You must be signed in to read the rest of this article.
Registration on CDEWorld is free. Sign up today!
Forgot your password? Click Here!
Mass-fatality incidents, whether natural or manmade, occur often and can overwhelm local, state, and government agencies, resources, and personnel quickly.1 Of critical importance is a rapid and effective response from skilled, multidisciplinary teams that are trained to manage each incident’s aftermath, including the identification of the deceased.2 Dental hygienists are widely distributed, and when trained in this area, can add to response capabilities during mass-fatality incidents in all aspects of postmortem dental examinations.2 Hence, preparation and training in anticipation of mass-fatality incidents is vital.2 The literature is devoid of models for mass-fatality preparedness and victim identification in dental hygiene curriculum; however, mass-fatality training has been recommended for predoctoral dental school curriculum.3-6 Mass-fatality training that incorporates computer-based multimedia to present topics through integrated text, sound, graphics, animation, video, imaging, and spatial modeling has been used in developing forensic training in dental curricula.3,7 Some dental educators believe exposure to and participation in forensic specialty coursework might also stimulate students’ interest in serving their community as a disaster responder.5,8
Dental hygiene education provides competencies in administrative skills, dental radiology, dental examinations, and documentation of the oral cavity applicable to a clinical setting. However, currently, there are no accreditation standards for mass-fatality training in dental or dental hygiene curriculum.3-6 Disaster-victim identification during a mass-fatality incident is the most important dental forensic specialty area for dental hygienists to participate in, and they are recommended as viable responders for disaster-victim identification efforts.9-11 The defined role of dental hygienists as a mass-fatality team member includes serving as dental registrars for managing antemortem and postmortem dental records, providing surgical assistance for jaw resections, imaging postmortem dental radiographs, and performing clinical examinations of the oral cavity as part of the postmortem or records-comparison teams.9-16 Identifying the deceased must be safe for emergency responders, as well as reliable and accurate.2,17,18 However, dental hygiene participation and education in mass disasters has been inadequately addressed in the literature. Expansive training is needed and recommended because practitioners with special forensics training and experience are better able to accomplish duties needed for identifications.2,4-9
There are a limited number of studies addressing how disaster preparedness should be developed in dental curriculum. In dental education, More et al specifically recommends a multimedia approach for catastrophe preparedness with “hands-on” simulations to provide an active learning experience, including mock disaster scenarios.3 More et al’s publication on the development of a curriculum to prepare dental students response to catastrophic events cites technology as “ideal” in combination with case studies, drills, and dramatizations using multimedia and simulated events.3
Investigators have suggested that mass-fatality training be interactive and provide assessments of skill acquisition, because regular practice and learning keeps skills and best practices for emergency preparedness and response current.5 Stoeckel et al5 and Hermsen et al6 recommend that forensic dental education for predoctoral dental school curriculums include identifying victims of a mass disaster using portable radiology equipment and victim identification software systems. Repeated practice is required to strengthen skills in radiographic imaging technique for exposure of postmortem dental remains.19
Meckfessel et al demonstrated that multimedia was effective in a dental radiology course.19 The Department of Oral and Maxillofacial Surgery of the Hannover Medical School introduced an online, multimedia dental radiology course called “Medical Schoolbook,” for predoctoral third-year dental students.19 It was designed to support multimedia learning modules.10 In the low-media module group, only 15 out of 42 students failed the radiology final examination. Two years after initiating the multimedia, only 1 out of 67 students failed the radiology final examination.19 The authors concluded that the radiology program benefited from additional media for teaching difficult concepts and transfer of knowledge.
Multimedia presentations of simulated events can provide an environment with authentic learning situations that facilitate knowledge transfer and retention beneficial for safe practice.20 Mayer found that media supports the way the human brain learns.22 His theory on the cognitive theory of multimedia learning supports dental educator’s recommendations for use of multimedia.21 Mayer’s theory centers on the idea that learners attempt to build meaningful connections between words and pictures, learning more deeply than with words or pictures alone.20,21 In the absence of an actual mass-fatality incident, learners need training resources that connect their established competencies with the additional competencies or skills needed for mass-fatality training and forensics. Multimedia could provide easily deployable training modules, which could be reviewed repetitively with actual demonstrations for just-in-time training, including abbreviated training sessions for untrained volunteers during the time of an actual incident.
The key elements of Mayer’s theory are based on three assumptions.20 First, the dual-channel assumption is that working memory has auditory and visual channels. Mayer’s “Modality Principle” states that people learn better from words and pictures when words are spoken rather than printed.20,21 Next, the limited capacity assumption is that working memory is limited in the amount of knowledge it can process at one time, so that only a few images can be held in the visual channel and only a few sounds can be held in the audio channel.20,21 Lastly, the active processing assumption explains that it is necessary to engage our cognitive processes actively to construct a coherent mental representation and to retain what we have seen and heard. Learners need to be actively engaged to attain or remember, organize, and integrate the new information with other or prior knowledge.20,21 Use of multimedia has several advantages, including observation of simulated experiences and opportunities for visualizing a process or procedure before being involved physically.20-23 This provides the potential for increased cognitive knowledge, analysis, and application of new knowledge in a “safe” environment.20-23 Stegeman and Zydney also found that learners who have repeated access to information and videos had an advantage over students who did not have access to the materials for further study.23
Mayer identifies improvement in learning as the “multimedia effect.”20 The presentation of audio and video are held in working memory simultaneously to create referential links between the two. In another study, Mayer and Moreno found that onscreen text and images can overload the learner’s visual processing system, whereas narration is processed in the verbal information processing system, requiring the student to both read and simultaneously view the mage.22 Both activities use a single channel, the visual channel. Video is single-channeled because our brains already pull the underlying video and audio together, and is considered multimedia.20,21 Because multimedia uses a single channel only, researchers believe information is easier to remember and retain.20,21 An image with accompanying narration is using dual channels, whereas narration is processed in the verbal information processing system, part of the auditory channel.20,21 Dual-channeling usually involves pictures and sounds, such as a narrated PowerPoint.
Emergency experts have underlined disaster preparedness as a way to reduce the many challenges that occur during incident response and management.1-18 This study investigates the effectiveness of strategies for mass-fatality training among dental professionals. More specifically, it assesses whether the use of multimedia is likely to enhance educational outcomes related to mass-fatality training. Multiple-choice examination scores and clinical competency-based radiology lab scores of two groups of second-year dental hygiene students were completed. Interest in this specialty area for each training approach was also assessed.
Methods and Materials
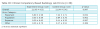
Mayer’s “Modality Principles” and Stoeckel et al’s recommendations for mass-fatality training in dental students were the basis for the use of multimedia and a “hands on” clinical competency-based radiology lab for the mass-fatality training in this study.3-6,20 A two-group, randomized, double-blind, pre- and post-test research design was used (Table 1). The sample for this educational evaluation included dental hygiene students in their first semesters of the second year of an entry-level baccalaureate degree program. All participants were required to have completed prerequisite coursework, to have completed 1 year in oral radiology, and to be certified in Virginia radiation safety. Pregnancy or suspected pregnancies were part of the exclusion criteria, due to the use of portable radiation devices in atypical positions. After Institutional Review Board approval, the researchers invited students to participate in the study via on an online announcement. Participation was voluntary, and students could withdraw from the study at any time without impacting their status in the dental hygiene program; 42 participants completed informed consent documents and were enrolled and randomly assigned to either the control group (n = 21) or experimental group (n = 21).
The control group viewed an educational module with low media (dual channeling), while the experimental group viewed information with multimedia (single channel). For the purpose of this study, multimedia was defined as media that integrated text, graphics, audio, and video demonstrations to allow for self-pacing, repetition of reading text, listening to and viewing materials, and/or guided demonstrations. Low media was defined as using teaching presentation software with text and graphics (PowerPoint) that also allowed for self-pacing and repetition, but only through reading and in an one-dimensional visual context.
The content for both of the educational modules was comparable and developed by an instructional designer and dental hygiene faculty members who have emergency preparedness and response training. All student participants viewed their assigned educational module with unrestricted access before participating in the clinical competency-based radiology lab. Both educational modules were deployed online via the university-supported Blackboard Learn system® (Blackboard, Inc).
The educational modules for both multimedia and low media were of parallel content and included the definition of forensic odontology, the role of the dental hygienist during a mass-fatality incident, and victim identification. The educational module specifically addressed biosafety considerations, personal protective equipment, and sterilization procedures in the mortuary setting. Dental radiography topics included techniques for using portable handheld radiographic equipment when imaging simulated victim remains and safe exposure of postmortem radiographs. An online pretest was given before viewing the educational module. The post-test was administered after student participants viewed the educational module and completed the clinical competency-based radiology lab. The multiple-choice pre- and post-tests had the same 15 forced-choice questions on interest in mass-fatality training and on taking radiographs of victim remains (two questions), knowledge of forensics (two questions), personal protective equipment, and infection control in a mortuary setting (four questions), radiation safety (three questions), and radiographic technique when imaging simulated victim remains (four questions). Students had 1 week prior to their clinical competency-based radiology lab to view the educational module in full. The clinical competency-based radiology lab included exposure of 11 intraoral radiographs of six fragments of lubricated and real human skulls with bitewing, anterior, and posterior periapical images.
To evaluate the performance of students on their technique when imaging dental remains, all radiographic images were scored by two calibrated examiners, and a radiographic evaluation form was used to identify errors in the following categories: angulation, placement, exposure, and density. Errors were entered as: 0 = no error, 1 = slight error not indicating a retake of the image, and 2 = nondiagnostic error requiring retake of the image. Students received instructions on technique through the educational module. No instruction on radiographic technique was given during the radiology lab portion of the study, and there were no retake exposures. Lab equipment included a portable handheld x-ray device (Nomad Pro®; Aribex, Inc), a direct digital image sensor (Schick Elite®; Sirona Dental), and a modified image receptor holder, which is used at onsite, temporary morgues during mass-fatality incidents.
Quantitative data analysis of interactions, pre- and post-test results, and radiology laboratory results were performed using SAS® 9.3 software. Significant differences existed at α = 0.05 for analysis of variance (ANOVA), after the assumption of normality and equality of variance had been met. Assumptions of equality of variances to validate the statistical tests performed were also conducted. More specifically, Levene’s test, Brown-Forsythe test, and Bartlett’s test for homogeneity of variance were found to have high P values, indicating that additional corrections were not necessary prior to making comparisons between groups.
Results
A total of 39 participants out of 42 (92.8%) completed the pre- and post-tests for the multiple choice exam (experimental group [n = 20], and the control group [n = 19]); 38 participants completed the radiology lab portion of the study (experimental group [n = 20], control group [n = 18]). One and two participants were excluded from each experimental and control groups, respectively, because they did not complete the research protocol in its entirety.
The means and standard deviations for the experimental and control groups were calculated. The mean sum pretest score for both groups combined was 8.1 (SD = 1.32). The mean sum pre-test score within the experimental group was 8.4 (SD = 1.35), and 8.2 (SD = 1.32) in the control group. Post-test scores for the groups combined was 9.9 (SD = 1.40), 9.95 (SD = 1.23) within the experimental group and 10 (SD = 1.6) within the control group. ANOVA indicated no significant gain between the groups; however, there was significant improvement in scores within each group (Table 2).
In the control group, the mean score for the pre-test was 8.2 (SD = 1.31), with a mean post-test score of 10 (SD = 1.59). Similar analysis revealed a significant improvement in scores with P value < .0001. Students reported similar interest in learning more about the role of the dental hygienist in disaster-victim identification for mass-fatality incidents from baseline (99.9%) to post-test (94.8%). Students reported slightly more interest in exposure to radiographic images on postmortem remains at the post-test (94.7%) compared to baseline (88.6%). Specifically, interest in disaster-victim identification had significant gain from pre-test to post-test scores, where the mean difference score was -0.07 (SD = 0.634) (P = .45). Results also suggest students from both groups showed an increased interested in postmortem radiographic imaging after the educational modules and clinical competency-based radiology lab, with a mean difference score of 0.12 (SD = 0.57).
Overall, the participants performed well in both the educational modules and clinical competency-based radiology lab with some improvement from pre- and post-test scores within the groups and little difference in scores between the two groups. In the experimental group, the mean score of 0.3 (SD = 1.09) revealed no significant gain in radiation technique knowledge (P = .16). Within the control group, there was also no significant difference in radiation technique knowledge, with a mean score of 0.26 (SD = 0.81). For radiation safety, there was a statistically significant gain in knowledge from pre- to post-test sums between the groups with a mean score of 0.69 (SD = 0.76) (P < .0001). The experimental group mean scores were 0.55 (SD = 0.68) and the control group mean scores were 0.84 (SD = 0.76). There was no significant gain in scores between the two groups for forensic knowledge (P = .210). Mean scores for the experimental group were -0.10 (SD = 0.45) and the control group means score was -0.1 (SD = 0.57). Lastly, a statistically significant difference was found between the two groups in terms of infection control scores (P < .0001). The experimental group had a mean score of 0.75 (SD = 0.79), and the control group was 0.79 (SD = 0.63). The correlation between radiation safety and technique was 0.33 (P = .0406). Therefore, a strong relation existed between the two variables. The greater the radiation safety scores, the greater the radiation technique score in both groups.
For the clinical competency-based radiology lab portion of the study, the higher the score on the radiographic evaluation form, the worse the performance or increase in errors per radiographic image. The experimental group had an overall mean score of 21.95, and the control group had an overall mean score of 21.94. No significant difference was found between the experimental and control groups in overall laboratory scores (P = .997). Comparisons were also made between the experimental and control groups in the specific error categories, which included errors in placement of the digital image receptor, vertical and horizontal angulation errors of the position indication device, exposure errors, mounting errors, and an “other” category for errors that did not fall within one of the above mentioned categories. Between the two groups, there were no significant differences within the four categories of radiographic technique errors. Table 3 presents the means, standard deviations, and related P values for each category. Because there were no mounting errors recorded for either group, this category was omitted.
Discussion
This study compared a low-media and multimedia approach to mass-fatality training via a multiple-choice examination, competency-based radiology lab, and an assessment of changes in interest in mass fatality as a specialty. This type of research is not currently found in dental hygiene literature. The mass-fatality training review suggested that approaches to preparing dental hygienists for disaster response and victim identification needs to be further explored. This study addressed this gap in the literature by looking specifically at dental-hygiene mass-fatality training within the framework of what has been published in the dental curriculum.
The majority of participants in each group at the post-test reported a high level of interest in mass-fatality training and in disaster-victim identification through exposing radiographic images on simulated victim remains, which supports the idea by Stoeckel et al that exposure to specialty coursework can encourage interest.5 Exposure to training in the forensic specialty area also gives dental and dental hygiene students the opportunity to decide whether they are interested in pursuing further training.
No statistically significant differences existed between the two groups; however, scores increased within each group. Both approaches resulted in increased scores. This increase in scores supports the recommendation by More et al for the use of multimedia for mass-fatality training.3 The discrepancy between the groups may be explained by what Jonassen et al describes as focusing on the student rather than a focus on the media.24 Jonassen et al states that “any reasonable interpretation of an instructional medium should be more than a mere vehicle.”24 He explains that educators should not assume that by simply adding media, the student’s cognitive processes will integrate the new information with the old.24 Students may not have been fully engaged with the media during the lesson. Also, while multimedia modules are designed to facilitate a way for students to repeat, interrupt, and resume the lesson at will, there is a large assumption that they will take advantage of those benefits. Students may choose to “cram” with technology and multimedia-based modules. Another explanation could be due to the small sample size (n = 21 in each group), which may have limited statistical power. In general, the results of our evaluation revealed that providing mass-fatality training can be offered through a multimedia approach.
For the clinical competency-based radiology lab assessment, both groups had a similar mean score from baseline to post-test with a 0.01 difference. In radiology education, a multimedia module with visual, audio demonstrations, and supplemental face-to-face instructor-guided lab demonstrations for skill acquisition may produce improved lab scores in the future. The educational modules allowed students to view demonstrations as needed, prior to the lab for review of difficult radiology concepts. This study supports that for difficult, hands-on skills such as radiographic technique, media could be used to enhance the learning process. These results support Stoeckel et al and Hermsen and Johnson’s recommendation for simulated exercises that allow students to practice clinical competencies such as the use of the portable radiology equipment and postmortem radiographic imaging.5,6
This study has some general limitations that preclude generalizing results to practice. Threats to the validity of the pre- and post-tests include the small sample size and the use of a convenience sample of dental hygiene students from an entry-level baccalaureate degree program. Because students were in the same program, it is possible that participants in the experimental group could have shown participants in the control group the multimedia educational module; participants could have also shared their clinical competency-based radiology lab experience with participants who had not taken that portion of the research study. The amount of study time is unknown because both educational modules were delivered online. Future studies should include larger samples sizes with a diverse sample of dental and dental hygiene students, practicing dentists and dental hygienists, and other dental team members from various universities and colleges. Additionally, this study did not utilize a full-curriculum approach because participants were evaluated based on one educational module and one attempt at the clinical competency-based radiology lab; researchers did not test long-term knowledge retention. Glotzer et al4 and More et al3 recommend catastrophe preparedness curriculum that is offered through multiple semesters by “supplementing the established curriculum with units of instruction.” Future research should identify educational methodologies that improve learning. The pre- and post-test limitations include asking 15 multiple-choice questions; a more reliable instrument would include questions covering a wider span of information. Modifications in research design and implementation may be required for application of instruction in different environments to include dental curriculum or just-in-time training during an actual mass-fatality incident. Additionally, researchers were not able to test whether multimedia might have an impact on the participant’s level of function during a mass-fatality incident; it is unknown whether or not a multimedia training approach would lead to better outcomes and recall in higher-stress situations.
This study contributes to the dental hygiene literature by assessing the effectiveness of multimedia in incorporating mass-fatality training and radiographic imaging of dental remains specific to dental hygiene. Multimedia approaches have been identified in the dental publications and curriculum; however, there are no peer-reviewed publications on what type of educational methodology should be used for mass-fatality training for dental hygienists.5,19 These findings, although based on a small sample size, demonstrated minimal differences when using a multimedia versus low-media approach to mass-fatality training. A combined approach could be used to develop training modules specific to dental hygiene mass-fatality preparedness, response training and simulated lab exercises allowing students to practice clinical competencies that are beneficial for taking radiographs on simulated victim remains. Future research should include more diverse, multidisciplinary samples, and longitudinal data.
Conclusion
Dental hygienists have participated in mass-fatality incidents and show promise in acts of community service and volunteerism. Training in anticipation of a mass-fatality incident is important for increasing the number of skilled and deployable dental professionals for recovery efforts.10
As training applicable to dental hygiene is developed and tested, dental hygienists can continue to add to response capabilities during a mass-fatality incident. Additional research in this area could contribute to the identification of teaching methods to to better prepare dental hygienists for a mass-fatality incident.
About the Authors
Tara L. Newcomb, BSDH, MS, is an Assistant Professor at the Gene W. Hirschfeld School of Dental Hygiene, Old Dominion University. Ann M. Bruhn, BSDH, MS, is an Assistant Professor at the Gene W. Hirschfeld School of Dental Hygiene, Old Dominion University. Loreta H. Ulmer, EdD, is a Senior Instructional Designer and faculty for the Center for Learning and Teaching, Old Dominion University. Norou Diawara, PhD, is an Associate Professor for the College of Mathematics and Statistics, Old Dominion University.
Acknowledgment
This research was supported by an Old Dominion University Faculty Innovator Grant.
References
1. Teahen P. Mass Fatalities: Managing the Community Response. 1st ed. Baco Raton, FL: CRC Press; 2012:421.
2. Brannon RB, Kessler HP. Problems in mass-disaster dental identification: a retrospective review. J Forensic Sci. 1999;44(1):123-127.
3. More FG, Phelan J, Boylan R, et al. Predoctoral dental school curriculum for catastrophe preparedness. J Dent Edu. 2004;68(8):851-858.
4. Glotzer DL, More FG, Phelan J, et al. Introducing a senior course on catastrophe preparedness into the dental school curriculum. J Dent Edu. 2006;70(3):225-230.
5. Stoeckel DC, Merkley PJ, McGivney J. Forensic dental training in the dental school curriculum. J Forensic Sci. 2007;52(3):684-686.
6. Hermsen KP, Johnson JD. A model for forensic dental education in the predoctoral dental school curriculum. J Dent Edu. 2012;76(5):553-561.
7. Von Wodtke M. Mind Over Media: Creative Thinking Skills for Electronic Media. New York, NY: McGraw-Hill; 1993.
8. Markenson D, DiMaggio C, Redlener I. Preparing health professions students for terrorism, disaster, and public health emergencies: core competencies. Acad Med. 2005;80(6):517-526.
9. Ferguson DA, Sweet DJ, Craig BJ. Forensic dentistry and dental hygiene: how can the dental hygienist contribute? Can J Dent Hyg. 2008;42(4):203-211.
10. Brannon RB, Connick CM. The role of the dental hygienist in mass disasters. J Forensic Sci. 2000;45(2):381-383.
11. Guay AH. The role dentists can play in mass casualty and disaster events. Dent Clin North Am. 2007;51(4):767-778.
12. Hinchliffe J. Forensic odontology, part 2: major disasters. Brit Dent J. 2011;210(6):271-273.
13. Rawson RD, Nelson BA, Koot AC. Mass disaster and the dental hygienist: the MGM fire. Dent Hyg (Chic). 1983;57(4):12-18.
14. Berketa J, James H, Lake A. Forensic odontology involvement in fatality victim identification. Forensic Sci Med Path. 2012;8(2):148-156.
15. Avon SL. Forensic odontology: the roles and responsibilities of the dentist. J Can Dent Assoc. 2004;70(7):453-458.
16. Gambhir R, Kappor D, Singh G, et al. Disaster management: role of dental professionals. Int J Med Sci Public Health. 2013;2(2):169-173.
17. Zohn HK, Dashkow S, Aschheim K, et al. The odontology victim identification skill assessment system. J Forensic Sci. 2010;55(3):788-791.
18. Petju M, Suteerayongprasert A, Thongpud R, Hassiri K. Importance of dental records for victim identification following the Indian Ocean tsunami disaster in Thailand. Public Health. 2007;121:251-257.
19. Meckfessel S, Stühmer C, Bormann K, et al. Introduction of e-learning in dental radiology reveals significantly improved results in final examination. J Craniomaxillofac Surg. 2011;39(1):40-48.
20. Mayer R. Multimedia Learning. 2nd ed. New York, NY: Cambridge University Press; 2004.
21. Mayer R, Fennell S, Farmer L, Campbell J. A personalization effect in multimedia learning: students learn better when words are in conversational style rather than formal style. J Edu Psychol. 2004;96(2):389-395.
22. Mayer R, Moreno R. A split-attention effect in multimedia learning: evidence for dual processing systems in working memory. J Edu Psychol. 1998;90:312-320.
23. Stegeman C, Zydney J. Effectiveness of multimedia instruction in health professions education compared to traditional instruction. J Dent Hyg. 2010;84(3):130-136.
24. Jonassen DH, Campbell JP, Davidson ME. Learning with media: restructuring the debate. Edu Tech Res Dev. 1994;42:31-39.