You must be signed in to read the rest of this article.
Registration on CDEWorld is free. Sign up today!
Forgot your password? Click Here!
INTRODUCTION
The prickling sensation of an appendage that “fell asleep” and the numbness that is experienced with dental anesthesia are not life-threatening. Numbness that occurs with no explanation and does not resolve quickly may indicate the presence of a serious underlying condition, especially if it occurs in the mandible. The medical literature reveals that chin numbness may be indicative of a more serious underlying condition, especially if cancer or the treatment of radiation or chemotherapy preceded the numbness.
Case Study
In September 2011, a 39-year-old woman, a non-smoker and rare drinker, presented to the University of Texas School of Dentistry for an adult prophylaxis. The patient complained of localized numbness to her lower left quadrant with slight discomfort, which she had experienced for approximately 2 weeks. She reported that she had been diagnosed with high-grade sarcoma in her left breast the previous year and had been treated with radiation therapy and chemotherapy, but she ultimately underwent a radical mastectomy in January 2011. A review of her chart revealed no report of any symptoms in the head and neck during her previous two dental visits since 2007. No remarkable findings were noted on either the medical history or intra/extraoral examinations. The patient’s last visit to the dental school was in July 2010. Her treatment plan consisted of an adult prophylaxis for her maxillary arch with localized scaling and root planing (SRP) for her mandible. The localized SRP was performed and the patient was scheduled to come back to complete treatment but never returned.
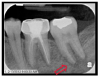
At the September 2011 appointment, significant findings in her intra/extraoral exam consisted of palpable lymph nodes across the left side of the mandible with numbness affecting the lip and chin, tenderness in the region of tooth No. 20, and redness with inflammation that was consistent with gingivitis. To diagnose the etiology of her numbness, a partial full-mouth series of radiographs were taken. No distinguishable carious lesions or apical lesions were noted; however, tooth No. 19 had a stainless steel restoration consistent with a history of endodontic treatment (Figure 1). To rule out other pathologic conditions, an oral pathologist ordered a panoramic image, which was interpreted by a dental radiologist. The radiograph revealed no signs of trauma or other sources to explain the etiology of the numbness. Idiopathic osteosclerosis in the right side of the mandible was present (Figure 2). A prophylaxis was performed and on a 3-week follow-up visit, her gingival tissue health improved but her symptoms still persisted. Recommending she should consult with her oncologist, her treating physician found no evidence of any recurring malignancy.
When the patient returned to the clinic 5 months later, additional radiographs were taken and interpreted by an oral pathologist revealing a “moth-eaten” radiolucent lesion of apical resorption around tooth No. 18 (Figure 3 and Figure 4). The area was swollen and teeth Nos. 18 and 19 were tender to percussion. Further testing included a pulp vitality test to tooth No. 18 with a biopsy to the surrounding bone. A cone beam computed tomography scan was also recommended to rule out metastatic disease and intraosseous malignancy. Original differential diagnoses included acute apical abscess and subacute osteomyelitis but after a biopsy the differential diagnoses expanded to myofibroma, lipoma, adenoma, adenocarcinoma, lymphoma and sarcoma. Ultimately, the lesion was described as a malignant spindle tumor compatible with myofibroblastic sarcoma. The patient was referred to a local hospital for treatment, which included surgery to remove the mass, affected tissues, and all portions of diseased bone within the left side of mandible. However, the patient lived for approximately 1 year after surgery, dying 19 months after the onset of chin numbness.
Mental Nerve Neuropathy/Numb Chin Syndrome
Mental nerve neuropathy, better known as numb chin syndrome, is a rare condition with one of the first documented cases reported in the early 1800s by Charles Bell in a patient with breast cancer.1,2 Since then, studies have reported a positive correlation linking neuropathies of the mental nerve to metastatic cancers. The most notable are recurrent cancers in the breast, lung and prostate, as well as leukemia and lymphoma; however, the strongest relationship with numb chin syndrome has been with breast cancer and lymphoma.1-4 Research indicates a high number of instances where chin numbness runs parallel with the progression of or relapses in the aforementioned cancers. A systematic review by Galán-Gil et al reported 136 documented numb chin syndrome cases showing that numb chin syndrome has the greatest correlation with breast cancer (40.4%) followed by lymphoma (20.5%).3 This relationship is of importance to dentistry because the oral cavity is often sensitive to internal changes and will display signs of an obscure systemic disease long before it is discovered. It is important for clinicians to be thorough when reviewing a patient’s medical history and while doing an intra/extraoral exam. One study found that in 47% of cases where numb chin syndrome was detected, the syndrome preceded the diagnosis of malignancy and in 30% of the cases examined, neuropathies preceded relapses of malignancies.5 Unfortunately, in the instances where numb chin syndrome was detected and associated with cancer, the survival rate was poor. Statistics reveal that life expectancy is less than 12 months from the date of diagnosis.2,5-7 It is critical for dental professionals to be cognizant and acknowledge possible symptoms of numb chin syndrome in patients, especially for those with a history of cancer.
Clinical Presentation
Numb chin syndrome normally presents as unilateral numbness along the lip and chin with patients describing effects feeling similar to local anesthesia.2,7,8 The functions of the lip and tongue, such as movement and taste, may appear normal.9,10 Diagnostic dental radiographs may not indicate an etiologic source.6,10 In circumstances where a patient reports symptoms of numbness without an identifiable source, a referral to a specialist for further medical examination should be considered.
Patient Considerations and Diagnostic Tests
There are several factors to consider if numb chin syndrome is suspected. In numerous case studies, diagnostic dental radiographs found no correlation to the etiologic pathology of the symptoms to paraesthesia. In a case report by Ryba et al, a 58-year-old edentulous man described an abrupt onset of localized numbness to the lower left side of his mandible.7 Although no significant abnormalities in dental radiographs or oral examination were found, neurological tests exposed disturbances in the inferior and mental nerve, and blood tests revealed signs of widespread metastatic disease.7 In another report, a 56-year-old woman who presented with a 3-month cough, shortness of breath and bone pain, indicated a tingling sensation in the lower right region of her mouth. No tangible abnormalities within the lymph nodes or neurologic evidence were described. However, a computed tomography (CT) scan discovered a mass in the patient’s lung along with multiple liver metastases and bone marrow involvement. Radiographs of the cervical area and the CT scan of the mandible revealed no defects within either region.5 In respect to other cases reviewed for this article, the patients’ initial dental radiographs were the least useful in determining an early diagnosis; cases that presented radiolucent lesions were in later stages of an already manifesting disease.
Prescriptions are meant to treat common dental problems; however, when antibiotics and medications have limited or no effect in treating numbness, clinicians should view this lack of response as a sign of urgency.2,8,11 This was the case of a 37-year-old man with no prior symptoms who experienced pain in the lower jaw after an adult prophylaxis. The patient was treated with erythromycin for 5 days, which failed to alleviate what was thought to be a dental infection. Findings from his magnetic resonance imaging (MRI) were within normal limits; however, this condition persisted and later, after he developed a fever, blood tests and a bone marrow biopsy verified that the underlying condition was lymphoma.2 In another case, a 48-year-old woman with diabetes was seen by her physician to treat her symptoms of numbness and tingling to the lower right side of her lip and chin. Prednisone was prescribed to relieve her symptoms, both of which returned about a month later. The woman’s neurological exam and MRI appeared normal but blood tests and a bone marrow biopsy revealed lymphoma.2 These cases illustrate why additional testing and evaluation are essential for proper diagnosis.
Other Diagnostic Tests
Blood and neurological tests are useful in detecting underlying conditions and diseases associated with numb chin syndrome.2,5-7,11,12 Useful diagnostic tools are MRI and CT scans, with CT scans most widely used.1,4,5,8,9,11-13 An additional test referenced in studies is the touch and pain test which is relatively simple to execute with an explorer or small brush on the soft tissues. The test helps to diagnose the extent of manifesting numbness by comparing the affected region to a non-affected area.10 Another notable test is the technetium Tc 99m methylene diphosphonate bone scan, which uses a radioactive intravenous imaging agent to locate the sites of possible lesions.10 Of note, in all of the cases reviewed in this paper, a combination of tests were used to determine a diagnosis. Because neuropathies have the tendency to imitate tooth pain, multiple tests may be recommended to form an accurate diagnosis.8 A misdiagnosis could cause a dangerous delay in suitable treatment.
Differential Diagnosis and Other Possible Causes to Numbness
Typical sources of paresthesia or numbness frequently have dental origins. These include, but are not limited to, iatrogenic causes such as trauma to the mandible, damage to the nerve from extractions, mandibular surgery, ill-fitting dentures and implants.8,9 In these cases, the aforementioned are likely to cause injuries to the nerves of the ramus and cause hypoesthesia. Other causes may arise from benign tumors, radiotherapy, bone infection (osteomyelitis) and dental abscesses partly due to infection imposing or compressing on the nerve (Table I).7-9
Chronic systemic disorders such as diabetes or demyelinating disorders such as multiple sclerosis can lead to neuropathies and nerve damage. Possible sources of nerve damage in diabetes include high blood glucose levels, abnormal blood fat levels and inflammation caused by the autoimmune response.14 Similar findings of chin numbness have also been associated with multiple sclerosis. These cranial nerve palsies involve several cranial nerves (CN), including CN III (oculomotor), CN VI (abducens) and CN V (trigeminal), not limited to the mandibular nerve alone.13
Conclusion
Healthcare professionals who encounter patients reporting chin numbness should not underestimate the significance of this symptom. Because many dental professionals are unaware of numb chin syndrome and its links to serious underlying systemic conditions, unnecessary dental treatment may be recommended with little or no improvement. A patient’s medical history proves to be an essential part of every visit. Dental professionals should further investigate patients who present symptoms of chin numbness, especially when cancer or the treatment of cancer was ever a part of their history. Unexplained numbness is not a normal symptom, and consultation with other medical experts may provide needed answers. Having the ability to recognize numb chin syndrome, or mental nerve neuropathy, as a possible indicator to serious disease is important for the health and the potential survival of a patient.
About the Author
Norma J. Chapa, RDH, BSDH, is a clinical hygienist in a general private practice in Southeast Texas that also specializes in oral pathology.
Acknowledgments
A special expression of thanks to Donna Warren-Morris, her guidance and mentorship helped facilitate the article. Also, a notable extension of appreciation and recognition to Jeffery Chen, Marcey McLawchlin, and Kim Anh Thi Nguyen-Garrett for all the hard work that was put into collecting the materials that led to producing this manuscript.
References
1. Colella G, Giudice A, Siniscalchi G, et al. Chin numbness: a symptom that should not be underestimated: a review of 12 cases. Amer J Med Sci. 2009;337(6):407-410.
2. Faltas B, Phatak P, Sham R. Mental nerve neuropathy: frequently overlooked clinical sign of hematologic malignancies. Am J Med. 2011;124(1):e1-e2.
3. Galán Gil S, Peñarrocha Diago M, Peñarrocha Diago M. Malignant mental nerve neuropathy: systematic review. Med Oral Patol Oral Cir Bucal. 2008;13(10):e616-e621.
4. Turner-Iannacci A, Mozaffari E, Stoopler ET. Mental nerve neuropathy: case report and review. CJEM. 2003;5(4):259-262.
5. Laurencet FM, Anchisi S, Tullen E, Dietrich PY. Mental neuropathy: report of five cases and re¬view of the literature. Crit Rev Oncol Hematol. 2000;34(1):71-79.
6. Baskaran RK, Krishnamoorthy, Smith M. Numb chin syndrome—a reflection of systemic malignancy. World J Surg Oncol. 2006;4:52.
7. Ryba F, Rice S, Hutchison IL. Numb chin syndrome: an ominous clinical sign. Br Dent J. 2010;208(7):283-285.
8. Divya KS, Moran NA, Atkin PA. Numb chin syndrome: a case series and discussion. Br Dent J. 2010;208(4):157-160.
9. Bar-Ziv J, Slasky BS. CT imaging of mental nerve neuropathy: the numb chin syndrome. AJR Am J Roentgenol. 1997;168(2):371-376.
10. Yoshioka I, Shiiba S, Tanaka T, et al. The importance of clinical features and computed tomographic findings in numb chin syndrome: a report of two cases. J Am Dent Assoc. 2009;140(5):550-554.
11. Ray A, Skoura T, Scherer W. Numb chin syndrome: dental treatment implications. N Y State Dent J. 2011;77(2):28-29.
12. López-Cortés LE, Vera JA, Merino de L, et al. Numb chin syndrome: a warning sign of aggressive b-cell malignancy. Leuk Res. 2011;35(9):e177-e178.
13. Khandaghi R, Arami MA. “Numb chin” as the first and sole presenting sign of multiple sclerosis. Arch Iran Med. 2005;8(1):60-62.
14. National Institute of Diabetes and Digestive and Kidney Diseases. Diabetic neuropathies: the nerve damage of diabetes. National Institutes of Health. 2009.