You must be signed in to read the rest of this article.
Registration on CDEWorld is free. Sign up today!
Forgot your password? Click Here!
Halitosis is a universal affliction suffered by many individuals irrespective of age, sex and social status. Halitosis, or oral malodor, is a common term used to define an unpleasant or an offensive odor in expired air.1 Clinically, some individuals may present with self-perceived halitosis (described as halitosis complaint lacking objective confirmation with diagnostic methods such as a halimeter)2 while others may seek treatment as a result of a complaint from their spouse, relatives or friends. The prevalence of halitosis is highly variable within the general population; ranging from 22% to more than 50%.3 An estimated 8 to 50% of the developed world’s population report the perception of persistent episodes of oral malodor.4 Ashwath et al found that among Indian dental students reporting self-perceived halitosis, that females self-reported at 35.5% versus 21.7% for males.5 Multiple studies report higher percentages of subjective halitosis among those aged 30 years and older.1,6-11
Halitosis has a multi-factorial etiology including extra-oral, intra-oral and psychological factors.5,11 In approximately 80-90% of cases, oral malodor originates intraorally and includes the following factors: bacterial reservoirs on the dorsum of the tongue, plaque biofilm, periodontal pockets, xerostomia and extensive carious lesions with exposed dental pulps. Other oral causes identified in the literature include pericoronitis, mucosal ulcerations, food impaction, debris accumulation, unclean dentures and habitual mouth breathing.12-17 Of the aforementioned factors, tongue coating has been identified as having a significant role in the etiology of halitosis. According to Quirynen et al, tongue coating was the predominant cause of halitosis either alone (43.3%) or in combination with gingivitis and periodontitis (18.2%).17 The irregular texture of the dorsum of the tongue is an ideal niche for oral anaerobic bacteria to putrefy the debris, producing volatile sulphur compounds (VSCs), hydrogen sulphide and methyl mercaptan, all reported to be responsible for oral malodor.13,16-21
Concern about oral malodor can significantly impede an individual’s personal, professional and public life which can lead to the development of social anxiety.22 Social anxiety is the extreme fear of being scrutinized and negatively judged by others in social or performance situations. Individuals with social anxiety are typically shy when meeting new people, quiet in groups and withdrawn in unfamiliar social settings. They avoid speaking in public, expressing opinions or even fraternizing with peers.22-24 Also, it is suggested that anxiety influences the production of VSCs by stimulating autonomic nervous system (ANS).6,7,25-27 As a consequence to ANS stimulation, adrenalin and noradrenalin secretion is enhanced, similar to fight or flight response thereby, reducing the salivary flow. This decrease in salivary flow further impairs the self-cleansing properties of the mouth, thus enabling tongue coating and potential malodor to develop.28,29 Therefore, social anxiety plays a pivotal role leading to halitosis. Against this background, the present study was conducted to assess the association between social anxiety with oral hygiene and tongue coating among patients with subjective halitosis.
Methods
A cross-sectional study was carried out to assess the association between social anxiety with oral hygiene status and tongue coating among patients with subjective halitosis. The study was conducted in the outpatient department, Panineeya Institute of Dental Sciences and Research Centre, Department of Oral Medicine and Radiology during the 5 month period from January 2016 to May 2016. Approval for the study was obtained from the Institutional Review Board at Panineeya Institute of Dental Sciences and Research Centre.
Subjects aged 18 years or older presenting in the outpatient department with the complaint of halitosis were invited to participate in the study. Individuals with the following conditions: history of antibiotic usage over the last month; systemic medical conditions including pregnancy, diabetes mellitus, renal disease, and immunosuppression; oral infections such as dental abscess; respiratory infections; history of tobacco use; and complete or partial denture wearers, were excluded from the study. Interested participants received an explanation of the study procedure and completed an informed consent form. Participation was voluntary and anonymity and confidentiality was maintained.
Social anxiety was assessed with the 24-item Liebowitz Social Anxiety Scale-Self Report version (LSAS-SR) developed in 1987 by Michael Liebowitz. The assessment instrument was available in both English and local vernacular language (Telugu).30,31 LSAS-SR measures social interaction (S) (11 items) and performance (P) (13 items) in terms of fear and avoidance. Both fear and avoidance were rated on a 4-point Likert scale (Fear: 0- none, 1-mild, 2-moderate and 3- severe; Avoidance: 0-none, 1-occasionally, 2-usually and 3-often) in the last week. The LSAS-SR also provides six subscale scores: social-interaction fear, social-interaction avoidance, total fear, performance fear, performance avoidance, total avoidance along with total LSAS-SR score. Individual total scores ranged from 0-144 with the total fear/total avoidance varying from 0-72. Sociodemographic details were also collected including age, gender and level of education.
Oral Examination
The clinical examination included an assessment of the oral hygiene status using the Simplified Oral Hygiene Index (OHI-S) by Greene and Vermillion.32 Tongue coating was evaluated using Tongue Coating Record (TCR) by Shimizu et al.33
Data analyses were performed using the Statistical Package for Social Sciences Software (SPSS Version 21.0). Descriptive statistics were computed for the demographic variables. Mean score was calculated for each item, sub-scales and the total LSAS-SR. Likewise, the mean Debris Index simplified (DI-S), Calculus Index- Simplified (CI-S) and Simplified Oral Hygiene Index (OHI-S) scores were calculated. The Tongue Coating Record (TCR) was used to calculate mean percentage of tongue coating affecting the study population. Comparison of variables (gender) was carried out by t-test and Mann Whitney U test. ANOVA was used for comparison of 3 or more groups (educational levels). Correlation of social anxiety, oral hygiene status and tongue coating was assessed using Pearson’s correlation coefficient method. The level of significance (p value) was set at p<0.05. The validity and reliability of the questionnaire was tested using Cronbach’s alpha.
Results
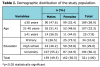
A total of 321 adults with self-reported halitosis presenting to the outpatient department, Panineeya Institute of Dental Sciences and Research Centre, Department of Oral Medicine and Radiology, were included in the study. A total of 159 males (49.5%) and 162 females (50.5%) participated. The majority of the study participants (n=189) were aged 30 years or younger (58.9%) and the majority of the participants (n=194) had completed a university education (60.4%) (Table I).
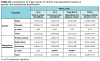
Gender-wise comparisons of questionnaire items revealed that, in the fear subscale females had higher mean scores as compared to males for all the items except “Trying to pick up someone” (I21). However statistical significance was observed only for “Using a telephone in public” (I1) (p=0.03*), “Talking to someone in authority (p=0.01*) (I5), “Going to a party” (I7) (p=0.006*), “Calling someone you don’t know very well” (I10) (p= 0.004*), “Talking face to face with someone you don’t know very well” (I11) (p=0.006*). Overall, for the fear subscale, the highest mean was noted for “Acting, performing or speaking in front of an audience” (I6) (1.83). A similar tendency was identified for the avoidance subscale, with females demonstrating statistically significant higher scores only for “Going to party” (I7) (p=0.02*), “Meeting strangers” I12 (p=0.03*), “Urinating in public bathroom” (I13) (p=0.03*) and “Giving party” (I23) (p=0.04*) (Table II).
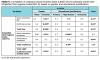
The total Liebowitz Social Anxiety Scale (LSAS) for the study population was 61.41±24.09 with females having a significantly higher score (64.64±24.95; p=0.01*). Likewise, for the subscales: social interaction fear (13.57±7.20; p=0.001*), performance fear (16.35±7.97; p=0.02*) and social interaction avoidance (16.22±6.69; p=0.04*), females had significantly higher scores compared to males. When subscales total fear and total avoidance were compared, a significant difference was found regarding gender only for total fear (p=0.004*) with females having higher scores (32.15±14.32) (Table III).
When educational levels were taken into consideration, higher mean scores for all the subscales were noted for those with lower levels of education i.e., primary school. Moreover, with the exception of performance avoidance (p=0.17), all other subscales and total scores were significantly higher for those with lower (primary school) educational qualifications (Table III).
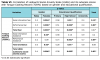
Gender-wise comparison of clinical oral parameters revealed that poor oral hygiene (2.45±1.06) with more tongue coating score (71.38±18.24) was observed among males. However, the scores were statistically insignificant. With regard to education levels, significantly higher scores were recorded for CI-S (0.004*) and OHI-S (p=0.007*) among subjects with lower (primary school) levels of education (Table IV).
The OHI-S and TCR% revealed a significant and positive correlation with total LSAS and its subscales except for performance avoidance and total avoidance subscales. Wherein, subjects with high anxiety had high OHI-S score and high TCR percentage indicating poor oral hygiene status (Table V and Table VI).
Based on gender, OHI-S and TCR percentage showed a significant positive correlation among females for total LSAS and its subscale scores. However, insignificant correlations were found between OHI-S and performance avoidance (p=0.7) and total avoidance subscales (p=0.1)S. Furthermore, gender wise correlation between TCR percentage and social anxiety and its subscales revealed an insignificant correlation among females for only the performance avoidance subscale (p=0.09) (Table V and Table VI).
Likewise, based on levels of education, OHI-S and TCR percentage showed positive correlation with the social anxiety scale and its subscale scores, significant correlations were observed only for the social interaction fear (p=0.01*), performance fear (p=0.003*), total fear (p=0.003*), performance avoidance (p=0.001*) and total avoidance (p=0.01*) subscales, and total LSAS score (p=0.0003*) with TCR percentage only among subjects who had high school qualification (Table V and Table VI).
Discussion
Oral odors are essential clues in the creation and conservation of social bonds. Halitosis as a medical term, was first coined in 1921 by the Listerine Company to describe unpleasant breath, regardless of its sources.11 There are several agents that can temporarily mask the malodor such as mouth rinses, chewing gum, etc., which in turn may prevent the individual from seeking definitive treatment from an oral health professional. While halitosis is most often associated with oral causes, its presence may have serious medical implications as there are numerous medical conditions that predispose one to oral malodor. Halitosis is a common condition with serious social stigmas that may lead to individuals to becoming anxious and stressed in their daily lives. Therefore, identifying a need to enhance knowledge regarding the relationship of self-perceived halitosis, social anxiety and clinical diagnostic factors.5 Halitosis, whether real or perceived, is a cause of concern, embarrassment and frustration on the part of the both sufferer and the general public, and has been shown to lead to social isolation, divorce proceedings, and even contemplation of suicide.11
There are very few studies evaluating subjective halitosis and its social impact. Therefore, the present study was undertaken to explore the association between social anxiety with oral hygiene and tongue coating among patients with subjective halitosis. To evaluate the social impact of halitosis on the study population, Liebowitz Social Anxiety Scale-Self Report version (LSAS-SR) was used.30,31 The LSAS is recognized by the International Consensus Group on Depression and Anxiety as the gold standard for evaluating the clinical impact of social anxiety in an individual.26 The merit of LSAS scale compared to other social anxiety measures- [Social Interaction Anxiety Scale (SIAS), Social Phobia Scale (SPS), Social Avoidance and Distress Scale (SADS) and Fear of negative Evaluation Scale (FNE)] is that, LSAS assesses both anxiety and avoidance in specific situations, rather than assessing specific symptoms. Also, the psychometric properties of the self-report version were found to be as satisfactory as the clinician administered format, with added advantage of being easier and faster.32 In the present study, the validity of the questionnaire was 0.81.
In a study by Miyazaki et al, wherein the correlation between volatile sulphur compounds and certain oral health measurements in the general Japanese population was estimated, it was reported that tongue coating was the main cause of halitosis among the young female subjects.10 Another study by Delanghe et al revealed that of the intraoral causes of halitosis, 51% was associated with tongue coating, 17% due to gingivitis, 15% as a result of periodontitis and 17% was the result of the combination of the previous conditions. In order to objectively measure tongue coating and correlate it with the self-reported complaint of halitosis, the Tongue Coating Record (TCR) was employed in this study. Apart from its reliability and reproducibility, the index had good inter-observer agreement (0.66) and intra-observer agreement (0.80).33
In comparison to an Italian study by Settineri et al, where a higher number of female participants (59.2%) presented with subjective halitosis,6 the present study had comparable numbers of male (49.5%) and female (50.5%) participants.
The majority of the participants had a university education (60.4%) demonstrating a higher concern among educated subjects with respect to their self-image, which might be lowered due to bad breath. Similar findings were observed in a study among Kuwaiti patients with a university education (66.2%).35 Contrary findings come from a study conducted by Youngnak-Piboonratanakit et al, among Thai dental patients from Chulalogkorn Dental Hospital. Subjects with lower education levels (77.7%) dominated the study population as compared to those with a university education (66.2%).7
When individual items of LSAS were taken into consideration, such as the fear subscale, females reported higher mean scores for all the items except for Item-21 (Trying to pick someone up). This could be due to the fact that women may be more phobic and less willing to interact in a strange/unknown situation due to their bad breath. On the other hand, avoidance subscale showed comparable mean scores between males and females. The overall LSAS and its subscale mean scores were significantly lower for males, indicating that males were less anxious when compared to females. Less anxiety among men could be attributed to the fact that, they have higher self-esteem and less introverted tendencies as compared to women and they may seldom avoid social situations. Similar findings were also reported among Japanese26 and American36 populations where females posed a greater risk of having social anxiety as compared to males.
However, significantly lower mean scores for LSAS and its subscale (except the performance avoidance subscale), was noted among subjects with a higher level of education in this study. This could be because subjects with higher or university education, indulge in good oral hygiene practices as evidenced with the overall good oral hygiene score (2.22±1.08) and Tongue Coating Record (69.55±18.44) when compared to subjects with a lower education in the current study.
In a study by Liu et al among Chinese individuals, it was found that a significant correlation existed between volatile sulphur compounds (VSCs) and oral hygiene status (plaque index and calculus index) among various age groups wherein females outnumbered males.13 Whereas, in the present study, poor oral hygiene scores based on OHI-S and TCR index were found among males, which may be attributed to the fact that females are invariably more concerned about oral hygiene and appearance and may be spending more time on oral hygiene maintenance as compared to males. This was further supported by this study’s finding of a positive correlation between total LSAS, its subscale and the oral clinical parameters among females, thus signaling a higher level of concern about their oral hygiene.
The present study acknowledges certain limitations; such as the cross-sectional nature of the study which was confined to a single institution, therefore, the results cannot be generalized beyond the study population. The effects of age, gender and education in regards to the etiology and self-perception of halitosis could not be clearly established. Lastly, there was a lack of correlation between subjective halitosis and clinical or laboratory-based evaluations made using halimeter, gas chromatography and organoleptic methods.
Conclusion
The current study revealed that social anxiety, poor oral hygiene and tongue coating were associated with subjective halitosis. Also, it may be concluded that halitosis may pose a serious oral health problem with an extensive social impact on its sufferers. Maintenance of good oral health along with the use of appropriate tongue cleaning methods is of utmost importance in reducing oral malodor. In some cases, however, a comprehensive treatment of halitosis may require a multidisciplinary approach by a team of dental, psychology and counselling professionals.
About the Authors
Jenisha Patel, BDS is a post graduate student; Suhas Kulkarni, MDS is the department head and professor; Dolar Doshi, MDS is a professor; Madupu Padma Reddy, MDS is a professor; Srikanth Reddy, MDS is a reader; Adepu Srilatha, MDS, is a senior lecturer; all in the Department of Public Health Dentistry, Panineeya Institute of Dental Sciences and Research Centre, Hyderabad, India
Corresponding author: Jenisha Patel, BDS; jenisha.patel91@gmail.com
References
1. Bornstein MM, Kislig K, Hoti BB et al. Prevalence of halitosis in the population of the city of Bern, Switzerland study comparing self reported and clinical data. Eur J Oral Sci 2009 Jun;117(3):261-7.
2. Ozen ME, Aydin M. Subjective halitosis: Definition and classification. J N J Dent Assoc 2015 Fall;86(4):20-4.
3. Cortelli JR, Barbosa MD, Westphal MA. Halitosis: a review of associated factors and therapeutic approach. Braz Oral Res 2008;22 (Suppl 1):44-54.
4. Porter SR, Scully C. Oral malodour (halitosis). BMJ 2006;333(7569):632-5.
5. Ashwath B, Vijayalakshmi R, Malini S. Self-perceived halitosis and oral hygiene habits among undergraduate dental students. J Indian Soc Periodontol 2014 May;18(3):357-60.
6. Settineri S, Mento C, Gugliotta SC et al. Self-reported halitosis and emotional state: impact on oral conditions and treatments. Health Qual Life Outcomes 2010 Mar 26;8:34.
7. Youngnak-Piboonratanakit P, Vachirarojpisan T. Prevalence of self-perceived oral malodor in a group of Thai dental patients. J Dent (Tehran) 2010 Fall;7(4):196-204.
8. Nadanovsky P, Carvalho LBM, Ponce de Leon A. Oral malodour and its association with age and sex in a general population in Brazil. Oral Dis 2007 Jan;13(1):105-9.
9. Nalcaci R, Baran I. Factors associated with self-reported halitosis (SRH) and perceived taste disturbance (PTD) in elderly. Arch Gerontol Geriatr 2008 May-June;46(3):307-16.
10. Miyazaki H, Sakao S, Katoh Y et al. Correlation between volatile sulphur compounds and certain oral health measurements in the general population. J Periodontol 1995 Aug;66(8):679-84.
11. Arora L, Sharma A. A study to find out the dental and associated psychosocial factors in patients of halitosis. Deli Psychiatry Journal 2012;15(1):122-9.
12. Lawande SA, Lawande GS. Tongue hygiene and its significance in the control of halitosis. J Orofac Res 2013;3(4):256-62.
13. Liu XN, Shinada K, Chen XC et al. Oral malodor-related parameters in the Chinese general population. J Clin Periodontol 2006 Jan;33(1):31-6.
14. Evirgen S, Kamburoglu K. Effects of tongue coating and oral health on halitosis among dental students. Oral Health Prev Dent. 2013;11(2):169-73.
15. Vali A, Roohafza H, Keshteli AH et al. Relationship between subjective halitosis and psychological factors. Int Dent J 2015 Jun;65(3):120-6.
16. Kursun S, Acar C, Atakan C et al. Relationship between genuine halitosis and pseudohalitosis and social anxiety disorder. J Oral Rehabil 2014 Nov;41(11):822-8.
17. Quirynen M, Dadamio J, Van de Velde S et al. Characteristics of 2000 patients who visited a halitosis clinic. J Clin Periodontol 2009 Nov;36(11):970-5.
18. Veeresha KL, Bansal M, Bansal V. Halitosis: a frequently ignored social condition. J Int Soc Prev Community Dent 2011 Jan;1(1):9-13.
19. Hinode D, Fukui M, Yokoyama N et al. Relationships between tongue coating and secretory-immunoglobulin A level in saliva obtained from patients complaining of oral malodor. J Clin Periodontol 2003 Dec;30:1017-1023.
20. Calil C, Liberto FL, Pereira AC et al. The relationship between volatile sulphur compounds, tongue coating and periodontal disease. Int J Dent Hyg 2009 Nov;7(4):251-5.
21. van den Broek AM, Feenstra L, de Baat C. A review of literature on aetiology and measurement methods of halitosis. J Dent 2007 Aug;37(8):627-35.
22. McKeown L. Social relations and breath odour. Int J Dent Hyg 2003 Nov;1(4):213-7.
23. Stein MB, Stein DJ. Social anxiety disorder. Lancet 2008 Mar;371(9618):1115-25.
24. Beard C, Rodriguez BF, Moitra E et al. Psychometric properties of the Liebowitz Social Anxiety Scale (LSAS) in a longitudinal study of African Americans with Anxiety Disorders. J Anxiety Disord 2011 Jun;25(5):722-726.
25. Calil MC, Marcondes FK. Influence of anxiety on production of oral volatile sulfur compounds. Life Sci 2006 Jul;79(7):660-4.
26. Zaitsu T, Ueno M, Shinada K et al. Social anxiety disorder in genuine halitosis patients. Health Qual Life Outcomes 2011 Nov 3;9:94.
27. Queiroz CS, Hayacibara MF, Tabchoury CP et al. Relationship between stressful situations, salivary flow rate and oral volatile sulfur containing com pounds. Eur J Oral Sci 2002 Oct;110(5):337-40.
28. Eldarrat A, Alkhabuli J, Malik A. The prevalence of self-reported halitosis and oral hygiene practices among Libyan students and office workers. Libyan J Med 2008 Dec 1;3(4):170-6.
29. Koshimune S, Awano S, Gohara K et al. Low salivary flow and volatile sulfur compounds in mouth air. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2003 Jul;96(1):38-41.
30. Santos LF, Loureiro SR, Crippa JA et al. Can the Liebowitz Social Anxiety Scale - Self Report Version be used to differentiate clinical and non-clinical SAD groups among Brazilians? PloS One 2015 Mar 26;10(3):e0121437.
31. Heimberg RG, Horner KJ, Juster HR et al. Psychometric properties of the Liebowitz Social Anxiety Scale. Psychol Med 1999 Jan;29(1):199-212.
32. Greene JC, Vermillion JR. The Simplified Oral Hygiene Index. J Am Dent Assoc 1964 Jan;68:7-13.
33. Shimizu T, Ueda T, Sakurai K. New method for evaluation of tongue coating status. J Oral Rehabil 2007 Jun;34(6):442-7.
34. Delanghe G, Ghyselen J, van Steenberghe D et al. Multidisciplinary breath-odour clinic. Lancet 1997 Jul;350(9072):187.
35. Al-Ansari J, Boodai H, Al-Sumait N et al. Factors associated with self-reported halitosis in Kuwaiti patients. J Dent 2006 Aug;34(7):444-9.
36. Turk CL, Heimberg RG, Orsillo SM et al. An investigation of gender differences in social phobia. J Anxiety Disord 1998 May-Jun;12(3):209-2.