crowded or broken down with loss of space, orthodontic alignment allows the natural proportions to be restored.
All teeth have a characteristic axial alignment that creates esthetic balance. The restorative dentist can alter the appearance of the inclination by reshaping the tooth or with a restoration (Figure 3). However, orthodontic tooth movement can make significant improvements in axial position on a routine basis. The orthodontist should always attempt to set the alignment to the best advantage for the restorative dentist.
While most orthodontists appreciate anterior dental esthetics, some do not consider that the posterior teeth also have a normal alignment angle. The posterior teeth axial line angles appear to converge from the gingival through the occlusal toward a “central fulcrum.7 Alignment of teeth with significant crowding without extractions may cause a flaring of the axial alignment of both anterior and posterior teeth. If orthodontists do not extract teeth or reduce the width of teeth with interproximal reduction when the dental arch perimeter is greater than the skeletal arch perimeter, the teeth will be tipped, creating a “flared” appearance. Tipped teeth are not only esthetically unappealing, they are not centered in bone and do not allow occlusal forces to be directed down the long axis of the root, which impairs long-term stability (Figure 4). If treatment goals cannot be reached without extractions, then extractions must be considered.
The location of contact points is often altered by the restorative dentist; when orthodontics is required, the contact point location can be enhanced by tooth movement. The position of the contact point can be improved by changing the axial alignment of the tooth. In cases with dark triangles, the contact points can be lengthened by interproximal reduction, followed by space closure.
Gingival heights and zeniths are important for establishing balance in dental esthetics. In the esthetic dentition, the gingival height of the lateral incisor should range between even with a line between the central incisor and canine to as much as 1.5 mm incisal to that line. The relative size of the lateral should be a guide as to where it should be positioned. The zenith of the gingival margin for maxillary central incisors and canines should be just distal to the tooth midline, while the zenith of the maxillary lateral incisor is at the midline (Figure 5).7,8 While the restorative dentist or periodontist can modify these components of gingival balance, the orthodontist should routinely ensure that these objectives are in place.
Color, shape, morphology, and texture of the teeth are all controlled by the restorative dentist and laboratory technician.9 However, in order to maximize results, all team members should be aware of each other’s abilities and limitations.
Facial Esthetics
All orthodontists can identify smile esthetics—the incisal edges should follow the lower lip contour (Figure 6). Orthodontists also understand the importance of tooth exposure with the lips at rest and on smiling. Yet many may not have considered how the jaws relate to the face. When a patient presents with a malocclusion caused by a skeletal discrepancy, orthodontists are quick to recognize the problem and inform the patient about the treatment options to correct the malocclusion. However, at times, orthodontists overlook how this discrepancy impacts facial esthetics. A retrognathic mandible may be corrected with a mandibular advancement surgery. However, closer examination of the face will often reveal a deficient maxilla associated with the retrognathic mandible. Learning to look at the face, as well as the teeth, allows orthodontists to be more objective. Many patients complain only about the teeth (possibly because this is what orthodontists treat). For example, a patient with a recessive mandible may complain about having “bucky” top front teeth. Some individuals have skeletal imbalances that do not affect the functionality of teeth, such as an occlusal cant, while other skeletal issues compromise orthodontic results without orthognathic–surgical treatment. While not all patients will be concerned with facial esthetics, many would appreciate knowing the options. Extraction of two maxillary premolars may be a reasonable compromise for a patient with a recessive mandible in order to improve function if esthetics is not a concern.
Facial evaluation involves the patient history and motivation, clinical examination, and records.2 The patient history includes questions regarding past orthodontic therapy, extractions, medical conditions, allergies, habits, any symptoms, and TMJ screening. The clinical examination should include an evaluation of the facial profile and frontal views. However, these evaluations are subjective. Records allow a more objective evaluation of the face. They include: facial pictures taken in natural head posture, intraoral pictures, lateral cephalometric radiographs, panoramic radiographs and bite wings, an accurate bite registration, and mounted models.2 Arnett developed the “soft tissue cephalometric analysis” to add objectivity to the clinical assessment. The analysis establishes norms and standard deviations for:
- Dental and skeletal factors
- Soft-tissue components
- Vertical facial lengths
- True vertical line projections
- Facial harmony10
This analysis emphasizes the importance of evaluating soft tissue in addition to hard bony cephalometric landmarks when assessing facial balance and proportions.
Periodontal Health
A stable periodontal environment is crucial to creating a stable result. Goals for the orthodontist should be as follows:
1. Ensure adequate attachment of keratinized gingiva before moving teeth. Orthodontic movement in the presence of inadequate attachment may accelerate recession.
2. Position teeth in the center of the bone. When teeth are moved through cortical bone, fenestrations and gingival recession may be an unintended consequence. Today, some orthodontists claim to have “nonextraction” practices. While most patients may be able to have teeth aligned without extractions, a significant number of the outcomes will result in teeth positioned out of the bone. The issue is not Can I treat without extractions; but Can I reach my goals without extractions; if I cannot achieve my goals, then extractions must considered. This is an important issue in orthodontics.
3. Position teeth to have forces directed appropriately without interferences to closure or excursions.1,5 While most clinicians agree that periodontal pockets do not form without bacterial inflammation, occlusal trauma in the presence of gingival disease accelerates attachment loss.1 Therefore, functional occlusal goals are important to periodontal health.
4. When possible, position teeth to level interproximal bone heights. When moderate bony pockets have developed, orthodontics may be attempted, understanding that restorative procedures will be required after orthodontics is completed.
5. Create an easily maintainable environment. Proper interproximal contacts, relief of crowding, appropriate axial positioning of the teeth, and correction of vertical boney defects all serve to improve the maintainability of the dentition.
TMJ Health
Perhaps the most debated topic in orthodontics is the relationship of the occlusion to the TMJ. Many orthodontic programs do not train the residents to understand components of an ideal occlusion and its relationship to a healthy joint. The National Institute of Dental and Craniofacial Research and the National Institutes of Health not found a relationship between the occlusion and TMDs.11 Part of the problem is that TMD “is an all inclusive term that includes many type of disorders, any one of which may be multifactorial.1 Additionally, there is a lack of sound evidence based on research. While head and neck pains are not all related to the occlusion, some TMDs are occlusally related and will respond to appropriate and meticulous occlusal treatment.1,12 The key is to understand how to differentiate and treat these cases.1-3,10,12-14 Given that few orthodontic programs emphasize the role of the joints in healthy function, some orthodontists may not have the background to meet the expectations of the restorative dentist.
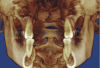
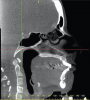
A stable TMJ is critical in establishing a normal functional occlusion. Unless the condyles are in a stable musculoskeletal position, there are always interferences to normal function and stress placed on the masticatory system.1-3,15 In orthodontics, the Angle classification of malocclusion using handheld models has been the standard to evaluate the fit of the teeth. However, it is not possible to truly identify the occlusion/malocclusion using handheld models. Before the occlusion can be evaluated, the clinician must ascertain the joint position and condition (Figure 7 and Figure 8).1,16
Optimum Functional Occlusion
From an orthodontic perspective, Andrews was the first to describe the static features of the ideal occlusion in the “Six Keys to Optimal Occlusion.17 He studied models of untreated cases with optimal unworn occlusions and described the attributes of the occlusion regarding tip, axial inclination, rotation, the curve of Spee, contacts, and the position of teeth relative to each other.
Roth added the importance of a seated condylar position to Andrews’ findings to establish a model of function for the orthodontist.13 Roth is considered to be the most outspoken proponent for the importance of a seated condylar position in orthodontics. The principles he learned from many of the pioneers in gnathology were missing in orthodontic study.15 He realized that these basics should be just as important to the orthodontist as they are to the restorative dentist. Yet his views were not well received by many in the orthodontic academic community. One well-known department chairperson has said that “gnathology is the science of how articulators chew.18 Many dentists express surprise that some orthodontists believe a seated condylar position is unnecessary and unimportant.19,20
Many of the most respected dentists in the world have described the importance of the joints in establishing a functional occlusion. Dawson, Lee, Okeson, and others have described the features of a functional occlusion.1,3,14 Roth attempted to bring the orthodontist into the same arena. His criteria for a functional occlusion are as follows:
1. Teeth in maximum intercuspation with the mandible in centric relation.
2. On closure into occlusion, the stress on the posterior teeth should be directed down the long axis of the posterior teeth so that the resultant stresses will be transmitted as tension to the periodontal ligament and lamina dura.
3. Posterior teeth should contact evenly and equally on closure into occlusion with light anterior contact when the joints are seated so as to protect the anterior teeth from lateral stress.
4. Adequate overbite and overjet to immediately disengage the posterior teeth in any excursive movement to protect the posterior teeth form lateral stresses. This anterior relationship should work in harmony with the movement pattern dictated by the TMJs so as to not produce lateral stresses on the anterior teeth.
5. Cusp height, fossa depth, ridge and groove direction, and cusp placement should be in harmony with the mandibular movements in all directions (border movements) to provide minimal interference of the teeth with the movement pattern of the mandible dictated by the TMJ.15
Stability
Traditional orthodontic research into stability has been directed at measuring how much unstable orthodontic cases have relapsed. Researchers have studied these failed cases and then drawn “conclusions that the answer to stability is to emulate what failed cases show us regarding arch form.5 Roth proposed that orthodontists should be examining the “common attributes” of cases that have “remained stable with healthy joints, healthy periodontium and no occlusal wear and attempting to emulate those attributes.5 Key features of stability included parallel roots, the occlusion allowing the joints to seat in centric relation, a mutually protected occlusion, and equal and even contact of centric cusps with forces directed down the long axis of the teeth.1,5
Satisfaction of Patient’s Chief Complaint
No treatment is adequate if orthodontists do not address the patient’s chief complaint. The team should note this at treatment initiation. By ensuring that the patient’s desires are understood at the beginning, the team is able to plan treatment to verify that those wishes are achievable. If unrealistic expectations are discovered, the team must ascertain that the patient is educated about the possibilities and limitations before any treatment starts.
Airway Assessment
In recent years, the medical community has better understood the prevalence of sleep apnea. The mean age for sleep apnea is 45 years.21 Severe apnea is considered to be more than 30 episodes of interrupted breathing per hour. Left untreated, apnea has been associated with high blood pressure, vascular disease, and stroke.22 Dentists are in an ideal position to screen and direct patients for appropriate evaluation. By adding the Epworth Sleepiness Survey21 to the medical history questionnaire, dentists can make a significant contribution to enhancing quality of life and helping reduce mortality rates. One of the most predictable long-term treatments for severe apnea involves surgical anterior positioning of the jaws to open the airway.23,24 Therefore, the interdisciplinary team is in an ideal position to diagnose and, in some cases, treat this malady. Consequently, it is prudent to include airway in the list of goals.2
Conclusion
Orthodontics is an important element of the interdisciplinary team’s approach to complete dentistry. Some orthodontic treatment has been criticized for not positioning teeth appropriately to allow the rest of the team to complete the rehabilitation properly. In many cases, the problem is related to the fact that some orthodontic training programs do not adequately emphasize objective treatment goals (Figure 9).
With handheld models, orthodontists cannot make accurate assessments concerning function. Therefore, objective evaluation of the dental relationship is not possible.
The debate about extractions is another important orthodontic issue. Extraction or nonextraction therapy is a treatment plan, not a philosophy. Yet, this has been debated for almost 100 years. The pendulum swings back and forth because of a lack of objective goals. The issue is not should we have extractions; rather, who should have extractions. Removal of teeth in the appropriate patient allows the goals to be met and does not cause a decline in facial esthetics.
The application of objective measurable goals that have been proven in the literature to provide long-term comfort, function, health, and esthetics can help the orthodontist provide an important and predictable service. This helps the interdisciplinary team achieve a more ideal result. Once the orthodontist understands the goals and their measurements, the team must develop a communication process that allows appropriate delineation of duties and sequencing of treatment for efficient flow.
This can facilitate better understanding and communication among team members. Shared goals help determine when extractions, periodontal surgery, orthognathic surgery, or other treatments should be considered to achieve the most ideal result for patients.
References
1. Dawson PE. Functional harmony. In: Dawson PE. Functional Occlusion: From TMJ to Smile Design. St. Louis, MO: Mosby; 2007:1-256.
2. Arnett GW, McLaughin RP. Facial and Dental Planning for Orthodontists and Oral Surgeons. St. Louis, MO: Mosby; 2004:4-11.
3. Lee R. Esthetics and its relationship to function. In: Rufenacht CR, ed. Fundamentals of Esthetics. Chicago, Ill: Quintessence; 1990:137-209.
4. Roth RH. Gnathologic concepts and orthodontic treatment goals. In: Jarabak JR, ed. Technique and Treatment with Light Wire Appliances. St. Louis, MO: Mosby; 1970:1160-1223.
5. Roth RH. The Roth functional occlusion approach to orthodontics. Notes from lecture introducing the functional occlusion section of the Roth/Williams Center for Functional Occlusion 2 year program.
6. Roblee RD. Interdisciplinary dentofacial therapy (IDT). In: Roblee RD, ed. Interdisciplinary Dentofacial Therapy. Chicago, Ill: Quintessence; 1994:17-44.
7. Rufenacht CR. Structural esthetic rules. In: Rufenacht CR ed. Fundamentals of Esthetics. Chicago, Ill: Quintessence; 1990:67-134.
8. Cliche GJ. Proportion, display, and length for successful esthetic planning. In: Cohen M, ed. Interdisciplinary Treatment Planning: Principles, Design, Implementation. Chicago, Ill: Quintessence; 2008:1-48.
9. Rufenchacht CR. Esthetic management of the dentofacial unit. In: Rufenacht CR, ed. Fundamentals of Esthetics. Chicago, Ill: Quintessence; 1990:225-234.
10. Arnett GW, McLaughlin RP. Diagnosing the case. In: Arnett GW, McLaughin RP, eds. Facial and Dental Planning for Orthodontists and Oral Surgeons. St. Louis, MO: Mosby; 2004:135-196.
11. TMJ disorders. National Institute of Dental and Craniofacial Research Web site. http://www.nidcr.nih.gov/OralHealth/Topics/TMJ/TMJDisorders.htm. Accessed July 7, 2010.
12. Okesson JP. General considerations in occlusal therapy. In: Okesson JP, ed. Management of Temporomandibular Disorders and Occlusion. 5th ed. St. Louis, MO: Mosby; 2003:553-566.
13. Roth RH. Functional occlusion for the orthodontist. J Clin Orthod. 1981;15(1):64-81.
14. Okeson JP. Criteria for optimal functional occlusion. In: Okeson JP, ed. Management of Temporomandibular Disorders and Occlusion. 5th ed. St. Louis, MO: Mosby; 2003:109-126.
15. Roth RH. The maintenance system and occlusal dynamics. Dent Clinics North Am. 1976;20(4):761-788.
16. Cordray FE. Three-dimensional analysis of models articulated in the seated condylar position from a deprogrammed asymptomatic population: a prospective study. Part 1. Am J Orthod Dentofacial Orthop. 2006;129(5):619-630.
17. Andrews LF. The six keys to optimal occlusion. In: Andrews LF, ed. Straight Wire: The Concept and Application. 1st ed. La Jolla, Calif: LA Wells; 1989:13-24.
18. Rinchuse DJ, Kandasamy S, Rinchuse D. Articulators in orthodontics: Part 2 (word of mouth). Orthodontic Products Online. 2007:6.
19. Rinchuse DJ, Rinchuse DJ. Orthodontics justified as a profession. Am J Orthod Dentofacial Orthop. 2002:121(1):93-96.
20. Rinchuse DJ, Kandasamy S. Articulators in orthodontics: an evidence-based perspective. Am J Orthod Dentofacial Orthop. 2006;129(2):299-308.
21. Johns MW. A new method for measuring daytime sleepiness: the Epworth sleepiness scale. Sleep. 1991;14(6):540-545.
22. Mayo Clinic Staff. Sleep apnea: complications. http://www.mayoclinic.com/health/sleep-apnea/DS00148/DSECTION=complications. Accessed August 26, 2010.
23. Prinsell JR. Maxillomandibular advancement surgery for sleep apnea syndrome. J Am Dent Assoc. 2002;133(11):1489-1497.
24. Riley RW, Powell NB, Guilleminault C. Obstructive sleep apnea syndrome: a surgical protocol for dynamic upper airway reconstruction. J Oral Maxillofac Surg. 1993;51(7):742-747: discussion 748-749.
About the Author
Carl P. Roy, DDS, MS
Private Practice
Virginia Beach, Virginia