You must be signed in to read the rest of this article.
Registration on CDEWorld is free. Sign up today!
Forgot your password? Click Here!
There have been many well-established reports regarding the education of oral healthcare providers within educational institutions.1,2 One most notable report in 2003 from the American Dental Education Association’s (ADEA) President’s Commission details the roles and responsibilities of academic dental institutions.3 In that report, authors draw attention to the significance educational institutions have in becoming part of the “moral community,” helping not only improve access to oral healthcare, but to “be able to influence state and federal policy makers, community leaders, industry, and other stakeholders to help the profession fulfill its moral duties.”3 A critical concern in this ADEA report was meeting the oral healthcare needs of our changing demographic society, including underserved and culturally diverse populations.
The Surgeon General’s Healthy People 2020 report noted the impact of oral health on general health, disparities in oral health, and access to care within the low-income and underserved.4 For example, a higher percentage of diverse populations have been shown to have a greater incidence of dental/oral disease. Therefore, the Surgeon General outlined the substantial benefits of including oral health in the design of community programming.3,4 It has also been suggested that without substantial change in dental and dental hygiene education models of oral care, dentistry as a profession will only reproduce rather than address and change the current landscape of oral health disparities.5
The Commission on Dental Accreditation (CODA) standards clearly identify that students graduating from dental/dental hygiene institutions must be competent in managing a diverse patient population and have the interpersonal and communication skills to function successfully in multi-cultural work environments (Standard 2.17), and that they are competent in assessing the treatment needs of patients with special needs, (Standard 2.12).6 Therefore, if educators implement strategies to expose students to diverse patient populations, those students may view working with these patients as a rewarding experience and be better prepared to treat them in the workforce.
Legislators are turning to alternative delivery systems to address the oral healthcare needs of underserved populations. Several midlevel provider models have been described and suggested such as the advanced dental hygiene practitioner (ADHP), the community dental health coordinator (CDHC), and the dental health aid therapist (DHAT).7 These models have been proposed at a national level; however, individual states are also working on models specific to their needs. For example, the state of Kansas has addressed access to oral healthcare through the enactment of the Extended Care Permit (ECP) Dental Hygienist and, to date, has in place the ECP I, II, and III.8
In order to prepare students for working with a diverse population upon graduation, it is critical that they are exposed to and know how to treat those from diverse backgrounds and who have diverse oral health needs and/or disabilities. The literature suggests the best way for students to grasp the importance of community service and to gain a sense of cultural competency is through the implementation of service-learning opportunities. Yoder states that “integrating service-learning into dental curriculum will create a deeper understanding of the dynamics, the assets, and the challenges of the community and its relationship to oral and general health.”9
Service learning is not simply providing services to the community or volunteer work. To be authentic service learning, there must be a reciprocal component, preparation, and reflection.9,10 The services provided are in response to a community need and work with and enhance the students’ course goals and objectives and their roles as professionals and community partners.9,11 Yoder outlines critical components for the planning, implementation, and evaluation of service learning in dental curriculum that are needed to be authentic service learning and not just community engagement.9
Three main goals of service learning used in dental educational settings have also been described by Hood.12 Improving student learning, promoting civic engagement, and addressing social needs are all crucial to a successful service-learning project in addition to strengthening the community at large. Other key components include reciprocation between the students and the community entity being served. Reflection by the student is also crucial to a successful learning experience.12 Elyer and Giles discuss the importance of matching the academic goals with the placement of students in the community setting in addition to student reflection as a way to deepen the transfer of knowledge learned in the engagement.13 Other important pieces noted by these authors include the students’ relationship with the community partner, the time or duration of the experience, and the student’s perception of the quality of the service-learning experience.13 CODA evaluates the dental institutions’ ability to make sure students are culturally competent; therefore, implementing service-learning opportunities in the dental hygiene curriculum is an effective way to ensure this outcome.
As an innovative approach to dental hygiene education and public health, a service-learning outreach clinic called Oral Health on Wheels (OHOW) began full operation as a clinical rotation for dental hygiene students at Johnson County (KS) Community College (JCCC) in August 2008. Following successful capital fundraising and college commitment towards ongoing operating expenses, a mobile dental hygiene vehicle was purchased to implement this service-learning program (Figure 1 and Figure 2). The mobile dental hygiene clinic is a 43-foot custom designed truck (LifeLineMobile®) outfitted with two complete dental operatories, sterilization area, patient intake, waiting room, and a wheelchair lift. Clinical rotation on the OHOW allows dental hygiene students to participate in and provide the full scope of dental hygiene services to culturally diverse patients and those with special needs. The OHOW continues to be fiscally supported by the college and is, therefore, maintained as an enriching clinical experience for the dental hygiene students. Operations of the OHOW are monitored by a full-time dental hygiene faculty who is the project coordinator. Additionally, community dentists are employed to enhance inter-professional education.12,13 Second-year dental hygiene students spend a three-week rotation in the OHOW as part of their clinical instruction. A 1:1 faculty-student ratio on the OHOW allows for extended learning and assistance with new patient experiences with special populations served by OHOW (Table 1).
Community Partners (Reciprocal Component)
The OHOW partners with two Johnson County service agencies, including Johnson County Developmental Supports (JCDS) and Johnson County Department of Health and Environment (JCDHE). A third partnership is in place with an outreach center, Center of Grace. Clients from JCDS are diagnosed with mild to severe intellectual and developmental disabilities. Patients seen at JCDHE are pregnant mothers, while Center of Grace clients are predominantly Hispanic adults. Table 2 describes the demographics of these community partners. Eligibility of consumers is determined by the JCDS Director of Clinical Supports. Appointment scheduling is maintained by nursing staff using a re-care system prescribed by OHOW staff to benefit clients’ periodontal health. Wednesday treatment alternates between JCDHE and Center of Grace outreach center. Clients at JCDHE are informed of the health benefits and provision of oral health services provided on OHOW through an internal intake system by WIC coordinators and nurse practitioners. Clients are then scheduled for a screening by the bilingual social workers in order to begin treatment as most of the clients served are Spanish speaking. Clients at Center of Grace are given appointments on a first-come first-serve basis. These patients continue care if they are still enrolled in ESL classes at the center.
OHOW Operations: Faculty, Staff, Students
Supervision of the OHOW mobile clinic is conducted by a full-time dental hygiene faculty from the college. A community pool of dentists make up the staff dentist position on the OHOW. One dentist is on the mobile unit during each rotation. Two dental hygiene students rotate through the mobile dental clinic at one time, twice per week. The same dentist maintains the staff position every Monday, serving clients at JCDS. The consistency of the same dentist on site with the special needs population strengthens the acceptability and comfort level for the patients. Currently, five remaining dentists rotate to fill the Wednesday staff dentist position participating from 1 to 5 days per semester. This community pool of dentists strengthens the relationship with the local dentist community and shares the learning experiences the college offers the dental hygiene student. In order to facilitate the cross-cultural bridge with the Spanish-speaking community, an experienced interpreter/translator completes the OHOW team. As an integral part of the OHOW mobile clinic, the interpreter assists Spanish-speaking clients with completion of forms, referrals (English/Spanish), understanding treatment findings and needs, oral healthcare instruction, scheduling, and post-treatment follow-up.
The literature is clear that dental hygiene education is a conducive platform to providing students with valuable service-learning experiences as an avenue for creating community partnerships.2,14 Therefore, the purpose of this service-learning project was to provide dental hygiene students a unique opportunity to gain meaningful patient care experiences with special needs and culturally diverse underserved populations through a mobile community-based clinic. In addition, this study evaluated student satisfaction with their experience on the OHOW rotation through a student feedback survey.
Methods and Materials
Students participated in the OHOW rotation 3 weeks at a time, two times per week. Prior to participation, students review and complete a series of modules on “Practical Oral Care for People with Developmental Disabilities.”15 Students also complete a take-home exam on this information, thereby increasing their ability to work with and treat patients with special needs and those from underserved populations.
In order to evaluate student satisfaction of the OHOW service-learning project, a Student Feedback Survey was administered to all students who participated in the project over the 5 years from 2009 to 2013. The survey was administered at the culmination of the second year, prior to graduation, giving the students time to reflect on their service-learning experience. The survey was blind and consent was given by participation. A total of 90 students completed the survey from 2009 to 2013. Completion of the survey was not required.
The survey measured the degree to which OHOW increased student awareness of underserved populations, cultural diversity, clinical skills, confidence building, dental team working relationships, and the delivery of ethical patient care. Students also provided open-ended feedback about current program operations and the degree to which the rotation may have influenced their clinical dental hygiene education as well as future professional endeavors. In this way, the survey assessed both quantitative and qualitative feedback.
The Feedback Survey was adapted from one used in a study by Ashton-Brown et al, where the authors evaluated the use of public health clinics in a service-learning rotation for dental hygiene students.16 That survey was originally modeled after the Health Professions Schools in Service to the Nation program taken from the handbook Methods and Strategies for Assessing Service-Learning in the Health Professions.17 The final adaptation of the survey in this study included a total of 25 questions. These 25 questions were broken into three sections. The first section included 10 questions pertaining to skill development with a five-point Likert scale answer ranging from 1 = not at all, to 5 = very much. The second section included 11 questions relating to the students’ experiences on the service-learning rotation. The Likert scale in this section ranged from 1 = strongly disagree to 5 = strongly agree. Lastly, section 3 included four questions for students to provide reflection on things they learned and/or might change, advice for the project, and any comments they would like to share with the faculty and staff about their service learning experience.
In order to assess the students’ learning strategies while on the OHOW rotation, students conferenced with the program director at the end of each rotation. Students provided reflection regarding their triumphs, progress, and opportunities for clinical skill improvement based on their performance. Progress evaluations were also submitted to the Second Year Lead Clinical Coordinator(s) of Clinic III and IV for consideration during clinic course conferences, which served as additional reflection.
Results
Out of the 90 students who responded to the survey, 85 (94.44%) indicated satisfaction and personal growth after their clinical experiences on the OHOW rotation. These responses provided valuable feedback for any changes in the curriculum related to intellectually and physically disabled populations. Students reported significant satisfaction, personal growth, and confidence while working with clients with intellectual and developmental disabilities (P ≤ .05). The JCDS service site was repeatedly favored by the dental hygiene students. Additionally, students expressed how the OHOW rotation exceeded their clinical expectations and personal satisfaction in treating clients with special needs.
The survey also ascertained the degree to which the OHOW experience enhanced the students’ dental hygiene education in working with diverse, underserved, multicultural, and special needs populations. Table 3 shows the Pearson correlation of students’ responses to key questions asked on the survey. Students expressed a significant level of satisfaction in many domains. Responses demonstrated strong correlations between student learning and their understanding of underserved populations (r = 0.504), building confidence in skills (r = 0.645), participation as a dental team member (r = 0.586), and understanding their role in total patient care (r = 0.545) (Table 3). The strong correlations among these key questions related to their clinical experience and confidence, skills, integration into the dental team, and understanding of both total patient care and their increased understanding of the needs of special populations. All of these items speak to the core mission of the OHOW program. Students also responded favorably to the advanced challenges presented in case treatment. Comments consistently reported a favorable learning environment and skill acquisition in the mobile facility. Students also reported significant satisfaction with their experience working as a team of professionals in order to treat the underserved populations on the OHOW facility.
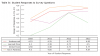
The Johnson County Community College survey demonstrated a high satisfaction with the ability of the OHOW rotation to enhance the dental hygiene students’ ability to provide dental hygiene care. Student comments included, “challenging, but a good experience,” “by far my favorite rotation site,” and “I wish I could have been on the truck all the time, I learned so much.” This feedback is essential in order to continue to provide each student with an authentic learning environment while meeting the needs of each service center. Several key questions are noted regarding the treatment of underserved populations learning, working as a team, and serving patients without discrimination. Table 4 demonstrates student responses to these key questions. It highlights student responses to working with underserved populations, learning more skills, working as a team and learning the value of serving patients with special needs. There was a major increase in the student’s perceived ability to learn more skills during their rotation on the OHOW service-learning project.
The unique operation in the OHOW setting allows students to treat special needs and underserved populations in a 1:1 faculty/student ratio. Significant satisfaction was expressed by students regarding the learning environment and treating patients with intellectual (ID) and developmental (DD) disabilities. Open-ended responses on the OHOW survey indicated students’ comfort level with treating ID and DD patients through JCDS were quite positive. One piece of advice given by a student stated “I would tell next year’s students about how great of an experience it is working with the population selected: rewarding, so just relax and think of the service being provided.”
Discussion
The faculty and administration at JCCC are committed to implementing and continuing service-learning projects in the dental hygiene program. Students’ positive response to their OHOW service-learning experience supports the mission of the educational arm of the dental hygiene program and the mission of OHOW. The strong correlations identified in this service-learning evaluation project may be due, in part, to the unique environment in which learning takes place. Students are encouraged and directed by all faculty and staff on how to use their knowledge and skills to deliver exceptional patient care while continuing to sharpen their professionalism.
The most significant results were from the JCDS service site. Students indicated treating clients with either intellectual/developmental disabilities (ID/DD) exceeded their expectations clinically and gave them personal satisfaction. In this setting students work with case/social workers, support staff, nurses, and dentists as well as the dental hygiene OHOW program coordinator. These results coincide with expected competencies of a graduating dental hygienist as indicated in the CODA standards (2-12), which address student competency in assessing treatment for patients with special needs.6 Additionally, having the project coordinator who is a full-time faculty on site at all times, increases the experience, supervision, and skill development of the student. Many of these recommendations are outlined in the Macy study, which favors a more community based dental education model.18
Students utilized didactic lessons learned in the classroom and applied that information in the mobile clinical setting under guided instruction. This guided instruction is thought to reduce potential apprehension when treating patients with ID and DD. The students’ ability to learn from their experience is an internal process within themselves. Different from the onsite clinic, students do not have scheduling burdens, as scheduling is done by the site personnel and project coordinator. This reduced burden may also allow students to focus on the task presented to them. Working with a Spanish interpreter also creates seamless communication with the Hispanic patient population. Students learn how to work with the interpreter for effective translation. It is understood that an interpreter is not available for every non-English–speaking encounter post-graduation; however, the experience provides students with an appreciation of the interpreter as a key member of the oral healthcare team. Additionally, this experience may give students the tools needed to navigate the public healthcare system in their future career endeavors.12
Other student feedback demonstrated a high satisfaction with their ability to provide dental hygiene care for special needs populations. Students became more aware of and sensitive to the unmet needs of underserved and diverse populations. One comment, in particular, highlights this reflection: “The most important thing I learned in my rotation was providing dental hygiene care for special needs patients, and having patience for others having trouble understanding.” This outcome demonstrates how the OHOW project has helped to increase the students’ sense of professionalism and civic responsibility as an oral healthcare provider.9,12
Results of this service-learning project are consistent with other research such as Wolff et al, which stated that the more experience dental students had with treating persons with intellectual disabilities, the more positive their attitude concerning this population.19 In another study by Aston-Brown et al, the authors found that after experience in a service-learning rotation opportunity in the public health environment, dental hygiene students expressed an improved understanding of ethical patient care and awareness of underserved populations and cultural diversity.16 These authors underscore the necessity of service learning as a way to increase student awareness of dental public health as an alternate career choice.16 These suggestions have been cited in the literature as integral components for a successful service-learning project.9,12,13,18
Lautar describes the characteristics of service learning in dental hygiene education.20 She suggests how providing sealants within a rural community is a good example of a service-learning project in the dental hygiene curriculum. This activity meets the needs of the underserved children in the community in addition to giving students exposure to a population they might not generally be able to treat.20 Likewise, the OHOW project meets the oral healthcare needs of underserved disabled populations, exposes students to community service, and connects and engages students to the community. Students are able to reflect on their experience and become more culturally competent.16
Another study utilizing a one-on-one faculty mentor approach found similar outcomes after the mentors’ dental hygiene students participated in a “Miles of Smiles” service-learning rotation.21 Results indicated students were able to increase their clinical skills, became more aware of community oral health needs in child populations, found satisfaction in working with these patients, and developed an appreciation for alternative models for delivery of oral healthcare.21
Elyer and Giles suggest that a crucial component of an effective service-learning project is connecting the academic goals with the placement of students in the community setting, further deepening engagement.13 The outcomes of this study demonstrated this suggestion by these authors. Students’ perceptions of the OHOW rotation were favorable, showing high satisfaction in their feedback, demonstrating the experience to be valuable both personally for their clinical skills and impacting their sensitivity to underserved populations.
A unique hallmark of service learning in dental hygiene is how the community partner benefits from the service provided.9 Patient surveys are shared with students as part of the student feedback process and reflection, allowing the students to see the direct impact and appreciation clients express after receiving oral healthcare services from the OHOW project. As part of the national oral healthcare objectives, working as a team to reduce the burden of oral disease is seen as an integral part to promote health and quality of life for all individuals.4 As educational institutions change the delivery of dental education for future healthcare professionals, it is hypothesized that the changes may produce oral health professionals with a renewed dedication to reach out to underserved populations.
Long-term data continue to be collected on the OHOW project and will be valuable in assessing the future impact of the service learning from both the student and community partner perspective. Follow-up study should include information from graduates to assess how the project impacted their choice of employment in public health clinics. Additionally, future plans include utilizing an Advanced Education in General Dentistry resident on the OHOW rotation 1 day per month to collaborate with the students and patients as well as reduce the burden of care in underserved populations.
Conclusion
The main purpose of the OHOW project was to evaluate its impact on student satisfaction and their ability to gain valuable clinical experiences treating underserved populations. The results demonstrated the OHOW project was able to meet its stated purpose as students were highly satisfied. Rotation on the OHOW increased student learning and understanding of underserved populations, built confidence in their clinical skills, and increased their participation as a dental team member and their understanding of their role in total patient care. Lastly, results from this study support the ADEA Commission on Dental Education recommendations for improving oral health for all Americans. The OHOW service-learning project allows dental hygiene students a unique opportunity to engage with their community while acquiring necessary clinical competencies required by national accreditation and providing access to oral healthcare services to underserved patients who would otherwise go without treatment.
ABOUT THE AUTHORS
Heather Flick, RDH, MS, MPH, is Professor, Department of Dental Hygiene, Johnson County Community College, and Project Coordinator, Oral Health on Wheels. Sheri Barrett, EdD, is Director, Outcomes Assessment, Johnson County Community College. Carrie Carter-Hanson, RDH, MA, EdD, is Director, Department of Dental Hygiene, Johnson County Community College.
REFERENCES
1. US Dept of Health and Human Services. A National Call to Action to Promote Oral Health. Rockville, MD: US Dept of Health and Human Services, Public Health Service, Centers for Disease Control and Prevention, and The National Institutes of Health, National Institute of Dental and Craniofacial Research; May, 2003. NIH Publication No. 03-5303.
2. Institute of Medicine and National Research Council. Improving Access to Oral Health Care for Vulnerable and Underserved Populations. Washington, DC: The National Academies Press; 2011.
3. Haden NK, Catalanotto FA, Alexander CJ, et al. Improving the oral health status of all Americans: roles and responsibilities of academic dental institutions. The report of the ADEA President’s Commission. J Dent Educ. 2003;67(5):563-583.
4. US Dept of Health and Human Services. Office of Disease Prevention and Health Promotion: Healthy People 2020 NASnewsletter (2002/05/04 ed., Vol. 15, p. 3): US Dept of Health and Human Services; 2012.
5. Albino JE, Inglehart MR, Habil P, Tedesco LA. Dental education and changing oral health care needs: disparities and demands. J Dent Educ. 2012;76(1):75-88.
6. Commission on Dental Accreditation. Accreditation Standards for Allied Dental Hygiene Education Programs. Chicago, IL: American Dental Association; April 2013.
7. McKinnon M, Luke G, Bresch J, et al. Emerging allied dental workforce models: considerations for academic dental institutions. J Dent Educ. 2007;71(11):1476-1491.
8. Kansas Dental Board. Kansas dental practices act statutes and regulations and related law relating to dentists and dental hygienists. Kansas Dental Board [Internet]. 2014 [cited 2015 April 25]. http://www.dental.ks.gov/laws/kansas-dental-practices-act.
9. Yoder KM. A framework for service-learning in dental education. J Dent Educ. 2006;70(2):115-123.
10. Siefer SD. Service-learning: community-campus partnerships for health professions education. Acad Med. 1998;73(3):273-277.
11. Brown JS, Collins A, Duguid P. Situated cognition and the culture of learning. Educational Researcher. 1989;18(1):32-42.
12. Hood JG. Service-learning in dental education: meeting needs and challenges. J Dent Educ. 2009;73(4): 454-463.
13. Elyer J, Giles DE, Astin AW. Where’s the Learning in Service-Learning? 1st ed. San Francisco, CA: Jossey-Bass; 1999.
14. Dehaitem MJ, Ridley K, Kerschebaum WE, Inglehart MR. Dental hygiene education about patients with special needs: a survey of U.S. programs. J Dent Educ. 2008;72(9):1010-1019.
15. US Dept of Health and Human Services, National Institutes of Health. Continuing education series: Practical oral care for people with disabilities. 2008. www.nidcr.nih.gov.
16. Aston-Brown RE, Branson B, Gadbury-Amyot CC, Bray KK. Utilizing public health clinics for service-learning rotations in dental hygiene: a four-year retrospective study. J Dent Educ. 2009;73(3):358-374.
17. Shinnamon A, Gelmon SB, Holland BA. Methods and strategies for assessing service-learning in the health professions. San Francisco, CA: Community-Campus Partnerships for Health; 1999.
18. Formicola AJ, Bailit HL, Beazoglou TJ, Tedesco LA. Introduction to the Macy study report. J Dent Educ. 2008;72(2 suppl):5-9.
19. Wolff AJ, Waldman HB, Milano M, Perlman SP. Dental students’ experiences with and attitudes toward people with mental retardation. J Am Dent Assoc. 2004;135(3):353-357.
20. Lautar CJ, Miller FY. Service learning and dental hygiene: a literature review. J Dent Hyg. 2007;81(3):64.
21. Simmer-Beck M, Gadbury-Amyot, CC, Ferris H, et al. Extending oral health care services to underserved children through a school-based collaboration: part 1: a descriptive overview. J Dent Hyg. 2011;85(3):181-192.