You must be signed in to read the rest of this article.
Registration on CDEWorld is free. Sign up today!
Forgot your password? Click Here!
Dental hygienists often experience musculoskeletal disorders (MSD) during the course of their careers, frequently as a result of the sustained grips on instruments, uncomfortable body positioning, and repetitive movements they practice throughout the work day.1 While these injuries can occur in any part of the body, a recent review has revealed that 42% to 69% of dental hygienists reported MSD in the hand and wrist region.1 In particular, carpal tunnel syndrome (CTS) is a painful disorder involving the entrapment of the median nerve, which reportedly affects up to 23% of dental hygienists.2 Studies have identified many predictors of hand and wrist pain, including hours working per week, poor work-life balance,3 patients with heavy calculus,4,5 and increasing age.5 Pain and fatigue may be associated with decreased hand strength, and a recent study of female dentists has identified that those with a low variation in work tasks were at an increased risk of lowered strength in their right hand6; these findings are concerning for the dental hygiene profession, which is predominantly female and with little variation in clinical procedures.
The practice of good ergonomics is an important strategy to prevent MSD, and currently there are numerous recommendations for improved ergonomics specific to dentistry and dental hygiene. Recommended strategies for reducing the risk of MSD include the use of instruments with large-diameter handles that require less gripping force, and the use textured instruments to allow for easier gripping.7 The use of lightweight instruments (15 grams) with large diameters (10 mm) requires less muscle load and pinch force, thereby reducing the strain and tension that can contribute to the development of MSD.8 A round, tapered handle may also be beneficial.9 Currently, there are few research studies investigating the correlation between instrument handle materials and hand and wrist disorders. It has been suggested that the use of silicone may be a way to reduce the ergonomic stress hand instruments put on the body; this material is designed to improve ergonomics, texture, and weight, which consequently decreases the stress placed on the hand and wrist.10
A study conducted in the United States found 27.8% of respondents reported MSD as the primary cause of reduction in work hours,11 highlighting the detrimental effect an MSD has on an individual’s career and income. MSD can result in increased medical expenses and workers compensation claims as well as higher levels of difficulty completing daily tasks.12 Ergonomically designed dental instruments using silicone handles may contribute to reducing MSD among dental hygienists, subsequently resulting in greater operator comfort, hand strength, and overall productivity.13 A recent study evaluating the efficacy of instruments in dentistry found that the use of thick silicone instrument handles caused the least strain, and improved work productivity, when compared to heavy, metallic instruments.14 The aim of this research project was to investigate the effect of silicone instrument handles on hand comfort and strength when compared to traditional stainless steel instruments.
Materials and Methods
This pilot study was conducted using a comparative cross-sectional study design, to examine and compare the effect of using stainless steel instruments and silicone handled instruments on hand strength and comfort. Institutional Review Board Approval was obtained from the University of Newcastle, Human Research Ethics Committee (H-2014-0024). Students enrolled in their second year of study in the Bachelor of Oral Health program at the University of Newcastle (n = 50) were invited to participate. This particular cohort of students was selected as a convenience sample based on having achieved a satisfactory level of competency in the use of scalers and curettes; however, the participants had not begun performing these skills on patients. In addition, the participants all had the same ergonomics instruction. Students were contacted during a lecture class session and were given a brief introduction and written synopsis of the project informing them of the nature of the research with an emphasis on the voluntary nature of the study participation. Students were given a participant information statement and a consent form to participate and could either return the completed consent form to the lecturer, or return to the on-campus clinic within two weeks.
Participants were required to attend two simulated scaling sessions, exactly one week apart, at the on-campus clinic. To limit external fatigue factors, the sessions were conducted on a day when the students did not have a preclinical scaling lab, and each student attended at the same time and on the same day of the week. In the first session, the participants were required to use the standard issue traditional instruments (stainless steel handle, 10 mm diameter, 21 to 25 g weight) in a simulated scaling task for 30 minutes. The simulated scaling task involved performing debridement of simulated calculus on quadrant four (lower right quadrant) of a typodont fitted into a manikin head. The manikin heads were set up in dental chairs in the campus clinic. Conducting the simulated scaling task in an actual dental clinic chair ensured that the participants could appropriately position themselves and the simulated patient for optimal ergonomics. Participants were provided with a mouth mirror, periodontal probe, 11/12 periodontal explorer, H6/7 sickle scaler, jacquette scaler 34/35, gracey 1/2, gracey 11/12, and gracey 13/14. The only instruction given to the participants was to debride the simulated calculus from quadrant four for a period of 30 minutes; no specific order of instrumentation was dictated. They were then required to complete a short survey, and have their hand grip and pinch strength assessed.
Hand comfort was assessed using the Patient Evaluation Measure (PEM) survey, which is considered to be a valid, reliable, and responsive tool.15 For the purposes of this study, only questions in the hand health profile (part two of the PEM survey) were investigated. Participants responded to statements regarding the feeling, pain (level, type, duration), skill, flexibility, strength, usefulness, appearance, and overall perceptions of their hands, on a 7-point Likert scale with 7 being the most negative response. Participants’ pinch and grip strength were assessed using a hand held pinch gauge and dynamometer, according to the protocols included in the American Society of Hand Therapists guidelines.16
Participants were required to attend a second session one week later, where they were required to use instruments with a silicone handle (Flexichange®, Dentsply Ash®, Lane Cove West, NSW, AU) in the same simulated scaling task for 30 minutes. They were then required to complete the same short survey as the previous week, and have their hand grip and pinch strength assessed.
Data was analyzed using the STATA software package. Means and standard deviations for all outcome measures were calculated. Paired t-tests were used to determine significant differences between the grip strength, pinch strength, and hand health profiles scores after using stainless steel and silicone instrument handles. All results were expressed as t-value with degrees of freedom and 95% confidence intervals, reported as significant with P < 0.05.
Results
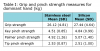
Twenty-three dental hygiene students agreed to participate in this pilot study. The participants were all female, with a mean age of 25.4 years (± 3.75, range 19-41). Means and standard deviations for grip, key pinch, palmer pinch, and tip pinch strength following the use of stainless steel and silicone instruments are presented in Table 1.
A paired t-test was performed to determine whether there was a statistically significant mean difference between the grip and pinch strength after participants used stainless steel instrument handles compared to silicone instrument handles. The results demonstrated that the participant’s grip was stronger after using silicone instruments (27.44 ± 4.64 kg) as opposed to after using stainless steel instruments (26.11 ± 4.81kg); with a statistically significant mean increase of 1.32 kg (95% CI 0.22-2.43, t[22] = 2.48, P < .02). The participant’s key pinch was also stronger after using silicone instruments (4.84 ± 0.99 kg) compared with stainless steel instruments (4.51 ± 0.85 kg); a statistically significant mean increase of 0.33 kg (95% CI 0.00-0.67, t[22] = 2.05, P < .05). There was also an improvement in palmer pinch and tip pinch strength between using stainless steel and silicone instruments, although these findings were not statistically significant.
A paired t-test determined that using silicone instrument handles demonstrated a statistically significant positive change in hand health profile scores. Hand health profile scores were higher (worse) after using stainless steel instruments (30.6 ± 11.4) compared with silicone instruments (24.4 ± 9.0), with a statistically significant mean difference of 6.1 points (t[22] = 3.04, P < .001). Figure 1 shows the specific questions in the Hand Health Profile that were significantly different after using the silicone instruments.
Discussion
This pilot study explored the effect of silicone instrument handles on hand strength and comfort compared to stainless steel handles, a comparison not previously reported in the literature. It was revealed that silicone instrument handles may assist in reducing fatigue in the hand, with a statistically significant improvement in grip strength, key pinch strength, and hand comfort. Previous research has established that lightweight instruments with a larger diameter require less muscle load and pinch force8; it is therefore conceivable that silicone handles would reduce hand fatigue, which is supported by the improved hand strength scores.
There were no statistically significant differences in palmer pinch or tip pinch between the stainless steel and silicone instruments. This may indicate that certain muscle groups fatigue more easily after using the fine motor skills required for the debridement of teeth. However, it should be noted that the mean key, palmer, and tip pinch strength measures were well below the normative values for adults, as established by Mathiowetz and colleagues.17 This may indicate that despite being students, initial training in periodontal instrumentation and debridement may already be affecting finger strength. Previous research has established that participants with CTS have decreased pinch grip.18 The mean grip strength, while less for females established in a healthy population, were within the normative range.19
Participants reported that their hand felt more comfortable after using the silicone instruments, when compared with stainless steel instruments. This finding is consistent with a study by Nevala and colleagues, whereby participants involved in simulated scaling tasks reported that instruments with the thickest silicon handles were more usable and caused less perceived strain that those with thinner, metallic handles.14 It should be noted that the instruments used in this study were color coded, which aids instrument identification and selection10; this design feature may have influenced the students’ positive response to the study instruments. What is not clear is whether the lighter weight, the larger diameter, the texture, or a combination of these elements found in silicone instruments is beneficial over the stainless steel alternatives.
Previous research has established that scaling instrumentation procedures and patients with heavy calculus deposits contribute to hand and wrist pain.4,5 While these tasks cannot be avoided as part of periodontal instrumentation, the ergonomic risks associated with these activities can perhaps be modified through the use of alternative instrument and workplace design. The results from this study should prompt dental practitioners to consider the handle design of periodontal instruments. The “one size fits all” approach to instrument design may not be suitable for all users, and individual dental practitioners should explore which instrument handle best suits their needs. Furthermore, the regular use of ultrasonic scalers in the dental hygienists’ armamentarium may influence hand and wrist MSD despite the use of ergonomically designed hand instruments.
While these subjects were not yet practicing dental hygienists, this research provides promising results for the use of silicone instrument handles in reducing the prevalence of MSD. Manufacturers are constantly developing new tools and technologies to improve the work environment, and it is important to research such developments to ensure the ability to make informed evidence-based decisions on dental practice. Nevertheless, there are aspects of the study that could be improved, and they should be noted in interpreting the results and designing future studies. All participants were required to use the stainless steel instruments in week one, and then the silicone instruments the following week; this lack of randomization increases the potential for confounding factors to be introduced during the week between tasks. Further, the sample was one of convenience; all the participants were enrolled in the same dental hygiene program, and the same institution, and as such, the results are difficult to generalize. The researchers were unable to identify any useful minimal clinically important differences (MCID) to help gauge the importance of this study’s particular results. While the PEM is a valid and reliable tool, the researchers only used the Hand Health Profile portion of the tool in this study, and there appear to be no available MCIDs for this portion of the survey alone. Studies exploring the MCID of grip and pinch strength often measure the magnitude of change following serious injury or surgical intervention; such differences are unlikely to be comparable in a small pilot study such as this, where the magnitude of change would likely be different for participants with lower levels of MSDs. A power analysis was not conducted due to the small sample chosen, which also limits the application of results to the entire profession. Nevertheless, small convenience samples are useful when conducting pilot studies, as they are usually accessible and easily recruited, which is valuable when time and financial constraints are considered.
It is important to remember that the etiology of MSD is multi-factorial, and as such, one intervention alone cannot be a panacea for this occupational problem. There are, of course, a number of strategies that can be employed to reduce the risk of MSD in the hand and wrist of dental hygienists, including taking regular breaks, stretching and strengthening muscles, and keeping instruments sharp.20 Studies exploring prevention of MSD among dental practitioners should investigate a wide range of symptoms and body areas for potential benefits. For instance, research exploring the use of loupes, or surgical magnification, in the reduction of MSD has demonstrated some improvements in the area of hand and pinch grip strength.21
Conclusion
This pilot study suggests that the use of silicone dental instrument handles may reduce fatigue and improve hand comfort among dental hygienists. Longitudinal prospective studies into ergonomic instrument design are recommended among larger cohorts of dental practitioners to determine longer-term outcomes. Dental hygienists should consider the handle design of periodontal instruments as part of an ergonomic assessment of their individual workplace and tasks.
ABOUT THE AUTHOR
Melanie J. Hayes, BOH, BHSc (Hons), PhD, is a senior lecturer at the Melbourne Dental School, University of Melbourne, Melbourne, Australia.
DISCLOSURE
The author would like to acknowledge the support of Dentsply™ for donating the silicone instruments used in this study. The author has no financial affiliation with Dentsply™ and they were not involved in the study design or analysis.
REFERENCES
1. Hayes MJ, Smith DR, Cockrell D. An international review of musculoskeletal disorders in the dental hygiene profession. Int Dent J. 2010;60:343-352.
2. Anton D, Rosecrance J, Merlino L, Cook T. Prevalence of musculoskeletal symptoms and carpal tunnel syndrome among dental hygienists. Am J Ind Med. 2002;42:248-257.
3. Hayes MJ, Taylor JA, Smith DR. Predictors of work-related musculoskeletal disorders among dental hygienists. Int J Dent Hyg. 2012;10(4):265-269.
4. Lalumandier JA, McPhee SD, Parrott CB, Vendemia M. Musculoskeletal pain: prevalence, prevention, and differences among dental office personnel. Gen Dent. 2001;49(2):160-166.
5. Liss GM, Jesin E, Kusiak RA, et al. Musculoskeletal problems among Ontario dental hygienists. Am J Ind Med. 1995;28:521-540.
6. Ding H, Leino-Arjas P, Murtomaa H, et al. Variation in work tasks in relation to pinch grip strength among middle-aged female dentists. Appl Ergo. 2013;44:977-981.
7. Cuny E, Wood AJ. Understanding and preventing musculoskeletal disorders in dentistry. Inside Dent. 2006;2(7).
8. Dong H, Barr A, Loomer P, et al. The effects of periodontal instrument handle design on hand muscle load and pinch force. J Am Dent Assoc. 2006;137(8):1123-1130.
9. Dong H, Loomer P, Barr A, et al. The effect of tool handle shape on hand muscle load and pinch force in a simulated dental scaling task. Appl Ergo. 2007;38(5):525-531.
10. Hodges K. What’s new in hand instruments. Dimensions Dent Hyg. 2005;3(11):26-29.
11. Morse TF, Michalak-Turcotte C, Atwood-Sanders M, et al. A pilot study of hand and arm musculoskeletal disorders in dental hygiene students. J Dent Hyg. 2003;77(3):173-179.
12. Yee T, Crawford L, Harber P. Work environment of dental hygienists. J Occup Environ Med. 2005;47(6):633-639.
13. Simmer-Beck M, Branson BG. An evidence-based review of ergonomic features of dental hygiene instruments. Work. 2010;35:477-485.
14. Nevala N, Sormunen E, Remes J, Suomalainen K. Evaluation of ergonomics and efficacy of instruments in dentistry. Ergon Open J. 2013;6:6-12.
15. Dias JJ, Bhowal B, Wildin CJ, Thompson JR. Assessing the outcome of disorders of the hand: is the patient evaluation measure reliable, valid, responsive and without bias? J Bone Joint Surg. 2001;83B:235-240.
16. Lindstrom-Hazel D, Kratt A, Bix L. Interrater reliability of students using hand and pinch dynamometers. Am J Occup Ther. 2009;63:193-197.
17. Mathiowetz V, Kashman N, Volland G, et al. Grip and pinch strength: normative data for adults. Arch Phys Med Rehab. 1985;66:69-72.
18. Baker NA, Moehling KK, Desai AR, Gustafson NP. Effect of carpal tunnel syndrome on grip and pinch strength compared with sex- and age-matched normative data. Arth Care Res. 2013;65(12):2041-2045.
19. Massy-Westropp NM, Gill TK, Taylor AW, et al. Hand grip strength: age and gender stratified normative data in a population-based study. BMC Res Notes. 2011;4:127.
20. Michalak-Turcotte C. Controlling dental hygiene work-related musculoskeletal disorders: the ergonomic process. J Dent Hyg. 2000;74(1):41-48.
21. Hayes MJ, Osmotherly PG, Taylor JA, et al. The effect of loupes on upper extremity musculo-skeletal disorders among dental hygienists. Int J Dent Hyg. 2014;12(3):174-179.