You must be signed in to read the rest of this article.
Registration on CDEWorld is free. Sign up today!
Forgot your password? Click Here!
For both consumers and clinicians, it is important to be aware of the dental product and technology landscape so that patient care can benefit from the most well-suited materials. Assessment must depend on a product's estimated clinical and financial advantages. In years past, caries detection was accomplished through visual examination, film x-rays, and the use of explorers. Now, though clinicians still utilize these methods, new technologies have enhanced and largely replaced them. Advanced tools can be used to improve presentation so that patients better understand their necessary treatment. Technology innovations are being used concurrently with traditional x-rays or replacing them entirely, depending on the needs of the case. This article presents a review of modernized caries detection technologies, including their advantages and disadvantages.
Caries Detection Technology: Then and Now
Visual examinations have improved over time, as dentists have been able to visualize better through magnification loupes and microscopes, as well as intraoral lighting and cameras that offer additional light sources and magnification. Moreover, patients, too, are able to see images of their intraoral condition. Many improvements also have occurred in radiography. Film has become far more sensitive, which means less radiation for the patient while better retaining image quality. Digital intraoral radiography also offers reduced radiation exposure1 and helps improve diagnosis due to image quality improvements. Digital x-rays provide a large-screen image, while dental practices benefit from not having to use or dispose of any chemicals, and there is no processor to maintain. Additionally, images are conveniently saved within program software, which eliminates the time that would otherwise be spent developing, processing, and mounting x-rays.
Perhaps the most significant advantage of modern advancements in caries detection is how helpful they are for patient education. Dentists are able to present their findings on a monitor that the patient can view. Digital extraoral radiography, which is a panoramic with all the benefits of intraoral radiography, is also available to the clinician. Three-dimensional (3D) cone-beam computed tomography (CBCT), in particular, uses a cone-beam with 3D views that can yield vast amounts of anatomical data.
Despite the litany of benefits, there are limitations to radiography. While x-rays still play a large role in diagnosis for many different types of disease, their use in caries detection is limited. Decay can be difficult to detect in radiographs unless it is larger than 2 mm to 3 mm deep into the dentin or one-third the buccolingual distance.2 Fortunately, technology provides clinicians options for overcoming these limitations.
Some controversy exists over the use of explorers for caries detection. According to G.V. Black's state-of-the-art occlusal caries detection methods published nearly a century ago in 1924, a sharp explorer should be used with some pressure and if a very slight pull is required to remove it, the pit should be marked for restoration even if there are no signs of decay.3 About 70 years later in 1991, research was published claiming there was no difference in diagnostic accuracy between an explorer and a visual technique only.4 In 2005, questions arose about the use of explorers on the basis of purported inaccuracy of their contribution to caries diagnosis, as some researchers believed it may have been possible to spread infective plaque from other teeth in the mouth or cause damage to pits and fissures, though evidence from long-term clinical trials was lacking.5
Fast forward to present day and caries detectors are now available with image tool software that demonstrate a higher intra- and inter-examiner reliability than the explorer method in estimating areas of enamel demineralization lesions.6 Overall, caries detection has advanced rapidly in recent decades, which naturally leads to the question: How can clinicians leverage new technology in the modern dental practice?
Modernized Examination Practices and Systems
Modernized examination technology begins with a traditional teeth cleaning. The clinician performs a prophylaxis, ideally using a system that combines an ultrasonic scaling unit and non-abrasive sodium bicarbonate and water-pressure air polishing system. Unlike rubber cups, which cannot penetrate into deep grooves or pits, these air polishing systems clean them out very efficiently.7 This also allows the clinician to later use a caries detection system (eg, DIAGNOdent™ Pen, KaVo Kerr, kavo.com; CariVu™, Dexis, dexis.com; CamX® Spectra, Air Techniques, airtechniques.com) without obtaining false readings. Assistants then take the necessary x-rays with a digital system (eg, DEXIS Platinum, DEXIS; Schick 33 Sensor, Dentsply Sirona, dentsplysirona.com; GXS-700, Gendex, gendex.com). Next, cancer screening can be performed by palpating oral tissues and moving the tongue aside to check for lesions.
The clinician proceeds to use an explorer, because though it is not the primary tool for decay detection, patients tend to expect it, and it can help in examining teeth for such issues as surface irregularities, calculus, resorption, and even pulp exposure. After this, a caries detection system can be used for screening. The clinician reviews the images and findings with the patient by using an intraoral camera. The value of this method is that it helps educate patients regarding their intraoral condition, which typically leads to greater understanding and perhaps treatment acceptance. Overall, multiple technologies can be used in concert, enabling dentists to employ highly comprehensive diagnostics and presentation for, ultimately, excellent patient care.
Introduced in the late 1990s, early electronic caries detectors used fluorescence, with some later models specifically utilizing quantitative light-induced fluorescence.8 Over time, caries detectors have become more accurate, sophisticated, portable, and easy to use. Some have even begun to integrate with imaging software. Caries detectors quantify demineralization detection results and create a visible or audible indication that caries has been found. This helps improve the patient experience as they can clearly see that the condition exists.
A shortcoming of early fluorescence systems is that the tooth must be clean and free of all bacteria, which is why an air polishing prophy system should be used beforehand. Neglecting to prepare the tooth with an air polish and the resultant presence of prophy paste could lead to false readings.9 Other disadvantages are that the system may only function for occlusal and smooth surfaces and not around restorations or interproximally. Additionally, typically with fluorescence systems there is no image to view, or the image created may need to be imported into imaging software.
Other systems, the CariVu for example, use near-infrared transillumination for caries detection. This type of system builds upon older digital imaging fiber-optic transillumination (DIFOTI) technology through the addition of a dual near-infrared light in the intraoral camera and image capture. A benefit to this technology is that it detects not only occlusal but also interproximal and recurrent caries and fractures. Detection is not affected by the presence of bacteria and it is 99% accurate for interproximal caries.10 In some cases, the detection system can serve as a substitute for bitewing x-rays.11 It can capture an image that shows the exact size and location of the caries, which helps ensure that preparations are as conservative as possible, and leaves no metrics to interpretation. Additionally, the clinician can share the images with patients and save them in their record.
A disadvantage of this near-infrared transillumination technology is that it detects only up to 10 mm away from the light source, making it less than ideal for use on patients, particularly geriatric patients, with interproximal root caries that is considerably past the contact areas. It also does not quantify the depth of occlusal caries. According to the manufacturer, the CariVu unit functions by utilizing flexible arms that travel the tooth and near-infrared photons emitted through the arms. These photons travel from the root to the crown of the tooth. Dense enamel reflects the photons while porous lesions trap and absorb them. As a result, healthy tooth appears light and lesions appear dark, providing a structural view of the lesion whether it is interproximal, occlusal, or around a restoration. Emitting no radiation, the unit produces images in black and white. The unit's wand is placed over the patient's teeth with a soft rubber saddle, allowing the patient to see what x-rays may miss. Patients can watch live video as it is being captured by the detection system. The purpose it to diagnose issues as early as possible.
Case Studies of Caries Detection Technology
A laser fluorescence detector, such as the DIAGNOdent, is useful when the clinician is uncertain whether there is or isn't a lesion. Stain is largely suitable as an indicator. Transillumination is another method that the author uses most often, and its use will be shown in the following cases.
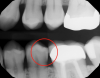
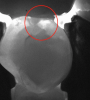
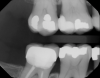
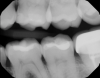
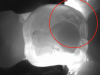
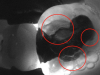
Figure 1 shows a pretreatment photograph of a tooth No. 20. In Figure 2, the circled area of the x-ray indicates the interproximal area where the clinician was uncertain if caries was present. Though x-rays are useful, transillumination is more sensitive and optimal for detecting caries in the early stages.12 With new devices, clinicians can acquire more information before working on the tooth. As shown in Figure 3, caries was confirmed using the transillumination system (CariVu), though it did not show up on an x-ray. The clinician was able to show the image to the patient. The open-tooth camera image then revealed the extent of the caries in the exact position that was displayed in the transillumination image (Figure 4). This is a significant advantage in minimizing preparations and saving valuable tooth structure.
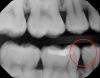
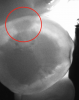
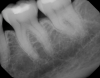
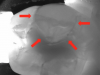
Figure 5 and Figure 6 show possible insipient legions. The clinician would need to decide whether to just flag the tooth or restore it. Nothing problematic is evident in the intraoral photograph of the tooth. The transillumination system, however, revealed a lesion at the dentinoenamel junction (DEJ) (Figure 7), and the open-tooth camera image clearly showed the decay present (Figure 8). This speaks to the notion that you cannot treat what you cannot see.
In Figure 9, transillumination images are shown from a case of a 3-year-old patient. Because taking x-rays on a very young child can be like trying to hit a moving target, the clinician used the CariVu. The caries detector revealed no decay, which was satisfactory. By opting to use the caries detection unit instead of trying to take x-rays, the clinician avoided irradiating the child while still employing an effective tool. Not having to irradiate a patient can also serve as a marketing instrument, as parents typically are pleased that their dentist offers non-radiation diagnostics. This, in turn, can function as a practice builder when these parents tell their friends.
In another case of a caries-prone 6-year-old patient, the clinician, who generally avoids taking x-rays on children, opted to take them this time because lesions can grow rapidly.13 The transillumination caries detector also was used to attain a more complete diagnosis and to find problems as early as possible. Decay appeared on both the x-ray (Figure 10) and the CariVu image (Figure 11). Viewing the situation from multiple perspectives enables treatment to be as conservative as possible because the clinician can pinpoint exactly where the decay is present on the tooth.
In yet another case, a comparison of an x-ray and a transillumination image is presented in Figure 12 and Figure 13. Though nothing was visible on the x-ray, the transillumination image showed a total fracture through the buccal cusp on tooth No. 19 that would require a crown. An added benefit is that the transillumination image can be used for the insurance predetermination. Figure 14 and Figure 15 depict a case of a lingual fracture on tooth No. 3 where nothing problematic showed up on the x-ray. However, the transillumination image showed the facture as well as caries distal to the fracture (Figure 16). There was also recurrent decay adjacent to the restoration. The image made the problem obvious to both the clinician and the patient, which led to the patient accepting treatment.
Upon initial examination, Figure 17 and Figure 18 reveal a large restoration and potential problem on distal of tooth No. 18, though the clinician was uncertain about it. Once the CariVu was utilized, the clinician saw a fracture and complete degeneration of the distal buccal cusp (Figure 19), which fell apart when preparation began due to the severity of the fracture.
Lastly, Figure 20 and Figure 21 show a case where it was unclear whether the situation was a failing restoration or caries on tooth No. 15. After viewing the transillumination images the clinician found recurrent caries in three places at the margins of the restoration (Figure 22). Because of the size of the restoration and the extent of recurrent caries, tooth No. 15 needed a crown. The patient accepted treatment having seen the oral condition.
Similar to its effectiveness for use on young children on whom taking x-rays can be challenging due to their figitiness, the transillumination caries detection system is also applicable to cases in which the patient requires a special-needs dentist. For example, the author has used the system when examining an 18-year-old patient with cerebral palsy who would normally jerk his head, which would make taking x-rays difficult. In the author's experience, images can be acquired and caries diagnosed in about 20 seconds.
Insurance Considerations of Caries Detection Procedures
Finally, it is valuable to understand the new ADA CDT code for caries detection procedures. According to the Code Maintenance Committee of the American Dental Association, it recently approved an insurance code specifically for a nonionizing diagnostic procedure capable of quantifying, monitoring, and recording changes in structure of the enamel, dentin, and cementum. The new CDT code D0600 took effect January 1, 2017. Unlike with x-rays, the clinician files for the service rendered rather than for the images. Reimbursements for filing of caries detection screening may take time, as carriers need to educate themselves on the need for the procedure. A narrative may also need to be included when filing so that insurance carriers can become familiar with the code.
Conclusion
Technology is changing the way caries detection can be carried out. By understanding the history and development of caries detection and the rationale behind certain modern technologies, clinicians can accurately assess current caries detection instruments that can be used to replace or complement traditional x-ray imaging. These systems can be especially helpful for cases in which the patient is young or otherwise moves around a lot. To successfully implement these products into their dental practice, the clinician must assess the technology's value on a case-by-case basis and become familiar with current changes to insurance reimbursement.
References
1. American Dental Association Council on Scientific Affairs. Dental Radiographic Examinations: Recommendations For Patient Selection And Limiting Radiation Exposure. Chicago, IL: US Dept of Health and Human Services; Revised 2012.
2. Rock WP, Kidd EA. The electronic detection of demineralisation in occlusal fissures. Br Dent J. 1988;164(8):243-247.
3. Black GV. Operative Dentistry. 1924;1(7):32.
4. Lussi A. Validity of diagnostic and treatment decisions of fissure caries. Caries Res. 1991;25(4):296-303.
5.Hamilton JC. Should a dental explorer be used to probe suspected carious lesions? Yes—an explorer is a time-tested tool for caries detection. J Am Dent Assoc. 2005;136(11):1526-1530.
6. Nassur C, Pomarico L, Maia LC. Reliability analysis of two methods for measuring active enamel demineralization: An in vitro study. Eur J Dent. 2013;7(2):159-164.
7.Botti RH, Bossù M, Zallocco N, Vestri A, Polimeni A. Effectiveness of plaque indicators and air polishing for the sealing of pits and fissures. Eur J Paediatr Dent. 2010;11(1):15–18.
8. Stookey GK. The evolution of caries detection. Dimensions of Dental Hygiene. 2003;1(6)12-15.
9. Gutkowski S. Minimal intervention: polishing enamel. RDH website. August 1, 2008. http://www.rdhmag.com/articles/print/volume-28/issue-8/feature/minimal-intervention.html. Accessed November 15, 2017.
10. Kühnisch J. Benefits of the DIAGNOcam Procedure for the Detection and Diagnosis of Caries [study project]. Munich: Ludwig Maximilian University of Munich; 2013.
11. Söchtig F, Hickel R, Kühnisch J. Caries detection and diagnostics with near-infrared light transillumination: clinical experiences. Quintessence Int. 2014;45(6):531-538.
12.Peers A, Hill FJ, Mitropoulos CM, Holloway PJ. Validity and reproducibility of clinical examination, fibre-optic transillumination, and bite-wing radiology for the diagnosis of small approximal carious lesions: an in vitro study. Caries Res. 2993;27:307-311.
13. Colak H, Dülgergil CT, Dalli M, Hamidi MM. Early childhood caries update: a review of causes, diagnoses, and treatments. J Nat Sci Biol Med. 2013;4(1):29-38.