You must be signed in to read the rest of this article.
Registration on CDEWorld is free. Sign up today!
Forgot your password? Click Here!
The ADAA has an obligation to disseminate knowledge in the field of dentistry. Sponsorship of a continuing education program by the ADAA does not necessarily imply endorsement of a particular philosophy, product, or technique.
The manual dual-arch (or triple tray) technique is an efficient way of making a definitive impression and fabricating provisional restorations for crown and bridge procedures. This continuing education course presents a team approach to triple tray crown and bridge procedures. Topics include taking initial and final impressions, making provisional restorations, mixing impression materials, deciding when to use separate arch impressions instead of the triple tray, and preparing and packaging the patient case for the dental laboratory. While technological advancements may reduce the frequency of use of the manual triple tray impression technique, its intrinsic efficiency still makes it a viable option.
The Triple Tray
The triple tray technique is an efficient method for producing accurate impressions for crowns and bridges in dentistry.1-3 A single, double-sided impression simultaneously captures an impression of the crown preparation, the maxillary arch, the mandibular arch, and the occlusal relationship between the arches (Figure 1).1 The flat surface of the triple tray consists of a piece of mesh, which is thin enough to allow the teeth to occlude closely together and allows the impression material to permeate it. Two basic impression materials, polyether or vinyl-polysiloxane (VPS), both similarly accurate,4-6 are used in the triple tray technique.7-13
In the basic triple tray technique,1,14,15 the assistant takes a preoperative triple tray impression of the area to be prepared, using a medium viscosity VPS or polyether impression material. After the dentist has prepared the tooth/teeth, the assistant uses the preoperative impression as a mold for making a provisional (temporary) restoration for the prepared tooth/teeth. When the provisional restoration is completed, the assistant places a layer of low viscosity (high flow to capture fine details) VPS onto both sides of the triple tray to use as a final impression. The assistant transfers the triple tray to the dentist, who seats the tray intraorally, realigning the impression to capture the fine details of the prepared abutment(s) and the opposing arch. (If a monophase, medium viscosity polyether impression material is used for the preoperative impression, then only this one phase is used for the reline impression). In most US states, only a dentist is legally permitted to obtain and approve a final impression for a crown or bridge. It is imperative that the dental team follow their state law in this matter.
The assistant (when allowed by state law) cements the provisional restoration(s), completes the dental laboratory prescription order according to the dentist’s request, has the dentist review and sign the order, and packages the case for shipping or pickup. The patient is then re-appointed for try-in and permanent delivery of the final crown or bridge.
Four Basic Types of Triple Trays
There are four main types of triple trays used in dentistry: posterior (long and short quadrant), short anterior, long dual-arch (Figure 2).
The posterior triple tray offers two variations. The first is a short quarter-arch tray that captures only posterior teeth. This tray may be needed if a patient has a small mouth. Dentists may prefer use of this tray because it uses less impression material compared to the longer quadrant tray. However, an impression in a posterior triple tray may flex more and have a greater chance of distortion because it uses less material. A disadvantage is that this short posterior tray may not capture enough teeth to ensure capturing the patient’s occlusion.
The second and longer quadrant triple tray is generally used for capturing all posterior and possibly the anterior teeth in a quadrant. The authors recommend the quadrant tray as the tray of choice for capturing posterior abutment preparations, since this tray captures more teeth and, therefore, helps to assure the maximum intercuspation occlusion of the arch. The quadrant tray also holds more impression material that provides a stronger structure to hold the liquid stone model mixture.
The third option is the short anterior triple tray. This tray captures all the anterior teeth and often captures the premolar teeth as well. This is the tray of choice for capturing anterior abutment preparations.
The long dual arch triple tray is a longer version of the short anterior option. This fourth tray can capture posterior teeth, but it may be too bulky for the patient to occlude into when taking a reline impression. The posterior aspect of the tray may be so long that the posterior aspect may bend under the weight of liquid stone.
Separate, full-arch impressions are preferred if the dentist wishes to capture impressions of teeth across multiple arches, or of multiple anterior teeth that extend beyond the midline in addition to simultaneously capturing impressions of posterior teeth.
Properties of Impression Materials Relevant to Triple Tray Impression Success
There are various properties that impression materials should possess to be suitable for triple tray impressions. These properties include: a dimensional accuracy of 1% or less, the ability to revert to their original accurate dimensions after being slightly bent or torqued while being removed from the oral cavity, and the ability to tear just enough during removal should it become locked into undercuts between teeth or under existing bridges in the patient’s mouth, without distorting the impression.15
It is beneficial to only use fast-setting (2-minute set) impression materials with triple tray impressions. Slower-setting materials are not necessary as the triple tray can be quickly loaded and positioned intraorally. Use of fast-setting material helps to prevent the tray from being inadvertently removed from the mouth before the impression has set completely. Also, it is faster and less tedious to take repeated impressions if these are required to capture missed details.
Impression materials set faster in the mouth as compared to the excess material in the operatory because the mouth is a warmer environment compared to the operatory temperature. The intraoral impression is set when it is does not show softness or dimpling to light finger pressure, or if extraoral impression material has also set. Impression materials may also have a manufactured-specified setting time, but the real world setting time may vary, depending on the temperature of the material, or if hand-mixed materials were inadvertently mixed with incorrect proportions of base or catalyst.
Impression materials used in crown and bridge procedures should be hydrophilic (attracted to moisture). A hydrophobic impression material would be repelled by moisture and may not be ideal for dental impressions. Even if a dentist packs cord into a periodontal pocket to reduce moisture, there is often a tiny amount of moisture in the periodontal pocket around the prepared tooth that seeps up onto the prepared tooth. An impression material that is hydrophilic can overcome, and be slightly attracted to this moisture, so the material can penetrate into the periodontal pocket around the abutment and yield an accurate impression. Polyether is a naturally hydrophilic impression material, and can often yield accurate impressions even if there is slight seepage of moisture or blood in a periodontal pocket.16,17 Newer VPS impression materials can be made hydrophilic using special additives.
One Triple Tray vs. Two Separate Arch Impressions
Before taking the preoperative impression, it must be decided if a triple tray impression can be used or if two separate maxillary and mandibular arch impressions should be used.
A triple tray method is acceptable to use if, after the tooth/teeth are prepared into abutments, it is still obvious from the occlusion of the unprepared teeth, how to articulate the teeth together.12 In general, if there are two unprepared posterior teeth in occlusion after the tooth is prepared, or if there is one unprepared posterior tooth and at least one (but ideally at least two) unprepared anterior teeth still in occlusion, the laboratory technician will be able to articulate the opposing arches represented on the triple tray model. In general, the occlusion of opposing posterior teeth is more obvious than the occlusion of opposing anterior teeth, but anterior teeth often have flat or faceted incisal contact points that make occlusion more obvious. The triple tray impression is accurate and appropriate to use for single unit crowns and three-unit bridge preparations, if the aforementioned occlusion reference points for unprepared teeth are present.
If the occlusion reference points are not present or are not obvious, if preparing a bridge where there is no unprepared posterior tooth distal to the bridge abutments, or if a single triple tray impression will not capture all abutment teeth, then two separate impressions of the arches should be made. Also, if a patient has a gag reflex when a triple tray is used, taking separate mandibular stock tray impressions may be more tolerable. If the patient cannot tolerate mandibular stock tray impressions, quarter arch stock tray impressions with a bite registration may be used to reduce the total amount of gag-stimulating impression material needed. Occasionally a patient’s dentition is malposed with teeth in many different directions resulting in closing difficulty into a triple tray when the provisional restoration is being fabricated. Here, separate arch impressions18 prevent the malposed teeth from the two arches from interlocking or interfering with one another.
Typically, the separate arch impressions are made using a medium sized plastic mandibular stock impression tray (Figure 2), but a larger or smaller sized tray may be used as needed. A maxillary stock tray, which needs more impression material, is not necessary because only an impression of the teeth and the edentulous areas between the teeth are required, not an impression of the palate. The amount of impression material in a maxillary stock tray can also trigger the patient’s gag reflex.
For the counter-model impression (the opposite arch), the assistant fills one-half to two-thirds of the impression tray with medium viscosity VPS, and then fills the rest of the tray with low viscosity VPS. The assistant then suctions moisture and debris from the mouth, dries the teeth with air, and seats the tray. The bottom layer of medium viscosity VPS helps to push the top layer of low viscosity VPS into the teeth, helping to ensure a precise impression. The counter-model impression does not have to be relined later with a low viscosity impression material to capture more details, as long as it captures all of the teeth that occlude into the teeth that will be prepared and captures at least the incisial three millimeters of the teeth. The counter-model impression would need a reline later if the dentist adjusts teeth in the arch opposing the prepared teeth.
For the arch that contains the tooth that will be prepared, the assistant first takes a medium viscosity impression. After the tooth is prepared, this impression will be relined with a low-viscosity impression material to capture the abutment details.
Alginate vs. VPS or Polyether for Counter-Model Impressions
Alginate impression material should not be used for counter-model impressions. Alginate can distort unless a stone model is poured up within approximately 10 minutes of making the alginate impression.19-21 Some offices may make the alginate counter-model impression and not pour it up immediately. Instead, the impression is wrapped in a paper towel moistened with disinfectant, and placed in a plastic bag to prevent moisture evaporation. Whether it is poured on site or sent to the dental laboratory for pouring, this time delay will have allowed the impression to distort.
A counter-model impression made with VPS or polyether is more accurate than alginate. VPS is stable for weeks in open air without distorting, while polyether is stable for about a week in air before it starts to distort.4,22 Unlike alginate impressions, VPS or polyether impressions should not be wrapped in a moist paper towel before sending them to the dental laboratory, but instead should be disinfected, dried, and stored dry.21 These materials do not need to be immediately poured up; an experienced dental laboratory technician can do so instead.
Manual vs. Automatic Mixing of Impression Materials
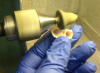
Impression materials can be mixed manually, via hand spatulation, or automatically, by using a hand-powered impression gun or an automated mixing machine12,23-24 (Figure 3).
To mix impression material by hand, the base and catalyst components of the impression material are placed on a mixing pad. Typically, equal lengths of each material are dispensed, such that the total amount of impression material that will be mixed will cover the triple tray. A wide hand spatula is used to mix the two components, by smearing the components together, and then using the edge of the spatula to incorporate the impression material into a pile, followed by smearing the material together again using an infinity motion - ∞ - into the pad surface. This process (spatulation) is repeated until the mixture is fully mixed into a homogenous mix of uniform color with no marbling, or individual streaks of the colors or the individual components. Then, the assistant uses the spatula to place the mixture in the triple tray.
If a very sticky impression material is used, such as polyether, the assistant should press the spatula downward into the impression material when mixing it, and avoid pulling the spatula off the impression material, a movement which can lift up the mixing pad. Also, the assistant should only use downward pressure when putting the impression material onto the triple tray. The triple tray is loaded by moving the spatula in a downward direction with the mass of impression material in the spatula being in contact with the triple tray, while simultaneously moving the triple tray in a single sideways direction across the edge of the spatula.
An impression gun with the applicable plastic mixing tip mixes impression material more accurately than hand spatulation. An impression gun has a disposable plastic cartridge with two tubes that hold the base and catalyst. This cartridge is locked into the impression gun, which, when the gun handle is squeezed, pushes two rods into the disposable plastic cartridge. These rods push the impression material out of the end of the cartridge, and into a disposable, spiral-tube mixing tip that is attached to the cartridge. The two ingredients emerge perfectly mixed from the tip’s lumen.
Spiral Mixing Tips
Each type of VPS cartridge may have its own type of spiral mixing tip attachment. Different tips are color-coded for different types of impression materials. Using the wrong tip may result in the incomplete mixture as it exits from the spiral mixing tip. The assistant should know which materials require which specified tips and monitor when the office is running low on stock of a required mixing tip.
An automatic mixing machine, like a Pentamix™machine, has a plastic, disposable, spiral mixing tip that is different in shape (shorter and wider) compared to the thinner, longer, spiral mixing tip of an impression gun. Also, some composite materials that are used to make temporary restorations, come in a cartridge that attaches to their own impression gun (different from a VPS gun) and uses their own spiral mixing tip.
Obtaining the Preoperative Triple Tray Impression
The initial, triple tray preoperative impression is made by placing medium viscosity VPS (or monophase or medium viscosity polyether) on the triple tray, while ensuring that the impression-gripping spokes on the short sides of the tray are completely filled with impression material. In the authors’ experience, it is not necessary to place an adhesive for the impression material in the triple tray. The spokes on the side of the tray, and the many tiny holes in the triple tray mesh, assure that the triple tray impression interlocks onto itself with mechanical retention, so that no adhesive is required.
The assistant positions the tray by aligning the curvature of the mesh surface of the tray with the curvature of the patient’s arch, such that essentially the patient occludes into the center of the mesh. For posterior triple trays, the posterior plastic loop of the tray should be placed distal to the most distal posterior teeth of the arch, such that the distal loop of the tray goes behind the teeth. Ideally, there should be no interference of the teeth, the maxillary tuberosity, or the retromolar pad into the distal loop of the tray.25-28
Sometimes, however, it may be unavoidable that the posterior teeth occlude into the loop, such as if there is an impacted third molar in the area. However, after obtaining hundreds of triple tray impressions, the authors find that crowns usually fit perfectly even if there is some soft tissue or tooth impingement into the distal loop of the triple tray. The stiffness of the impression material seems to overcome tiny amounts of flexure of the plastic tray itself, and a dental laboratory technician can usually detect and correct an incorrect triple tray articulation. Of course, the dentist will exercise their best judgment regarding this potential source of error if indicated and a new impression may need to be taken on the patient.
Prior to placing the triple tray, the assistant will check the patient’s natural occlusion to verify how the patient’s teeth occlude in maximum intercuspation. When the triple tray is in the mouth, the assistant makes sure that the patient is occluding into the same maximum intercuspation as verified during the initial check.29 If the patient is shifting the bite when occluding into the tray, the assistant can instruct the patient to “bite on the back teeth,” a command which often causes the patient to bite into their natural and proper maximum intercuspation position.
After making an anterior preoperative triple tray impression, the assistant rinses the tray in water to remove saliva, blood, and other protein material. The assistant will identify the midline between teeth No. 8 and No. 9 in the maxillary impression. The assistant then drills, into the plastic rim of tray, an orientation notch that originates at that midline and extends about 3-5 mm. in length (Figure 4). This orientation notch indicates which side of the tray is the maxillary side, and references the anterior midline point on the tray. After the tooth preparation, when the assistant places low viscosity impression material in both sides of the anterior tray to reline the preoperative impression, the low-viscosity impression material may cover up all of the anterior teeth. The orientation notch aids the assistant in proper orientation and eliminates later confusion and possible misalignment of the midline for making the reline impression. Misalignment of the tray or placing the reline impression upside down, can ruin the impression and require a remake of the impression, using a new triple tray.
With a posterior triple tray, the orientation mark is less necessary because the tray curvature follows the curvature of the arch, making tray positioning more clear. Also, an imprint in the preoperative impression of a maxillary anterior tooth, which need not be covered by reline impression material that is placed in the posterior aspect of the tray, is easy to distinguish from an imprint of the thin mandibular incisors.
Introduction to Provisional Restorations
After the preoperative impression has been obtained and the dentist has prepared the abutment tooth/teeth, the assistant (if the state practice act permits) makes a/the provisional restoration(s). While the permanent restoration is being fabricated, the temporary restoration protects the tooth while maintaining the interproximal contacts and occlusion. Without a temporary restoration, the prepared teeth may become sensitive and the neighboring teeth may shift toward the abutment tooth in the time it takes for a laboratory to make the final crown or bridge. Also, without a firm occlusal contact, the opposing teeth that occlude in the arch may unnecessarily extrude toward each other. This shifting may result in the final crown requiring extensive adjustment to fit onto the abutment tooth during crown delivery, or even require a remake of the crown.15,30-33
There are various techniques for making provisional restorations described in dental literature.15,30-33 Before mixing the acrylic, the assistant chooses an appropriate shade of the acrylic powder. The brightest shade is shade B-1, but usually less bright shades like A-1 or A-2 are used. A shade of acrylic that is too bright appears to stand out more than a shade that is too dark. In each circumstance, the assistant and dentist should use their best judgment to choose the best shade of acrylic for the provisional.
Modifying the Preoperative Impression Prior to the Fabrication of the Provisional Restoration
In some cases, the preoperative impression requires modification before the provisional restoration can be fabricated. The provisional restoration must have contact with the teeth next to the abutment tooth. If, in the preoperative impression, there is a wall of impression material between the abutment tooth and the neighboring tooth, a hemostat or scalpel should be used to remove the excess impression material, which allows the liquid temporary mixture to flow into contact with the adjacent tooth.
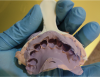
Sometimes, while making the preoperative impression, impression material can flow into tooth or oral undercuts, in the tuberosity areas, or under pontics of existing bridges in the patient’s mouth. This material may prevent the patient from fully occluding into the preoperative impression (Figure 5). The assistant should try in the preoperative impression prior to making the provisional restoration, ensuring that the patient can completely occlude again. The assistant should cut away any obstructions using scissors or a scalpel (Figure 6). In general, undercut areas within tooth structure, excess impression material that flowed under bridge pontic(s), or long protrusions of impression material in the posterior lingual area should be cut away until the patient can close completely into the preoperative impression.
When making a provisional bridge, the assistant should cut away the edentulous ridge between the abutment teeth, using a scalpel (Figure 7 and Figure 8). The assistant should remove a trapazoid-shaped section of the impression material between the abutment teeth, level with the occlusal aspect of the abutment teeth. The buccal-lingual width of the cut-out portion should be approximately the same as the buccal-lingual width of the abutment teeth. The buccal and lingual walls of the cut-out portion should flare slightly in the preoperative impression, so that it is not undercut, since undercutting this area would make the provisional restoration lock into the preoperative impression.
Additionally, lubrication is not indicated in the preoperative impression, since in general temporary material is easy to remove even from a dry preoperative impression. Applied lubrication can form a film on the preoperative impression material that may make it difficult for the reline impression material to bond to the preoperative impression when the final reline impression is obtained.
By moving the material on and off the abutment repeatedly while the material is setting, lock-on problems are prevented. Lubrication is not necessary to prevent the provisional material from locking onto the abutment as the patient’s own saliva provides all the lubrication needed.
Composite vs. Acrylic Temporary Restoration Materials
Some temporary restoration material, such a self-cure composite material, is mixed automatically. The material comes in a dispenser that contains the base and catalyst ingredients. This is attached to a dispensing gun, and extruded through a spiral mixing tip.34 The assistant points the tip into the voided area in the preoperative impression that corresponds to the abutment tooth and fills the void, thus creating the provisional.
Another type of temporary restoration material is acrylic resin and consists of powder and liquid monomer ingredients which are hand-mixed using a cement spatula. One to two cubic cm of the powder is dispensed into a dappen dish. Using an eye-dropper, the monomer liquid is placed into the powder. Enough liquid is added to create a thick, barely viscous, but not visibly powdery, acrylic/monomer mixture. This mixture is then spatulated into the abutment tooth void in the preoperative impression.
Some mix acrylic resin material directly in the void in the preoperative impression of the unprepared tooth, instead of using a separate mixing container. The void is filled with acrylic powder and then liquid drops of the acrylic monomer is incorporated into the powder while mixing it with a thin rod. It is advised not to mix the acrylic directly in the impression void because the uneven surfaces of impressions of teeth in the impression make it difficult to homogeneously mix the acrylic. Unmixed acrylic powder may remain in the void, resulting in a stiffer mix of acrylic that the patient cannot fully occlude into, and also will not flow enough to create a smooth, detailed, porosity-free temporary restoration.
A flexible, silicone dappen dish is perhaps the best container to use for mixing the acrylic/monomer mixture, since the hardened mixture can easily be removed from the container by flexing it, and the container is reusable and sterilizable. A silicone container also has a stable, non-slip base (versus plastic disposable dappen dishes that can slip while mixing impression material inside them).
If the material is mixed in a glass dappen dish, immediately clean out any excess, soft acrylic mixture from the dish using gauze. Immediately dispose of the gauze and the gloves that were used while wiping the dish, to prevent monomer from penetrating the gloves and contacting the skin. Gauze moistened with alcohol efficiently cleans hardened acrylic material from a silicone dappen dish.
The Preoperative Impression Technique for Fabricating a Temporary Restoration
A temporary fabrication technique is easily accomplished by filling the impression of the unprepared tooth, in the preoperative triple tray impression, with one of the aforementioned mixtures of impression material. The now filled, preoperative triple tray impression is replaced over the preparation(s), and the patient is instructed to bite down. The soft impression material is molded by the preoperative impression and formed into a tooth that has the same shape as the original tooth of the preoperative impression. The soft material then self-polymerizes into a hard temporary tooth after a few minutes.
Unsupervised vs. Supervised Setting of Acrylic
Another technique has the (initially soft) temporary material completely polymerize into a hard temporary crown in the patient’s mouth while the patient is occluding into the triple tray. This approach is not recommended. The dentist may have prepared the abutment(s) with undercuts or divots in the abutment(s) (Figure 9). An undercut is basically an axially directed indentation in the body of the abutment. It may be so small as to be microscopic, but if a hard temporary material infiltrates into it, the temporary crown may lock into it. It may be impossible to remove the temporary without cutting it off and starting over, which wastes chairside time. Also, if the dentist is making bridge abutments, the bridge abutments may not be fully aligned with one another and a hard plastic bridge made for the abutments may lock onto the abutments. Secondly, even if the abutment(s) are free of undercuts, temporary material can infiltrate into the interproximal areas between the abutment teeth and the adjacent teeth (Figure 10). When the temporary material hardens, the crown may be locked into the neighboring teeth. Thirdly, a temporary restoration that sets while inside the impression may set too high in the occlusion. Later, it can be time-consuming to grind down the temporary tooth to adjust the occlusion.
The Custom Technique for Making Temporary Restorations
A temporary crown should be made using a non-shrinking acrylic material that takes several minutes to harden, and can be actively adjusted while the temporary restoration is setting.
Here, the soft temporary material is placed in the triple tray, seated intraorally, and stays in place for approximately 2-3 minutes. The triple tray is then removed while the temporary material is still soft and rubbery. The temporary material often remains in the tray during tray removal. The assistant will wait until the temporary crown has polymerized enough to have adequate tensile strength to be removed from the preoperative impression without damage using cotton pliers.
At this point, fine scissors are used to trim away excess material that invaded the interproximal and marginal spaces (Figure 10). These interproximal “corners” of acrylic often cause the temporary restoration to lock into the adjacent tooth. Excess amounts of temporary material that flow past the margins of the provisional must also be removed while still maintaining the contact points and occlusion (Figure 11).
The pliable temporary crown is seated and the patient is instructed to bite. At this point the temporary tooth has some flexibility, but also some tensile strength. Occluding the arches while the temporary crown is still soft instantly sets the occlusion level of the temporary crown. The pliable provisional is removed and quickly reseated onto the abutment. While actively repeating the removal and reseating the crown, the patient should bite down into occlusion to ensure proper occlusion is still there. The occlusion could distort due to flexing the soft provisional while removing it and reseating it, and also due to shrinkage of the provisional crown while it is polymerizing. Removing and reseating the crown repeatedly until the crown is set hard allows the provisional to rub against any undercuts that may be in the abutments. This shapes the inner surface of the provisional so that it glides over the undercuts, instead of locking into the undercuts, which would happen if the provisional was just left on the abutment to polymerize completely. Moving the provisional on and off the abutment repeatedly will also prevent any acrylic shrinkage from causing the provisional to harden into something that is too tight to fit the abutment.
The Shell Technique for Making Temporary Restorations
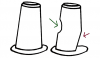
Sometimes a shell technique is used to make provisionals. Here, a crown form is chosen that is the approximate size for the abutment. The crown form is filled with the chosen provisional material and placed on the abutment. One disadvantage with this method is that the plastic crown form may be too big, which prevents the patient from occluding into the crown form to directly set the occlusion of the provisional restoration while the acrylic is setting. When the shell does not fit well, trimming the cervical margins and try-ins are necessary prior to placement. Later, it can be time-consuming to adjust the occlusion of the shell-made provisional restoration.
The Bulk Technique for Making Temporary Restorations
A provisional may need to be made without the use of a preoperative impression as a mold. For example, a patient may present for a crown preparation where the original crown was lost or the original tooth structure is severely compromised. In this situation, a bulk mix of temporary material is placed on the abutment and the provisional is made from scratch.
To make a bulk provisional, the temporary material is mixed as before. When the material has polymerized into a soft, but slightly stiff dough texture, it is placed on the abutment and compressed into the tooth by “pinching” it using gloved fingers. The thumb and middle fingers pinch the temporary mass from the buccal and lingual aspects, while the index finger simultaneously pushes the mass apically into the abutment from the occlusal aspect. The adjacent teeth help to box the material in on the mesial and distal aspects of the abutment. The purpose of the pinch technique is to make the temporary cover and encircle the entire abutment, so that the intaglio surface of the mass is well-defined, with a sharp circular margin.
As with the custom technique, the patient is instructed to bite into the mass to set the occlusion. After the patient opens again, the temporary mass is lightly pinched and then the patient occludes into it again. It is then removed from the abutment while it is still soft, and scissors are used to cut away the gross acrylic excess to the margin of the provisional, and to cut away the corners of the temporary tooth that can lock into interproximal spaces between the abutment and neighboring teeth. The still-soft temporary mass is reseated on the abutment, and then repeatedly moved up and down on the abutment, while at times pinching the mass into the abutment lightly to maintain its shape while it is forming, and having the patient occlude onto the provisional to ensure that the occlusion is still present, until the mass has hardened completely.
After the provisional has hardened, the unrefined and unpolished provisional is set aside. The dentist takes the final reline impression of the abutment. While the dentist is making the final impression, the bulk provisional is refined.
Refining and Polishing the Provisional Restoration
An initial provisional, when it first emerges from the mold, should only require a few minutes of minor adjustments before the refined provisional is completed. If the initial provisional is distorted from being locked onto a tooth, or has large porosities or defects, it may be more efficient to start over than to try to correct a grossly malformed temporary restoration.
Sometimes, the provisional has voids or marginal deficiencies that must be filled with more temporary material. In general, to add temporary material to a provisional, temporary material is mixed until the material is somewhat thick but completely moist and smooth, with no powder in the mixture. A small amount of the material is then added into the gap or void, with a small excess, that can be polished away later. After the temporary material has set to the point where it is not liquid-like, a wet, gloved finger is used to smooth the temporary material against the provisional. The temporary is moved up and down over the abutment to prevent the added material from locking into the abutment.
If an anterior provisional features a rough anterior surface, the entire face of each rough tooth should have extra material added. The material should be smoothed with a wet, gloved finger, and then the edge of the spatula is utilized to scrape temporary material away from the embrasure and interproximal spaces between the teeth. In general, the most efficient way to contour the facial surface of the anterior tooth is to shape and smooth it as perfectly as possible while the material is still soft, and while preserving all margins between provisionals, to minimize the difficulty of refining the shape after the provisionals have hardened.
A hand-held, straight nose-cone handpiece and a set of polishing burs should be used to achieve coarse and fine polishing of the provisional. Another option is to use a large lab bur on a dental lathe (Figure 12 and Figure 13). The provisional should be smooth and the margins should be flush with the margins of the abutment. It should be in occlusion, neither too high nor too low, and should have contact with the interproximal surfaces of the adjacent teeth. The provisional is then polished into a glossy finish. This is completed using a wet rag wheel with an incorporated fine pumice, or by using acrylic finishing and polishing burs, with different degrees of polish fineness from one bur to another (Figure 12). High-magnification (4-6 x) loupes worn by the operator help in detecting rough areas on the provisional restoration.
The dentist, or the assistant (depending on the state’s dental law and mastered skill set), adjusts the occlusion on the temporary by using articulating paper and a round diamond bur to trim away excess occlusal material. Drying the provisional before asking the patient to bite on the articulating paper helps ensure accurate marks. The operator may use direct and indirect vision to directly see where the high spot on the provisional is located. The use of 4-6 x magnification loupes and operatory lighting aid in this direct visual observation.
Relining a Triple Tray Impression
To make a final reline impression, the assistant places low-viscosity VPS in the preoperative impression, and completely covers the teeth on both sides of the impression. The assistant then immediately hands the triple tray to the dentist, who places the tray intraorally over the previously dried teeth. The patient then occludes into the tray until the material sets.
The reline impression material should be placed onto the abutment teeth, but it is advised to place the material onto all of the teeth in both arches of the tray. Placing the material only on the abutment teeth may distort the occlusion on the abutment teeth, making the abutments too elevated on the model that will be made from the impression. If all of the teeth in both arches are covered, any such elevation will elevate all of the teeth simultaneously. The trained dental laboratory technician can properly hand-articulate the models to obtain an accurate bite if the teeth are evenly elevated.
Preparations Prior to Obtaining the Reline Impression
Prior to filling the initial triple tray impression to reline it, the assistant would have already ensured that the patient could close completely into the tray when creating the provisional. The impression material within the tray would have already been trimmed as needed to remove closure obstructions. Also, prior to making the final impression, cord may need to be packed in the sulcus around the abutment. The cord is removed before the final reline impression is taken to ensure adequate exposure of the abutment margin.
Obtaining the Impression
After the dentist places the triple tray with the reline material in the mouth, the patient should occlude into the tray until the excess, leftover impression material on the pad has set hard. The dentist then removes the impression, and it is rinsed under tap water to remove blood and saliva and then dried using an air-water syringe. (All personal protective equipment (PPE) is worn during chairside procedures. Rinsing both sides of the impression ensures that there are minimal amounts of potentially infectious materials in the impression, to help prevent infectious material from being blown around the operatory when the assistant air dries the impression.)
The dentist must examine the impression of the abutment teeth to ensure that the impression has captured all details, without air bubbles, gaps, delamination of the impression material, pulling of impression material, distortions of the margins, etc.1 Ideally, the impression is accurate enough to capture tiny streaks and scratches on the abutment surface made by the diamond bur that the dentist uses to prepare the abutment (Figure 14).
If the impression is inaccurate or defective, another reline impression may be required. Prior to the dentist making the second reline, the assistant will carefully remove and trim the previous material from triple tray impression as needed to ensure that the patient can occlude fully into it.
Obtaining a Bite Registration
After making the triple tray reline impression, a separate bite registration may be needed. A bite registration is a separate impression that uses just a bite registration material, and no tray, to capture an impression of how the patient’s jaws occlude (an interocclusal record.)36 A separate bite registration is required if the occlusion between the two arches is not obvious when observing how the unprepared teeth that are captured in the triple tray impression occlude with one another. Many dentists prefer to use VPS, instead of less accurate wax, as a bite registration material for high-precision crown and bridge procedures.
VPS bite registration material comes in a plastic cartridge that is locked into an impression gun. The assistant attaches a spiral mixing tip to the cartridge and dries the patient’s teeth. The VPS is placed on the most posterior mandibular tooth on one side of the arch, and then, in a continuous movement, the assistant dispenses a continuous ribbon of VPS around the arch to the most posterior tooth on the other side. The patient occludes into the VPS and continues to occlude until the VPS sets. Bite registration VPS sets in either thirty seconds or two minutes. The fastest set is preferred since this assures that the VPS will fully set and not be removed before it has completely polymerized. This requires fast work and coordination to dispense the material and completely seat over the teeth while the VPS is still soft enough for the patient to occlude completely into it.
Some patients will be edentulous on one side of the patient’s arch. In this situation the VPS will need to be built up between the opposing maxillary and mandibular edentulous areas, to capture the vertical relationship between the ridges at various points along the arches.
Impression for a Full-Arch Round-House Crown and Bridge Case
If a dentist is making a round-house bridge that involves an entire arch of teeth, separate arch impressions must be used. For full arch cases, if most of the patient’s anterior teeth exist before the bridge teeth are prepared, a separate preoperative impression of the unprepared teeth should be made and sent to the laboratory (Figure 15). The laboratory will use this to make a model to use as a reference for replication of the anterior teeth before tooth preparation, and to show the vertical dimension of the patient’s dentition in occlusion.
In addition, an impression of the facial surfaces of the unprepared anterior teeth can be made to show their original shape and relationship. The patient will occlude and fast-setting bite registration material will be placed on the facial surfaces of both the mandibular and maxillary anterior teeth (Figure 15). When the impression material has reached a tacky set, the assistant lightly uses fingers to press the impression material into the teeth to ensure the infiltration of the impression material. This shows the relationship of the maxillary midline to the mandibular midline, and the measurement of any existing overjet.
If a dentist is performing a round-house bridge on a patient, obtaining a bite registration can be challenging. When all of the teeth are prepared, there may be no normal occlusion due to all teeth prepped into abutment form. Here, the dentist may want to prepare all of the abutment teeth except for one tooth that is in occlusion and makes the jaws stop at a fixed and reproducible point in space. Then, a bite registration is taken by placing VPS on the abutment teeth and the edentulous ridge segments between them and having the patient occlude using the one unprepared tooth, such that the bite registration material contacts and connects the surfaces of the two arches. After this bite registration has been obtained, the dentist prepares the last remaining tooth. The dental laboratory technician can articulate the casts by using the bite registration that articulates on all of the abutments except the one that was not yet prepared when the bite registration was made.
Cementing the Provisional Restoration
Dentists often use a eugenol-based temporary cement to cement provisional restorations. This allows for relatively easy removal of the provisional at the try-in appointment. This cement is dispensed with a 50-50 ratio of base and catalyst onto a mixing pad. The cement is placed into the provisional and swirled around until the intaglio surface is completely coated with cement. The prepared tooth is dried, the provisional is seated onto the tooth. The patient is instructed to bite and hold the provisional in place. This ensures that the occlusion sets perfectly as cementation occurs. A drawback to note is that the eugenol oils can react with the acrylic, making it difficult, if not impossible, to further reline the provisional.
Carboxylate cement is stronger than eugenol-based cement and bonds weakly to the tooth itself. Unmixed, two-part carboxylate cement starts as a powder and liquid. The mixed cement can be thick and opaque, or slightly tacky.37 Use of a thicker and tacky mix of a strong cement such as carboxylate helps to fill in small voids under the intaglio surface of the temporary restoration. Provisionals cemented with carboxylate cement are less likely to disengage with the tooth compared to those cemented with eugenol-based cement, even if there are small marginal voids in the temporary restoration. On the day of final insertion, a handpiece with a bur may be needed to cut off the temporary restoration, followed by an ultrasonic scaler to efficiently remove carboxylate cement from the abutment(s).
To remove excess cement during initial placement, a cotton roll is used to wipe away excess cement while the cement is still liquid. Floss is used in the interproximal spaces around the provisional to remove interproximal excess. The tip of an explorer or floss is passed under bridge pontics to remove excess cement from underneath the pontics. After the cement has attained a somewhat hard but brittle set, an explorer may be used to carefully remove excess cement from the margins without making contact with sensitive gingival tissues. The interproximal cement is removed by pushing an explorer tip into the interface between the cement and the provisional and moving the tip in an apical and lateral movement to dislodge the cement. An ultrasonic scaler may also be used to remove excess hardened cement. The patient is instructed not to eat using the provisional(s) for two hours while the cement fully cures.
Writing Dental Laboratory Prescriptions and Packaging the Case
A laboratory prescription slip contains written instructions from the dentist to the dental laboratory technologist (DLT). The instructions state details and expectations about what to fabricate using the enclosed impression and other materials. The dentist will complete the laboratory script or dictate the exact details to the dental assistant for inclusion. The tooth shade(s) of the crown or bridge, and the type of shade guide used to obtain the shade, should be indicated on the laboratory slip along with additional details such as metal work and porcelain coverage. Different shades will be compared and the patient may be consulted on the chosen shade(s).
The laboratory prescription slip will contain the dentist’s name and contact information. The start date of treatment and the required due date of return will be written on the slip. The treating dentist will review all of the information and instructions involved, and sign the laboratory slip.
If a DLT personally picks up the office laboratory cases, the case may be placed in a small bag or box. A few crumpled paper towels may be placed in the container for cushioning and to absorb moisture, and the case items are placed over this. The dentist may also mail the case to a lab outside the area. The case items are packaged in a small box with foam cushioning, so that the materials are not compressed but also do not move inside the box. The box will be secured according to standard mailing instructions. Materials from different cases should never be packed in the same container. A note describing the disinfecting procedures must be included in the packaging to notify the DLT working on the case.
Summary
When assisted by an educated and skilled dental assistant, a dentist performing triple tray procedures may only need to anesthetize the patient, prepare the crown and/or bridge abutment(s), and complete final checks before patient dismissal. The assistant, depending on what tasks can be legally delegated under the dentist’s supervision, can complete several supporting tasks during crown and bridge restorative appointments. Although in the future, computer-based crown and bridge procedures38-40 may supplant various aspects of the manual triple tray technique, the efficiency of the manual technique may ensure its continued use.
Glossary
Abutment - a tooth that is shaped, via drilling, into a support for a crown; the crown will later be cemented permanently onto the abutment, which is also called a "preparation."
Counter-model impression - an impression of the opposing arch; this arch does not contain the tooth that is being prepared into a crown abutment
Dappen dish - a tiny bowl/cup used for mixing acrylic material when making temporary restorations
Hydrophilic - attracted to moisture
Hydrophobic - repelled by moisture
Intaglio surface - the inside surface of a crown
Loupes - special magnification glasses that aid in seeing small, fine details
Maximum intercuspation - a jaw position where a patient’s teeth mesh perfectly together, with opposing wear facets touching one another; a patient’s normal bite position where there are no ob- structions to separate the teeth from fully meshing together
Maxillary tuberosity - the most distal ends of the maxillary arch; the “knob” of gingiva located distal to the maxillary third molar areas
Monophase - an impression material that does not come in different viscosities like high viscosity, low viscosity or medium viscosity, but instead only comes with one viscosity
Polyether - a type of impression material that is naturally hydrophilic; accurate enough to be used for crown and bridge impressions; very sticky when mixed and sets into a stiff but somewhat flexible impression material
Pontic - the artificial crown tooth that is fused between two abutments to bridge the gap between the two abutments, thereby creating a bridge
Preparation - a pattern cut into a tooth to prepare the tooth to accept a restoration. In crown and bridge, a preparation, also known as an abutment, is a tooth that is shaped such that a crown can be made to fit over it.
Retromolar pad - the areas of gingiva located distally to the mandibular third molar area in the mandibular arch
Round-house crown and bridge case - a crown and bridge case where all (or most) teeth across an entire arch, from left to right, are prepared for crowns and bridges; after preparing the teeth into abutments, there may be no unprepared teeth left to clearly show what the occlusion was like before the teeth were prepared
Stock impression tray - an impression tray that is of a generic shape, often made of stiff plastic, coming in sizes of small, medium and large
Vinyl polysiloxane - a type of impression material that is accurate enough to be used for crown and bridge impressions; modern formulations of VPS allow VPS to be moderately hydrophilic; also known as poly vinylsiloxane
Viscosity - a measure of the amount of flow of an impression material; low viscosity material flows into tinier crevices compared to a high viscosity material
References
1. Wilson EG, Werrin SR Double arch impression for simplified restorative dentistry. J Prosthet Dent. 1983;49(2):198-202.
2. Cox JR, Brandt RL, Hughes HJ. The double arch impression technique: a solution to prevent supraocclusion in the indirect restoration. Gen Dent. 2000;January-February:86-91.
3. Christensen G. A new simple double arch impression tray. Clin Res Assoc News. 5:4, 1981.
4. Thongthammachat S, Moore BK, Barco MT 2nd, Hovijitra S, Brown DT, Andres CJ. Dimensional accuracy of dental casts: influence of tray material, impression material, and time. J Prosthodont. 2002;11(2):98-108.
5. Johnson GH, Mancl LA, Schwedhelm ER, Verhoef DR, Lepe X. Clinical trial investigating success rates for polyether and vinyl polysiloxane impressions made with full-arch and dual-arch plastic trays. J Prosthet Dent. 2010;103(1):13-22.
6. Small BW. Revisiting impressions using dual-arch trays. Gen Dent. 2012;60(5):379-381.
7. Davis R, Schwartz, Hilton T. Marginal adaptation of castings made with dual-arch and custom trays. Am J Dent. 1992;5(5):253-254.
8. Breeding LC, Dixon DL. Accuracy of casts generated from dual-arch impressions. J Prosthet Dent. 2000;84(4):403-407.
9. Lane DA, Randall RC, Lane NS, Wilson NH. A clinical trial to compare double-arch and complete-arch impression techniques in the provision of indirect restorations. J Prosthet Dent. 2003;89(2):141-145.
10. Cox JR, Brandt RL, Hughes HJ. A clinical pilot study of the dimensional accuracy of double-arch and complete-arch impressions. J Prosthet Dent. 2002;87(5):510-515.
11. Davis RD, Schwartz RS. Dual-arch and custom tray impression accuracy. Am J Dent.1991;4(2):89-92.
12. Pesun IJ, Swain VL. Three-way trays: easy to use and abuse. J Can Dent Assoc. 2008;74(10):907-911.
13. Ceyhan JA, Johnson GH, Lepe X. The effect of tray selection, viscosity of impression material, and sequence of pour on the accuracy of dies made from dual-arch impressions. J Prosthet Dent. 2003; 90(2):143-149.
14. Schoenrock G. The laminar impression technique. J Prosthet Dent. 1989;62:392-395.
15. Shillingburg HT, Jacobi R, Brackett S, Hobo S, Whitsett LD. Fundamentals of fixed prosthodontics. 3rd ed. Chicago: Quintessence Publishing; 1997.
16. Rupp F, Geis-Gerstorfer J. Hydrophilicity of unset and set elastomeric impression materials. Int J Prosthodont. 2010;23(6):552-554.
17. German MJ, Carrick TE, McCabe JF. Surface detail reproduction of elastomeric impression materials related to rheological properties. Dent Mater. 2008;24(7):951-956.
18. Hammond BD, Myers ML, Haywood VB. A quadrant tray and bite registration as an alternative to dual-arch impressions for fixed prosthetics: a clinical and dental laboratory technique. Gen Dent. 2011;59(5):350-354.
19. Faria AC, Rodrigues RC, Macedo AP, Mattos Mda G, Ribeiro RF. Accuracy of stone casts obtained by different impression materials. Braz Oral Res. 2008;22(4):293-298.
20. Nassar U, Hussein B, Oko A, Carey JP, Flores-Mir C. Dimensional accuracy of 2 irreversible hydrocolloid alternative impression materials with immediate and delayed pouring. J Can Dent. Assoc. 2012;78:c2.
21. Wassell RW, Walls AW, Steele JG. Crowns and extra-coronal restorations: materials selection. Br Dent J. 2002;192(4):199-202, 205-211.
22. Endo T, Finger WJ. Dimensional accuracy of a new polyether impression material. Quintessence Int. 2006;37(1):47-51.
23. Di Felice R, Scotti R, Belser UC. The influence of the mixing technique on the content of voids in two polyether impression materials. Schweiz Monatsschr Zahnmed. 2002;112(1):12-16.
24. Kugel G, Swift EJ Jr, Sorensen JA, Tucker JH, Dunne JT Jr. A prospective clinical evaluation of electronically mixed polyvinyl siloxane impression materials: results from the prosthetic “SuperStudy”--a consumer evaluation. Compend Contin Educ Dent Suppl. 1999;(24):S3-21.
25. Carrotte PV, Johnson A, Winstanley RB. The influence of the impression tray on the accuracy of impressions for crown and bridge work-an investigation and review. Br Dent J. 1998;185:580-585.
26. Thornton LJ. A survey of disposable articulators. Gen Dent. 2002;50(1):72-76.
27. Hoos JC, Kaplowitz GJ. Proper placement of dual-arch impression trays. J Am Dent Assoc. 2003;134(6):729-730.
28. Larson TD, Nielsen MA, Brackett WW. The accuracy of dual-arch impressions: a pilot study. J Prosthet Dent. 2002;87(6):625-627.
29. Keesee SM, Cameron SM, Lefler TB. Fabricating a simple closure guide for the dual-arch impression technique. J Prosthet Dent. 2001;85(4):418.
30. Wassell RW, St George G, Ingledew RP, Steele JG. Crowns and other extra-coronal restorations: provisional restorations. Br Dent J. 2002;192(11):619-622, 625-630.
31. Rosenstiel SF, Land MF, Fujimoto J. Contemporary Fixed Prosthodontics. 4th edition. Mosby; 2006.
32. Lowe RA. Predictable fixed prosthodontics: technique is the key to success. Compend Contin Educ Dent. 2002;23(3 suppl 1):4-12.
33. Rossein K. Provisionalization: the key to cosmetic & restorative success. Compend Contin Educ Dent. 1995;16(7):684, 686, 688 passim.
34. Cutbirth ST. Provisionalization for porcelain veneers using bis-acrylate and polyvinylsiloxane matrix. Pract Periodontics Aesthet Dent. 2000;12(3):308-312.
35. Walker MP, Rondeau M, Petrie C, Tasca A, Williams K. Surface quality and long-term dimensional stability of current elastomeric impression materials after disinfection. J Prosthodont. 2007;16(5):343-351.
36. Boksman L. Optimizing occlusal results for crown and bridge prostheses. Dent Today. 2011;30(1):154, 156-157.
37. Behr M, Rosentritt M, Loher H, Kolbeck C, Trempler C, Stemplinger B, Kopzon V, Handel G. Changes of cement properties caused by mixing errors: the therapeutic range of different cement types. Dent Mater. 2008;24(9):1187-1193.
38. van der Meer WJ, Andriessen FS, Wismeijer D, Ren Y. Application of intra-oral dental scanners in the digital workflow of implantology. PLoS One. 2012;7(8):e43312.
39. Kachalia PR, Geissberger MJ. Dentistry a la carte: in-office CAD/CAM technology. J Calif Dent Assoc. 2010;38(5):323-330.
40. Kassem AS, Atta O, El-Mowafy O. Fatigue resistance and microleakage of CAD/CAM ceramic and composite molar crowns. J Prosthodont. 2012;21(1):28-32.
About the Authors
John S. Mamoun, DMD
John S. Mamoun, DMD, is a 2003 graduate of the University of Medicine and Dentistry of New Jersey (now the Rutgers School of Dental Medicine). He completed a one–year Advanced Education in General Dentistry residency at the Eastman Dental Center, in Rochester, NY, and in 2006 earned his Fellowship award from the Academy of General Dentistry. He has published over 30 articles in dental journals, and is currently in private practice in Manalapan, NJ.
Mariam Javaid, BDS
Mariam Javaid, BDS, graduated from the Altamash Institute of Dental Medicine (AIDM) in 2009, in Pakistan. After completing a residency at the AlDM in 2010, and an externship at the Karolinska Institute in Stockholm, Sweden, she came to the United States. She then graduated from the University of Pennsylvania School of Dental Medicine in Philadelphia, PA, and is now a pediatric dentistry resident at Holyoke Health Center.