You must be signed in to read the rest of this article.
Registration on CDEWorld is free. Sign up today!
Forgot your password? Click Here!
Instruments used today to perform dental surgical techniques have evolved over hundreds of years, starting with the scalpel in the 1800s, electrosurgery in the 1920s, and various types of lasers over the course of the past 25 years. Besides the scalpel, today’s primary forms of instrumentation include electrosurgery, diode lasers, carbon dioxide (CO2) lasers, and erbium lasers (Table 1). No one instrument is capable of fulfilling all the needs of dentists and patients for the entire range of surgical procedures. In fact, the optimal surgical instrument would have to comply with patient demand for comfortable procedures with esthetically appealing results and with the dental practitioner’s need for efficiency with predictable outcomes.
Surgical Technique Challenges
Dental practitioners face a number of challenges when using surgical equipment. One such challenge is maintaining a clean operating field with consistent visibility. Bleeding during the use of a scalpel or other instruments obstructs the user’s field of vision and can slow down or halt the procedure until appropriate measures are taken to stop the bleeding. Another challenge with laser instruments can be achieving smooth, snagless cutting with tactile feedback. While a scalpel is usually easy to guide along a planned trajectory, some instruments, especially diode lasers, are known for stalling and dragging during the cutting process. The laser fiber may intermittently lose its ability to cut and can catch on tissue. To remedy this, the fiber must be frequently reinitiated in order to cut. If not immediately noticed, stalling and dragging may result in unnecessary collateral thermal damage because the time on tissue is extended. Some laser devices, such as the CO2 or erbium lasers, work in a non-contact mode and have no tactile feedback, which precludes the dentist from being able to “feel” the tissue while cutting—a major drawback to the use of these lasers for soft-tissue surgery.
Controlling thermal collateral damage is another challenge for dentists. All surgical instruments with a thermal component—especially electrosurgery instruments—can tend to cause thermal damage during cutting. This is a function of the heat created and the speed at which the cutting instrument glides over tissue. Classic electrosurgery systems are known for extensive collateral thermal tissue damage,2 and they may also damage tissue and bone around implants if touched. Diode lasers can also produce thermal tissue damage that may potentially be extensive depending on cutting speed. Both of these modalities are technique-sensitive, lending themselves to insufficient control over thermal collateral damage.
Reducing the time spent on tissue is another issue. For standard diode lasers with fixed power, collateral tissue damage greatly depends on the speed of cutting. With low speed caused by a snag or drag, the extent of collateral damage can exceed 1 mm. Hemostasis requires no more than 200 µm to 500 µm; therefore, 1 mm or more of tissue coagulation corresponds to a significant over-treatment. Extensive thermal tissue damage has multiple implications in the success of a procedure, the postoperative phase, and the esthetic outcome. Results may be similar to a third-degree skin burn—ie, extensive tissue necrosis, long healing times, scar tissue formation, and uncontrollable tissue recession.
Clinicians must also be cognizant of protecting sensitive structures from overheating. Removing soft tissue on or around structures—such as natural teeth, teeth with dental crowns, or dental implants—is a concern when using diodes and other lasers in the 800 nm to 1,100 nm range. This laser radiation can penetrate deep into tissues and heat up highly absorbent dental materials or dental implants that conduct heat to the surrounding soft tissue and bone. Extensive collateral thermal damage to these structures is possible. Monopolar electrosurgery is not recommended around metal objects, such as teeth with dental crowns or dental implants.
Another issue is maintaining hemostasis and wound sealing. Non-thermal cutting techniques like the scalpel require chemical and mechanical methods to stop bleeding and seal blood vessels. The resulting open wounds may also require some kind of wound closure, such as sutures, to enhance the healing process and avoid infection. Thermally oriented surgical instruments, such as electrosurgery, diode lasers, and CO2 lasers, cauterize as they cut to a depth of more than 200 µm, so blood and lymphatic vessels are sealed and wounds are protected from infection. An exception is the erbium cut, which does not provide sufficient cauterization (< 50 µm) for many blood vessels and, therefore, requires additional methods of hemostasis.
Finally, clinicians must also be careful to avoid technique-related operative and postoperative discomfort. Different surgical techniques and procedures have varied requirements for pain control. Electrosurgery is perhaps the most pain-inducing technique due to the sometimes extensive burning of tissue, and the postoperative phase might be longer with considerable discomfort because of the excessive tissue damage.
Issues Regarding Non-Contact Vs. Contact Cutting
While most surgical instruments contact the tissue to be cut, some laser systems require that a certain distance from the surgical site be maintained. The most prominent non-contact laser devices are CO2 lasers and erbium lasers. Both of these laser systems have good absorption in soft tissue (about 630 cm-1 for CO2 and 10,000 cm-1 for erbium), ie, the laser light interacts directly with oral tissues to create the cutting effect. The direct laser light absorption by oral soft tissues also means that laser energy remains localized and focused, leading to lower heat generation in surrounding tissues and virtually no penetration of laser light into deeper tissue layers. The cuts obtained with these lasers are clean and, depending on the mode used, exhibit a small coagulation zone around the cut, with a depth ranging from 5 µm to 500 µm. However, because the specific laser wavelengths travel through standard quartz glass fibers, both CO2 and erbium lasers require complicated light transport systems and optical handpieces with specific focal points in order to work in a clinical environment. The handpiece must be held at a certain distance to achieve a good focal point that cuts tissue, similar to using a magnifying glass to focus sunlight. This is counterintuitive to many dentists. Also, the absence of tactile feedback means that observation alone defines the field of operation, cutting depth, and width, which may require a steep learning curve for the clinician.
Except for the scalpel, most soft-tissue contact-cutting technologies use some form of heat to produce a cut. The electrosurgery device uses an electrical current to create heat and perform a cut; other variants of the electrosurgical device use radio waves to create heat. Scalpel and electrosurgery are described in Table 1.
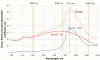
Another and very popular device for contact surgery is the near-infrared diode laser. Near-infrared lasers, such as diode or Nd:YAG lasers, have wavelengths ranging from 800 nm to 1,100 nm and use quartz fibers to transport laser light from the laser source to the target tissue. The fiber walls have a reflective cladding that keeps the laser light inside the fiber; the laser light bounces back and forth from wall to wall, and finally exits at the distal end, or the fiber tip. If the fiber tip has a clean fresh cleave, the laser light will exit freely and penetrate into the tissue below. When tissue effectively absorbs the laser light—as with CO2 and erbium lasers—most of the light is absorbed in the top tissue layer, leading to a rupture of the tissue, ie, cutting. For near-infrared lasers, light tissue interaction is completely different. Figure 1 shows the absorption spectra for two major tissue chromophores in the near-infrared range, with water and blood calculated based on experimental data.3-5 For soft tissue, such as the reticular layer of mucosa with 70% water and 5% blood, total absorption coefficient is as low as 0.2 cm-1 to 0.65 cm-1. In the 800 nm to 940 nm range, the dominating absorption occurs in blood, and for the 970 nm to 1,100 nm range, the absorption in water and blood are comparable. Because the tissue is a poor absorber of the near-infrared laser light—for example, oral soft tissue for a diode or Nd:YAG laser—the light will then penetrate into deeper layers of the tissue.6 This may lead to heat build-up in larger tissue areas and damage sensitive structures beneath the soft-tissue layer being irradiated.
Diode Laser Limitations
Diode lasers have poor absorption in dental soft tissue and would be extremely ineffective cutting instruments if they relied solely on the absorption of laser radiation to cut tissue. Power density needed for direct tissue cutting using light is inversely proportional to the absorption coefficient. Because of the very low tissue-absorption coefficient (Figure 1), a very high power is needed for direct tissue cutting with light. Minimum average power for direct tissue cutting with a 400 μm tip is about 25 W, which is much higher than the typical power of commercially available diode dental lasers (which are typically in the range of 2 W to 7 W).
Another issue is that diodes cut with heat, not light. Diode lasers exhibit a phenomenon called the “hot-tip effect.” When the tip of an uninitiated laser fiber touches soft tissue and the laser is activated, the laser energy penetrates into the tissue. At the point of contact of the distal end of the fiber with the tissue surface, protein is slowly denatured, becomes carbonized, and turns black.7,8 This black denatured protein then clings to the tip and heavily absorbs laser energy, thus heating the tip to several hundred degrees. When this hot tip touches soft tissue, the heat causes thermo-mechanical tissue cutting and coagulation. The cutting effect is not constant, however, because the black deposit on the fiber is continuously scraped away as the fiber passes over tissue, leading to fluctuations in cutting and coagulation power. When there is little or no absorption of diode laser power at the tip of the fiber, the laser power penetrates deep into tissue, heating up tissue and adjacent sensitive structures. However, diode laser power in the range of 1 W to 7 W is simply not sufficient to cut soft tissue with direct laser light. Thus, standard diode lasers cut exclusively based on the hot-tip effect.
Diode laser manufacturers have noted this issue and now suggest initiating laser fibers using cork or articulating paper. These non-standardized techniques do not guarantee consistent initiation, nor does the initiation last longer than a few seconds while cutting tissue. The diode relies heavily on constant reinitiating by denatured protein to work as a cutting instrument, resulting in fluctuations in cutting temperature, cutting efficiency, and the coagulation zone during a procedure. This inconsistent cutting effect directly impacts cutting performance and collateral thermal damage. Uncontrolled collateral thermal damage is the visible result of temperature fluctuations; the time on tissue is variable but is always longer than with all other heat-based techniques. Diode laser manufacturers have proposed procedures for tip initiation that accelerate the hot-tip creation but do not guarantee complete initiation or consistency over time.9,10
Advances in Surgical Techniques
A new generation of diode laser technology, Thermo-Optically Powered (TOP) surgery, has been developed with the goal of meeting the challenges and issues associated with conventional contact surgical technologies as discussed above. In research leading to the development of the new diode laser technology, the key factors contributing to thermal conductive cutting were evaluated. The objective was to provide a cutting instrument with optimized cutting temperature, stabilized temperature and thermal power, protection from inadvertent overheating of sensitive structures, and reduced technique sensitivity.
TOP surgery technology cuts, cauterizes, and disinfects soft tissue for oral surgery11-13 using a computer-controlled semi-conductor laser as a power source whose power is converted into thermo-optical power in the system’s thermo-optically powered tip. Real-time sensors continuously monitor the thermal power at the tip. A regulating mechanism continuously adjusts the output power of the laser to ensure constant preset temperature at the tip, thus maintaining constant cutting conditions for soft tissue that are almost independent of the speed of cutting.
The power source of the TOP surgery system is a laser. Laser light is monochromatic, ie, light of one specific wavelength, with low absorption in oral soft tissue.14 In the TOP system, this light is transported to the unique tip, where the laser light undergoes a conversion from monochromatic light to thermal power and polychromatic light with wavelengths in the range of 1,400 nm to 11,000 nm. The vast majority of the laser light power is consistently converted to thermal power in the surgical tip of the TOP system. The thermal power that is created in the system’s tip constitutes the primary cutting mechanism. During surgery, the tip is in direct contact with soft tissue, and thermal power is transported to the soft-tissue surface conductively for a thermo-mechanical cut. The dentist maintains tactile feedback at all times during the cutting process.
A part of the initial laser light is converted to optical power—polychromatic infrared light that radiates from the tip with wavelengths from about 1,400 nm to 11,000 nm. The tip is a quartz glass fiber with sintered particles and ions integrated into the glass structure, highly absorbing laser light. Figure 2 and Figure 3 show optical and thermal images, respectively, of a TOP tip. Laser irradiation is highly absorbed at the distal end of the tip, with the tip heating up to 500°C to 900°C (image in Figure 3 acquired with a thermal camera). The heated tip emits incandescent thermal radiation with spectrum and power as described by Plank’s law.15
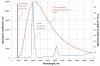
This radiation has a broad polychromatic spectrum with very little power in the visible range, resulting in an orange glow visible from the tip (Figure 2). Figure 4 shows a calculated spectrum of the TOP tip thermal radiation with a temperature of 700°C. These wavelengths of thermal radiation are highly absorbable by soft tissues because they are overlapping with high peaks of water absorption in the mid-infrared range. The average absorption coefficient for this polychromatic infrared radiation is in the range of 700 cm-1 to 850 cm-1, which is very close to the absorption coefficient of a CO2 laser (having a 10,600 nm wavelength and absorption coefficient of 630 cm-1),13 which is known for its excellent soft-tissue cutting and coagulation capabilities. The absorption of this emitted optical radiation by soft tissue during cutting has an enhancing effect on the cutting and cauterizing power of the TOP surgical system. The result is that the laser tip will cut faster and cauterize tissue for hemostasis more effectively because the optical power emitted from the tip produces a CO2 laser-type tissue effect. The tip works as a wavelength energy converter, transforming poorly absorbed near-infrared light from a diode laser with a wavelength of about 980 nm and tissue absorption coefficient of about 0.5 cm-1 to a highly absorbed mid-infrared thermal radiation with a wavelength of 1,400 nm to 11,000 nm and an average tissue absorption coefficient of about 700 cm-1 to 850 cm-1 (Figure 4).
The tip is a key element of a TOP surgery system; it is designed to continuously convert most of the initial laser power into thermo-optical power. In research, the temperature range of the tip, which provides an optimal balance between efficient cutting and patient safety, was determined to be between 500°C and 900°C. Since this temperature is the temperature of the tip, and not of the tissue, the tissue temperature is much lower during cutting. The TOP surgery system allows the user to set the tip temperature anywhere within this range, or preprogrammed presets for the most common dental surgical procedures with optimized temperature settings can be used. A computer-controlled tip initiation process reproducibly creates a unique 3-dimensional (3-D) initiated laser tip. The tip initiation can be performed by a dental professional in-office with a built-in initiation module.
A core functionality of the TOP surgery system is the ability to precisely maintain constant temperature at the tip independent of the speed of the surgeon’s hand. This is made possible by a real-time temperature sensing and adjustment system. The temperature selected by the operator is maintained independent of the speed of movement through the tissue or the type and consistency of the tissue—a fundamental advancement in thermal cutting. This regulating mechanism dramatically reduces the effect of the movement speed as a variable. The cutting effect and the zone of thermal necrosis are constant for each temperature setting used, which significantly reduces the variability of depth of cut and collateral thermal damage due to changes in speed of movement. When necessary, this automatic power control delivers more power for fast cutting or cutting of fibrotic tissue, and minimizes power output for reduced cutting speeds to protect the patient. The TOP automatic power control (Figure 5) produces a deeper cut with minimal collateral thermal damage versus a cut performed with fixed power (Figure 6). Additionally, for safety the surgery system is capable of sensing a stop in hand movement and shuts down the power to avoid tissue overheating.
Connection Between Cutting Depth, Collateral Tissue Damage, and Speed of Cutting
The images shown in Figure 7 and Figure 8 represent a series of photos (top row) and histology (bottom row) of soft-tissue cutting at five different speeds of movement, ranging from 12.5 mm per second to 0 mm per second (stop for several seconds) performed with a traditional diode laser using fixed power (Figure 7) and TOP surgery with automatic power control (Figure 8).13 These experiments were performed using a translation stage with programmable speed and controlled vertical force between the fiber and the sample. To visualize tissue damage, nitro blue tetrazolium chloride (NBTC) viability staining was used, so stained areas show live cells, while cells in white areas are dead. This stain became a standard tool to visualize tissue thermal damage in laser surgery.16,17 It is characteristic that when the speed decreases, the cutting depth and level of collateral tissue damage and carbonization increase sharply for diode lasers, but they remain essentially the same with the new laser technology. The histological evaluations (Figure 7 and Figure 8) illustrate how the influence of cutting speed can reduce tissue damage with automated power control.
Conclusions
Developments in soft-tissue contact laser surgery are resulting in the creation of a new generation of lasers. New technology is enabling consistent use of thermal power generated from poorly absorbed laser radiation; computer-controlled, highly reproducible fiber initiation; and the ability to maintain a pre-selected temperature of the fiber tip with automated power control. These innovations in diode laser technology are aimed at significantly reducing dependence on operator technique, particularly for cutting speed; they allow consistent cutting and minimize snag, drag, and collateral thermal damage of the tissue. This may improve the clinical outcome in soft-tissue surgery while controlling the side effects in wound healing.
DISCLOSURE
The author has no affiliation with any products mentioned in this article.
ABOUT THE AUTHOR
Georgios E. Romanos, DDS, PhD, Prof Dr med dent
Professor and Associate Dean for Clinical Affairs, Department of Dental Medicine, Stony Brook University School of Dental Medicine, Stony Brook, New York
Queries to the author regarding this course may be submitted to authorqueries@aegiscomm.com.
REFERENCES
1. Glover JL, Bendick PJ, Link WJ. The use of thermal knives in surgery: electrosurgery, lasers, plasma scalpel. Curr Probl Surg. 1978;15(1):1-78.
2. Goharkhay K, Moritz A, Wilder-Smith P, et al. Effects on oral soft tissue produced by a diode laser in vitro. Lasers Surg Med. 1999;25(5):401-406.
3. Wray S, Cope M, Delpy DT, et al. Characterization of the near infrared absorption spectra of cytochrome aa3 and haemoglobin for the non-invasive monitoring of cerebral oxygenation. Biochim Biophys Acta. 1988;933(1):184-192.
4. Roggan A, Friebel M, Dörschel K, et al. Optical properties of circulating human blood in the wavelength range 400-2500 nm. J Biomed Opt. 1999;4(1):36-46.
5. Optical absorption of water compendium. Oregon Medical Laser Center Web site. http://omlc.ogi.edu/spectra/water/abs/index.html. Accessed October 30, 2013.
6. Romanos GE, Pelekanos S, Strub JR. Effects of Nd:YAG laser on wound healing processes: clinical and immunohistochemical findings in rat skin. Lasers Surg Med. 1995;16(4):368-379.
7. Verdaasdonck RM, Jansen ED, Holstege FC, Borst C. Optically modified fiber tips penetrate only when “dirty.” SPIE Digital Library. 1990;1201:129-36. doi:10.1117/12.17527
8. Verdaasdonk RM, van Swol CF. Laser light delivery systems for medical applications. Phys Med Biol. 1997;42(5):869-894.
9. van As G. The Diode Laser—Tip Selection and Initiation of the Tip. AMD Lasers Web site. http://www.amdlasers.com/media/articles/Dentistry_Today/tip_initiation.pdf. Accessed October 1, 2013.
10. Christensen GJ. Are Diode Lasers Worth the Investment? Clinicians Report. June 2012;5(6):1-2.
11. Feldchtein FI, Magid KS, Belikov AV, et al. Soft tissue surgery with a 980 nm diode laser: direct laser cutting or hot tip? [abstract]. ALD 2011 Annual Meeting. San Diego CA: Academy of Laser Dentistry; 2011. Abstract TH-13.
12. Magid KS, Belikov AV, Pushkareva A, et al. Soft tissue surgery with thermo-optical tips with a real-time temperature control [abstract]. ALD 2010 Annual Meeting. Miami FL: Academy of Laser Dentistry; 2010. Abstract TH 27-28.
13. Altshuler G. Thermo Optically Powered (TOP) Surgery: A new opportunity for the dental practice. ALD 2012 Annual Meeting. Scottsdale, AZ: Academy of Laser Dentistry; keynote lecture 2012.
14. Manni JG. Dental Applications of Advanced Lasers (DAAL). Burlington, MA: JGM Associates, Inc.; 2007:240.
15. Howell JR, Siegel R, Mengüç MP. Thermal Radiation Heat Transfer. 5th ed. Boca Raton, FL: CRC Press Taylor & Francis; 2011.
16. Neumann RA, Knobler RM, Pieczkowski F, Gebhart W. Enzyme histochemical analysis of cell viability after argon laser-induced coagulation necrosis of the skin. J Am Acad Dermatol. 1991;25(6 Pt 1):991-998.
17. Sherwood ME, Flotte TJ. Improved staining method for determining the extent of thermal damage to cells. Lasers Surg Med. 2007;39(2):128-131.