You must be signed in to read the rest of this article.
Registration on CDEWorld is free. Sign up today!
Forgot your password? Click Here!
INTRODUCTION AND OVERVIEW
General principles for preoperative evaluation of the dental patient and cardiovascular considerations were addressed in part one of this article.1 Although the categories of disease addressed in these articles are so complex that they justify a medical specialty dedicated to each, our focus is to provide only a basic understanding of the pathophysiologic features of the principal conditions. This will enable the provider to comprehend the patient’s status and to properly design a plan for appropriate management while providing dental care.
PULMONARY DISEASE
The respiratory system can be afflicted with a vast number of disorders, but asthma and diseases that contribute to chronic obstructive pulmonary disease (COPD) are most prevalent. Furthermore, these particular disorders have the most significant impact on patient management during dental care.
Asthma
Asthma is an inflammatory disease of the airways characterized by increased responsiveness of the tracheobronchial tree to a variety of stimuli.2 It is an episodic disease, with acute exacerbations interspersed with symptom-free periods. During an acute attack, widespread narrowing of the air passages occurs as the result of bronchospasm and the patient experiences dyspnea, cough, and wheezing. Most attacks are short-lived, lasting minutes to hours depending on medications, and the patient normally recovers completely after an attack. However, on rare occasions, the obstruction can persist for days or weeks—a condition called status asthmaticus.
The key feature of asthma is a persistent subacute inflammation in which submucosal glands are hypertrophied and the submucosal tissue is profuse with mast cells, eosinophils, neutrophils, and lymphocytes. Inflammatory autacoids including cytokines produced by leukocytes and mucosal cells are responsible for three events that narrow the airways: (1) edema, (2) production of mucus, and (3) increased thickness and spasms of bronchial smooth muscle.
The inflammatory process in asthma is allergic in character, triggered by immunoglobulin (IgE) antibodies in lung tissues. However, a minority of asthmatics (~10%) are negative following antigenic provocations. This finding accounts for attempts to classify asthma as allergic or extrinsic and idiosyncratic or intrinsic based on the principal stimuli that incite acute episodes. Asthma most often is allergic (extrinsic) in nature and is associated with a personal and/or family history of atopy; provocations include drugs, foods, preservatives, and environmental allergens. Some patients have no personal or family history of allergy and are said to have idiosyncratic (intrinsic) asthma. For these patients, acute attacks are provoked by exercise, emotions, or common upper respiratory infections such as the common cold. These distinctions are merely a convenience for discussion and treatment strategies; patients often respond to both categories of stimuli.
The asthmatic patient should be questioned regarding factors that precipitate wheezing and the medications used. It is important to appreciate that albuterol is rapid acting in relieving an acute episode. Most other medications are intended as long-term medications intended to suppress inflammation (eg, corticosteroids, leukotriene antagonists) or provide sustained bronchial relaxation (eg, salmeterol, theophylline, ipratropium). The severity of the patient’s condition can be deduced by the number of medications prescribed and the frequency at which albuterol is required for rescue.
In general, drugs that release histamine should be avoided. Although many opioids are notorious in this regard, they have never been shown to have deleterious effects in asthmatic patients. In fact, they actually may be desirable because of their depressant effects on airway reflexes and coughing. Formerly, antihistamines and other anticholinergics were believed to increase the viscosity of mucus and, therefore, were contraindicated in patients with asthma or COPD. This concern has been dispelled, however, and the anticholinergic drugs, most notably ipratropium (Atrovent), currently are enjoying a reprise for long-term therapy.
Chronic Obstructive Pulmonary Disease (COPD)
Chronic obstructive pulmonary disease is a slowly progressive respiratory disorder characterized by reduced maximal expiratory flow during forced exhalation. This is measured during pulmonary function testing as forced expiratory volume in 1 second (FEV1) and forced vital capacity (FVC). These measurements are used to categorize severity3 (Table 1). Most of the airflow obstruction is fixed because of chronic narrowing, but varying degrees of bronchial hyperreactivity (bronchospasm) may be superimposed and reversible, sometimes described as having an asthmatic component. COPD is attributed primarily to emphysema and/or chronic bronchiolitis, but these conditions may exist alone and can be mild enough that they do not limit airflow. Only when chronic obstruction develops can the patient’s condition be termed COPD.3,4 Emphysema is defined by anatomic changes. It is a permanent enlargement of airspaces distal to the terminal bronchioles without obvious fibrosis and attributed to destruction of alveolar septae. Chronic bronchitis and bronchiolitis are defined according to clinical signs, including a persistent productive cough not attributable to infection. Depending on the relative proportion of each disease component, patients may be hypercapnic or hypoxemic or may suffer some degree of right and/or left heart failure.
COPD evolves from a chronic inflammatory process that differs markedly from that seen in asthma; inflammatory cells and chemical mediators are entirely different. In asthma, the inflammation causes secretion of mucus and hyperreactivity of airway smooth muscle that can be reversed, at least temporarily. In COPD, normal airway tissues are permanently damaged by inflammation generated by both innate and adaptive immune responses.5 Smooth muscle spasm is not a key feature but may be present to varying degrees. Although inflammatory mediators involved in COPD are less well defined than those in asthma, the inflammation is believed to be immune-mediated in response to oxidative stress, a term that describes the combination of increased activity of oxidants and decreased activity of antioxidants. The oxidants in this case are largely proteolytic enzymes released by neutrophils and macrophages, along with their byproducts. Despite the strong etiologic association between smoking and COPD, only 15% to 20% of smokers manifest the disease, although as many as 50% of heavy smokers are afflicted.5 Additional environmental oxidants and heritable factors that determine adaptive immune responses likely act in concert to produce the disease.5 Alpha1-antitrypsin is a target at which smoking, environmental oxidants, and genetics converge. This enzyme normally destroys oxidants that initiate inflammation. Individuals can inherit a deficiency of this enzyme, but smoking has been found to suppress its activity.
In addition to inadequate oxygen delivery to all body tissues, COPD produces a significant strain on the right ventricle of the heart. Impaired delivery of oxygen to the alveoli causes constriction of pulmonary vessels. This reflex is believed to be an effort on the part of the body to shunt blood toward better oxygenated alveoli for gas exchange. However, this resistance within the pulmonary arteries overburdens the right ventricle in attempting to pump blood through the lungs. In severe cases, the right ventricle may fail as a result of this strain/a condition called cor pulmonale. In such cases, the patient will exhibit peripheral edema in the arms and legs. The constriction of pulmonary vessels can be prevented somewhat by improving alveolar oxygen tension through supplemental oxygen therapy.
Despite the apparent advantage of oxygen therapy in COPD, it must be used with caution because of a change in ventilatory control. Normally, ventilation is stimulated by elevated levels of carbon dioxide (ie, hypercapnic drive). However, the respiratory center becomes tolerant to elevated carbon dioxide (hypercapnia) associated with COPD. In these patients, the stimulus to breathe is driven by low oxygen tension (ie, hypoxemic drive). Oxygen therapy may elevate oxygen tension to the point that there is no stimulus to ventilate and the patient may become apneic, especially when asleep or unconscious for other reasons. Previously, it was recommended that any supplemental oxygen for patients with COPD should be limited to a maximum of 40%. This is no longer the case. Current thinking is to provide supplemental oxygen in increments until the patient can sustain an oxygen saturation of >90 by pulse oximetry.3,4 Central nervous system depressants must be used cautiously in these patients, most notably, the opioids, which depress central carbon dioxide drive, and the inhalation anesthetics, which have a profound effect on peripheral hypoxemic drive.6
Finally, some personal suggestions regarding assessment and scheduling of COPD patients. Chronic respiratory failure is defined as an arterial oxygen tension <60 mm Hg while breathing room air.3 This corresponds to a hemoglobin saturation of <90 by pulse oximetry (SpO2). During preoperative assessment, a patient with COPD who cannot sustain a pulse oximetry reading >90 should be regarded as having stage 4 disease and presents a significant medical risk. Patients with moderate to severe disease should be scheduled for mid to late morning appointments. Afternoon appointments may be undesirable owing to patient fatigue as the day progresses. Furthermore, early morning appointments can be problematic because of coughing and attempts at expectoration of mucus accumulated during the preceding night.
ENDOCRINE DERANGEMENTS
Thyroid Disease
Most patients who have a history of thyroid disorder are controlled and present in a euthyroid state. In this case, there is little concern regarding sedation and anesthesia. However, patients who have questionable control are a matter of concern whether hypoactive or hyperactive in their status. The hypothyroid patient can be very sensitive to central nervous system (CNS) depressants and is at increased risk for bradycardia, hypotension, hypothermia, and hypoglycemia. Patients medicated with thyroid replacement (eg, Synthroid) may be functionally hyperthyroid if they are consuming an excessive amount. For this reason, careful attention to preoperative vital signs is essential because hypertension and tachycardia can be indicative of a relative hyperthyroid status.
Hyperthyroidism is associated with excessive production of thyroid hormone, which overly excites cardiac tissues. These patients should not receive local anesthetics that contain epinephrine because they are at risk for thyroid storm, a hypermetabolic state that includes hyperthermia, hypertension, and cardiac arrhythmias. Treatment of such patients should be delayed until a euthyroid state can be confirmed.
Adrenal Disorders
Primary adrenal derangements are complex and produce a staggering number of metabolic complications related to abnormal levels of adrenocortical hormones, both mineralocorticoids and glucocorticoids, as well as medullary catecholamines. Fortunately, these conditions are rare but when present require consultation with the patient’s endocrinologist to confirm a stable condition. The adrenal gland is vital for normal survival, and primary dysfunction creates a highly unstable medical status, especially in terms of cardiovascular stability.
More often concern is directed to secondary hypocorticism caused by prolonged glucocorticoid therapy. Patients who have adrenal atrophy may not be able to produce additional glucocorticoid levels normally required to cope with stressful conditions such as major surgery, and they may experience an adrenal crisis. In minor cases, this presents as an acute anxiety syndrome, but in severe cases, patients may experience hypotension and shock. However, adrenal crisis is an unlikely concern with typical dental and oral surgical procedures, especially when sedation is provided, and the following suggestion is consistent with that presented by Little et al.7 Should there be any concern regarding hypothalamic-pituitary-adrenal axis (HPA) function, a prophylactic dose of 50 mg to 100 mg of cortisol or its equivalent should be added preoperatively to the normal steroid regimen. If a particularly troublesome postoperative course is anticipated, it would be appropriate to increase the patient’s normal daily dosage by 25% to 50% for a day or two and then resume normal dosage.
Diabetes Mellitus
Diabetes mellitus is a group of metabolic diseases characterized by hyperglycemia resulting from defects in insulin secretion, insulin action, or both.8 Two major types of diabetes mellitus are known, reflecting differences in the origin and pathophysiology of the disease. Type 1 was formerly known as juvenile-onset diabetes or insulin-dependent diabetes mellitus (IDDM). Type 2 was formerly labeled maturity-onset diabetes or non–insulin-dependent diabetes mellitus (NIDDM). This dated nomenclature was based to a large extent on whether insulin was needed to control the disease. Current thinking is that diabetes mellitus is associated with several disease processes and may require more than just insulin replacement and insulin may be indicated in either category of disease.
Type 1 diabetes mellitus is characterized by absolute insulin deficiency, making patients dependent on exogenous insulin for survival. The insulin deficiency is attributed to an autoimmune destruction of pancreatic beta cells, and it is the result of both heritable and environmental factors. Type 2 diabetes is far more prevalent than type 1, accounting for ~90% of all cases of diabetes mellitus. Patients afflicted with type 2 diabetes retain some ability to secrete insulin but not enough to regulate their elevated glucose levels. Compounding this deficiency is the fact that tissues become resistant to the actions of insulin. Unlike type 1 diabetes, autoimmune destruction of islet cells does not occur in type 2 diabetes. Studies of identical twins have demonstrated a strong genetic influence; all identical siblings of type 2 patients also develop the disease. Thus, type 2 diabetes is regarded as an inherited disorder in which insulin resistance leads to overproduction of insulin initially, but eventually tissues become even less sensitive to insulin, and the capacity of beta cells to produce insulin is depleted.
Clearly, type 1 and type 2 diabetes mellitus are separate diseases, each leading to elevated glucose concentrations and impaired glucose tolerance. Once glucose concentrations remain chronically elevated, their eventual consequences are similar and largely attributable to microvascular and macrovascular changes. The severity of these changes is a consequence of the duration and the degree of hyperglycemia. Chronic elevations in blood glucose lead to the formation of glycoprotein deposits within vessel walls, which compromises their patency. Diminished perfusion results in diabetic retinopathy, diabetic nephropathy, and peripheral neuropathy. Alterations in lipid metabolism also contribute to macrovascular changes such as atherosclerosis associated with peripheral vascular disease, cerebrovascular disease, and coronary artery disease. The microvascular complications of diabetes rarely occur within the first 5 to 10 years after the diagnosis of type 1 diabetes. However, they may be present at the time of diagnosis in type 2 diabetes because of its slow and insidious onset and typical delay in diagnosis.
It is a common misconception that type 1 diabetes is of greatest concern when the actual issue is ongoing glycemic control, not the particular disease producing hyperglycemia. When poorly controlled, either class of diabetes mellitus results in long-term damage, dysfunction, and failure of multiple organs. When the diabetic patient is assessed, consideration should be given to cardiovascular and renal status. Patients with diabetes have an increased incidence of hypertension and coronary artery disease, and diabetic nephropathy is the leading cause of end-stage renal disease in the United States. The presence of neuropathies is a matter of particular concern, especially those involving the autonomic system. Autonomic dysfunction increases risk for bradycardia and hypotension associated with vasovagal responses or sudden postural change.
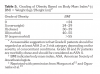
A good measure of glycemic control involves questioning the patient regarding his or her ‘‘hemoglobin test,’’ as in hemoglobin A1c. A single glucose reading offers little insight into the long-term glycemic control of an established diabetic patient. It merely identifies the patient’s glucose concentration at the time the blood sample was drawn. However, a small fraction of total hemoglobin (4% to 6%) is glycated (contains glucose) and is called glycosylated hemoglobin (HbA1c). Higher percentages of glycosylated hemoglobin confirm that blood glucose concentrations have been elevated for 3 to 4 months, because hemoglobin is found only in red blood cells, which have an average life span of 120 days. Thus, glycosylated hemoglobin percentages above 6% reveal ongoing hyperglycemia and indicate that the patient’s blood glucose is not under control9 (Table 2).
In the absence of end-organ complications, the individual with well-controlled diabetes poses little concern for the clinician in terms of sedation or anesthesia, other than ensuring that the patient does not become hypoglycemic. Hypoglycemia in the diabetic patient occurs when insulin levels are disproportionately high in relation to blood glucose concentration. It occurs when patients administer excessive insulin or consume excessive oral hypoglycemic medications and have inadequate food intake. The signs and symptoms of hypoglycemia generally commence as serum glucose concentrations decline to below 60 mg/dL; cognitive function deteriorates as concentrations fall to below 50 mg/dL.10
The common signs and symptoms of hypoglycemia can be categorized according to their mechanisms. Neurogenic mechanisms are first to appear and are attributed to the release of epinephrine and norepinephrine by the sympathetic nervous system. This reflects the body’s effort to elevate glucose by releasing these hyperglycemic hormones. Signs and symptoms include tachycardia, shakiness, and diaphoresis. This is followed by neuron-glycopenic influences that are attributed to depression of brain activity due to an insufficient supply of glucose. These generally present as tiredness, confusion, and overall mental clouding. The particular signs and symptoms in a given individual vary with the absolute blood glucose level, the rapidity of the decrease in blood glucose level, and the duration of hypoglycemia. Clearly, glucose replacement is indicated immediately if irreversible changes in brain function are to be avoided.
It is always wise to verify glucose concentration preoperatively. Because glucometers vary in their accuracy and sensitivity, it is reasonable to ask the patient to bring his or her personal unit to the appointment. Because of conventional NPO instructions, the patient’s medications may require adjustment. Well-informed patients who are taking insulin understand how to adjust the dosage when they skip breakfast. Otherwise it is prudent to ask the patient to consult his or her physician regarding insulin dosage. It is reasonable to have patients take half their normal morning dose and check their glucose level preoperatively. Oral hypoglycemic such as glipizide (Glucotrol) should be held until the patient can eat. Finally, it is significant that several of the newer agents used in diabetes management are not hypoglycemic in action. They are described as ‘‘antihyperglycemic’’ because they act by inhibiting the synthesis of glucose. These agents do not pose a risk for hypoglycemia and do not need to be withheld. Metformin (Glucophage) is a notable example.
KIDNEY DISEASE
Renal function is compromised by disorders that target the glomeruli or the tubules and interstitial tissues (tubulointerstitial). Any of these can become so severe that renal function is no longer adequate to sustain life. This is called renal failure and may be acute, but it more often presents as a chronic deterioration leading to so-called end-stage renal disease (ESRD) before overt failure occurs. Although chronic renal failure may be attributable to many disorders, diabetes mellitus is the leading cause. The overall incidence of new cases of ESRD in the United States is approximately 280 per million of population annually and has been steadily increasing over the past decade.
Injury to glomeruli allows proteins and/or red blood cells to enter the tubules, where eventually they are excreted in urine. This is described respectively as proteinuria and hematuria. It has become conventional to categorize glomerular disorders according to the degree of proteinuria discovered on urinalysis. When proteinuria is severe, it often is described as a ‘‘nephrotic syndrome’’; lower amounts of protein loss accompanied by red blood cells is regarded as a ‘‘nephritic syndrome’’ and generally is associated with acute inflammation (eg, glomerulonephritis).
The renal interstitium comprises a matrix of colloid, cells, and fibers that surround the nephrons and peritubular capillaries. The interstitium provides physical and nutritional support for the renal tubules and glomeruli, but interstitial fibroblasts are believed to secrete a hormone, erythropoietin, which stimulates red blood cell production in bone marrow. Primary tubulointerstitial injury can be attributed to a variety of toxic, metabolic, and genetic diseases, or to the use of medications such as nonsteroidal anti-inflammatory drugs (NSAIDs).
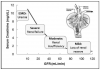
Renal failure occurs when the kidney is unable to maintain homeostasis and eliminate nitrogenous waste. Typically, a decline in glomerular filtration rate (GFR) is noted, along with retention of nitrogenous metabolic wastes such as creatinine and urea. This increased amount of nitrogenous waste in blood is called azotemia. Chronic renal failure is classified conventionally according to the decline in glomerular filtration, but this coincides with reduced creatinine clearance as well (Figure 1).
As some nephrons are damaged and renal function declines, the remaining nephrons undergo compensatory hypertrophy and other adaptations in an effort to maintain the composition of the extracellular fluid. Thus, until renal insufficiency is severe, these adaptations can provide reasonable function. However, severe renal failure and end-stage disease result in the dysfunction of many organ systems, highlighting the kidney’s central role in maintaining the internal environment of the body as a whole. These are summarized in Table 3 as uremic syndrome. For patients with end-stage disease, kidney transplantation is the only alternative to lifelong dialysis.
Mild and moderate stages of renal disease have little impact on patient management. Most of the conventional medications used for sedation and anesthesia are cleared hepatically. Propoxyphene and meperidine should be avoided however. Both are converted to metabolites with half-lives of 15 to 20 hours and are excreted renally. Neither is removed by dialysis. These metabolites act as CNS stimulants and will accumulate in all patients, but especially those with significant renal disease. In fact, they are poor choices for postoperative pain management in all patients. Of course the use of NSAIDs must be avoided if any degree of renal dysfunction is evident. For patients with severe disease, so-called nephrotic patients, some consideration should be given to lowering dosages of highly protein bound agents, such as etomidate and bupivacaine, if hypoproteinemia is suspected. Obviously, any medication that relies on renal clearance will require dosage adjustments.
For patients with severe renal failure and end-stage disease, dialysis generally is performed three times weekly. The arm containing the arteriovenous fistula (shunt) should be avoided when blood pressure is recorded or intravenous access established. Dental appointments are scheduled ideally on the day following dialysis. Consultation with the nephrologist is encouraged to discuss timing of the appointment and the patient’s general medical status. In particular, it is essential to confirm that hemoglobin and electrolyte status are stable because renal failure carries significant risk for anemia and electrolyte imbalance. Coagulation status should be confirmed if surgery is planned, and some degree of immunocompromise should be anticipated. For patients receiving dialysis, adjustments in dosage should be considered for commonly used antibiotics; these are summarized in Table 4.
Standard principles of patient monitoring should be followed for all patients with renal dysfunction with perhaps an increase in frequency of blood pressure assessment for those with severe or end-stage renal disease (every 5 to 10 minutes). Although hypertension and pulmonary congestion are more common consequences of renal disease, sedation and anesthesia may lead to hypotension because of the patient’s NPO status. In this regard, fluid administration is encouraged but must be done with caution to avoid overload and congestion. In general, 250 mL normal saline is an acceptable amount for a typical 1- to 2-hour procedure.
NEUROLOGIC AND MUSCULAR DISORDERS
In general, a history of neurologic dysfunction is not a matter of major concern, provided the condition is controlled medically. The epileptic patient should be maintained on the prescribed anticonvulsant regimen and consideration given to the fact that most of these medications are sedative in nature. However, the chronically medicated patient likely has developed tolerance to the sedative effects of these medications.
Parkinsonian patients suffer a defect in central dopaminergic activity. Their medications should be maintained and any use of antidopaminergic agents avoided. This would include phenothiazine and butyrophenone derivatives such as promethazine and droperidol, respectively. Because cholinergic input inhibits central dopaminergic transmission, anticholinergic agents may be useful adjuncts. In this regard, diphenhydramine, a histamine (H1) receptor blocker with anticholinergic activity, is an attractive addition to sedative and anesthetic regimens for Parkinsonian patients. In fact, diphenhydramine is the drug of choice for countering extrapyramidal symptoms that may follow the use of antidopaminergic agents, often used to manage nausea and vomiting.11
Although poorly understood, Alzheimer’s disease is a dementia that is believed to be related to a defect in central cholinergic transmission. For this reason, it is prudent to avoid the use of centrally acting anticholinergic agents. If such an agent is required, glycopyrrolate is most appropriate because its quaternary structure confers water solubility, which prevents it from crossing the blood-brain barrier and producing CNS effects. Lipid-soluble anticholinergic agents actually will counteract most of the drugs currently prescribed for Alzheimer dementia; these are cholinesterase inhibitors intended to elevate CNS levels of acetylcholine.
Multiple sclerosis is characterized as a demyelination process that most likely is related to an autoimmune mechanism. Patients experience localized or generalized neurologic deficits, which undergo periods of remission and exacerbation. Of special concern is autonomic involvement, which may predispose the patient to bradycardia and hypotension. Elective dental care should be scheduled during periods of remission when possible.
Muscular dystrophies are degenerative disorders of striated muscle that present a constant threat to ventilatory function. The Duchenne type, the most severe, typically compromises cardiac and skeletal muscles. Such patients are best hospitalized if sedation or general anesthesia is required.
Myasthenia gravis is an autoimmune disorder that consists of circulating antibodies against cholinergic receptors on skeletal muscle (ie, nicotinic receptors). As might be predicted, myasthenic patients are exquisitely sensitive to competitive neuromuscular blockers and their response to depolarizing agents is unpredictable. Cholinesterase inhibitors (eg, pyridostigmine) are used to manage this disorder, which introduces concern regarding parasympathomimetic side effects such as bradycardia and bronchoconstriction. Because of this, and because myasthenic patients are highly susceptible to ventilatory depression, deep sedation and general anesthesia are best avoided in the office. Mild to moderate sedation techniques may be used when the patient’s respiratory status is well monitored.
GASTROINTESTINAL DISEASE AND OBESITY
Most gastrointestinal disorders have little impact on patient management, other than the need to avoid NSAIDs for those with erosive and ulcerative disease. Patients who have gastroesophageal reflux disease (GERD) are at risk for aspiration during deep sedation and general anesthesia. Normally, dietary restriction protocols (NPO) prohibit solid food intake for 6 hours and clear fluids for 3 hours preoperatively. For this category of patient, however, it might be prudent to expand this restriction to nothing by mouth after midnight, other than normal medications. It is also wise to avoid supine or Trendelenburg positioning.
Liver disease obviously affects the clearance of many drugs used for sedation and anesthesia. Infectious and other inflammatory liver conditions generally have little impact, but the severity of cirrhotic changes with chronic disease must be considered. Of course dosages required to accomplish satisfactory sedation or general anesthesia cannot be reduced even when damage is significant, and postoperative management must take into consideration the possibility of delayed recovery. In this regard, inhalation agents are ideal, and for local anesthesia, articaine is attractive because of its rapid plasma clearance. Coagulation status must be confirmed before any surgical procedures are performed in severely liver impaired patients.
When cirrhosis is severe, oxygenation can be a matter of concern. Portal congestion and anemia lead to an increase in cardiac output and generalized arterial dilation. This allows for an elevation in venous pressures that produce a so-called right-to-left shunt due to venous blood shunting into arterioles. The result is hypoxemia, and a low preoperative SpO2 should warn of this possibility. Added to this issue is the fact that the presence of ascites will elevate the diaphragm, thereby reducing functional residual capacity.12 The sum of these issues mandates that patients be well oxygenated and that ventilation be monitored continuously.
Obesity is measured most accurately by the body mass index: BMI = Weight (kg)/Height (m2).With the use of this index, grades of obesity have been defined and offer an arbitrary basis for assigning such patients to ASA risk categories12,13 (Table 5). Obesity is associated with a myriad of cardiovascular, pulmonary, and metabolic derangements; these must be suspected even if the medical history is negative.
The obese patient requires a variety of considerations when the practitioner contemplates sedation and general anesthesia. It is not uncommon for obese patients to self-medicate with sympathomimetic agents for appetite suppression; this introduces concerns regarding heightened sensitivity to vasoconstrictors in local anesthetic formulations. Intravenous access is one of the most perplexing aspects of providing sedation and anesthesia for obese patients. Relaxing the patient with the use of orally administered benzodiazepines or nitrous oxide inhalation may be useful when difficulty is anticipated.
Assessment of airway and pulmonary status should be the initial consideration during preoperative evaluation. Obese patients often have short, thick necks and remarkably small mouths, which contribute to airway obstruction and difficulties for tracheal intubation. Diaphragmatic breathing can be compromised severely by the large quantity of abdominal fat, which makes chair position an important consideration. Obesity is associated with a reduction in functional residual capacity and increased oxygen consumption, which may lower baseline arterial oxygen tensions.13 Morbidly obese and super morbidly obese patients generally should not be candidates for office intravenous sedation or general anesthesia because of the significant risk for catastrophic airway problems. Serious consideration should be given to general anesthesia with awake tracheal intubation in a hospital where inpatient postoperative management is available. This latter consideration is particularly important because the large volume of distribution for lipid-soluble drugs delays their elimination, and airway compromise can be problematic during recovery.
Cardiovascular compromise, especially hypertension, is common in obese patients. Varying degrees of cardiomegaly attributed to left ventricular hypertrophy may be evident, and diminished cardiac reserve can result in poor exercise tolerance. Increased myocardial oxygen consumption, as well as several systemic metabolic derangements, accounts for an increased risk for ischemic heart disease. Abnormal glucose tolerance and unpredictable responses to insulin are frequent complications with obesity, and fatty infiltration may alter liver functions.
Pulmonary aspiration is an ever-present danger when deep sedation and general anesthesia are provided to obese patients. This is explained in part by the high incidence of hiatal hernia and GERD associated with obesity. Furthermore, the obese patient has increased gastric acidity and volume and intragastric pressure.12,13 For this reason, the preoperative use of anticholinergic drugs, histamine (H2) receptor antagonists, and metoclopramide should be considered to reduce gastric acidity and volume. NPO and patient positioning considerations are identical to those described earlier for patients with GERD.
PREGNANCY AND BREASTFEEDING
Clearly, all elective dental treatment should be avoided during pregnancy, especially during the first trimester. However, urgent dental care is required frequently for patients who are pregnant. Under these circumstances, it is not unusual for the patient to be anxious and fearful, often extremely so. For these patients, apprehension should be allayed by using the safest agents available; nitrous oxide frequently it cited as fulfilling this requirement.14,15 Furthermore, most of the conventional sedatives and opioids used for sedation and general anesthesia are considered safe and appropriate.14-17 Although benzodiazepines previously were believed to produce fetal malformations, these concerns have not been substantiated and no longer are held as true.17
Despite the fact that virtually all sedatives, opioids, and local anesthetics are lipid soluble and enter the fetal circulation, none has been found to produce harm following short-term use.14-16 When an agent is selected from a given class, prudence dictates using agents that have the shortest half-lives. Highly protein-bound agents distribute least, which makes bupivacaine an attractive local anesthetic when more than a few milliliters of solution is required. Dilute concentrations of vasopressors included in local anesthetic formulations do not appreciably alter uterine blood flow and should not be regarded as contraindicated.12 There can be no justification for subjecting an anxious pregnant patient to a stressful procedure on the basis of unfounded fear of fetal harm.
A few points should be considered regarding ancillary drugs for pain and infection. NSAIDs should be avoided, especially during the third trimester, because they inhibit formation of prostanoids that normally close the ductus arteriosus. Acetaminophen is the nonopioid of choice and hydrocodone generally is an acceptable opioid to most obstetricians. Other than tetracycline, conventional antibiotics used for dental infections, including beta lactams, macrolides, clindamycin, and metronidazole, are safe to administer.17
When managing the pregnant patient who is apprehensive, it is essential to prevent hyperventilation.14,15 Hypocarbia and alkalosis result in constriction of the umbilical artery, reducing fetal perfusion. During the second and third trimesters, uterine displacement should be accomplished by placing a pillow under the patient’s right side. This will provide a slight left lateral position, which relieves the vena cava of compression. Any evidence of complications during the pregnancy certainly warrants consultation with the patient’s obstetrician.
Most drugs taken by patients who are breastfeeding will transfer into milk in approximate amounts of 1% to 3% of the maternal dose.17,18 However, no cases of infant harm have been documented. Nevertheless, strategies are available to comfort mothers who are particularly concerned. Select drugs that have the shortest half-lives, and encourage patients so inclined to purchase a breast pump and store a 24-hour supply of milk for the infant following the procedure.
SUMMARY CONSIDERATIONS
Along with a complete medical history, baseline information regarding vital signs is an essential component of the medical record. It not only aids in assessing the patient’s medical status but also provides essential reference data during intraoperative monitoring. Ideally, the information is gathered during an interview appointment, when the patient is less likely to be apprehensive regarding eminent treatment.
In addition to the patient’s age, weight, and height, minimal essential vital signs should include blood pressure, pulse rate, and hemoglobin saturation by pulse oximetry. The airway should be examined and the Mallampati classification noted. The patient should be questioned regarding his or her physical stamina, including exertional or postural dyspnea and any history of lightheadedness or syncopal events. The dentist should note any visual impressions of cardiovascular, respiratory, or neurologic compromise. These might include evidence of distended jugular veins, edema of extremities, or elevated nail beds. For elderly patients, a notation regarding any evidence of dementia will be useful in evaluating any concerns regarding residual influences of sedative or anesthetic agents during the subsequent couple of days.
ABOUT THE AUTHOR
Dr. Becker is an Associate Director of Education, General Dental Practice Residency, at Miami Valley Hospital in Dayton, Ohio.
REFERENCES
1. Becker DE. Preoperative medical evaluation. Part 1: General principles and cardiovascular considerations. Anesth Prog. 2009; 56:92-103.
2. Barnes PJ. Asthma. In Fauci AS, Braunwald E, Kasper DL, et al, eds. Harrison’s Principles of Internal Medicine. 17th ed. New York: McGraw Hill; 2008.
3. Rabe KF, Hurd S, Anzueto A, et al. Global strategy for the diagnosis, management and prevention of chronic obstructive pulmonary disease: GOLD executive summary. Am J Respir Crit Care Med. 2007;176:532-555.
4. Reilly JJ, Silverman EK, Shapiro SD. Chronic obstructive pulmonary disease. In Fauci AS, Braunwald E, Kasper DL, et al, eds. Harrison’s Principles of Internal Medicine. 17th ed. New York: McGraw Hill; 2008.
5. Cosio MG, Saetta M, Agusti A. Immunologic aspects of chronic obstructive pulmonary disease. N Engl J Med. 2009;360:2445-2454.
6. Keats AS. The effects of drugs on respiration in man. Ann Rev Pharmacol Toxicol. 1985;25:41-65.
7. Little JW, Falace DA, Miller CS, Rhodus NL. Dental Management of the Medically Compromised Patient. 7th ed. St Louis: Mosby Inc; 2008:242-245, 187-192.
8. Expert Committee on the Diagnosis and Classification of Diabetes Mellitus. Report of the expert committee on the diagnosis and classification of diabetes mellitus. Diabetes Care. 2003;26(suppl 1):S5-S20.
9. Nathan DM, Kuenen J, Borg R, et al. Translating the A1C assay into estimated average glucose values. Diabetes Care. 2008;31:1473-1483.
10. Service FJ. Hypoglycemic disorders. N Engl J Med. 1995;332:1144-1152.
11. Stone DJ, DiFazio CA. Sedation for patients with Parkinson’s disease undergoing ophthalmologic surgery. Anesthesiology. 1988;68:821.
12. Morgan GE, Mikhail MS, Murray MJ. Clinical Anesthesiology. 4th ed. New York: Lange Medical Books/McGraw Hill; 2006:789-795, 813, 875-881.
13. Ogunnaike BO, Whitten CW. Anesthesia and obesity. In Barash PG, Cullen BF, Stoelting RK, eds. Clinical Anesthesia. 5th ed. Philadelphia: Lippincott Williams & Wilkins; 2006.
14. Santos AC, Braveman FR, Finster M. Obstetric anesthesia. In Barash PG, Cullen BF, Stoelting RK, eds. Clinical Anesthesia. 5th ed. Philadelphia: Lippincott-Raven; 2006.
15. Birnbach DJ, Browne IM. Anesthesia for obstetrics. In Miller RD, ed. Miller’s Anesthesia. 6th ed. Philadelphia: Elsevier, Churchill Livingstone; 2005.
16. Rosen MA. Management of anesthesia for the pregnant surgical patient. Anesthesiology. 1999;91:1159-1163.
17. Weiner CP, Buhimschi C. Drugs for Pregnant and Lactating Women. Philadelphia: Elsevier, Churchill Livingstone; 2004.
18. American Academy of Pediatrics Committee on Drugs. Transfer of drugs and other chemicals into human milk. Pediatrics. 2001;108:776-789.