You must be signed in to read the rest of this article.
Registration on CDEWorld is free. Sign up today!
Forgot your password? Click Here!
A dental patient is scheduled who has recently been diagnosed with cancer and about to begin chemotherapy. Are you prepared to provide the highest standard of care for this individual? The intent of this article is to provide the dental hygienist and dentist with an evidence-based dental treatment model, as part of a collaborative interdisciplinary oncology team, for patients scheduled for chemotherapy. This review emphasizes the significance of pre-dental evaluation/treatment prior to chemotherapy. An evidence-based protocol for dental care with specific treatment modalities, including the prevention and treatment of oral mucositis (OM), is included.
An individual’s diagnosis of cancer is followed by a plethora of information regarding prognosis and treatment options. The patient and/or caregivers are responsible for making critical decisions during a highly emotional time. The necessity of a dental evaluation and dental treatment prior to beginning chemotherapy is perceived as secondary following the diagnosis of a potentially life-threatening disease.1,2
Cancer treatment is no longer exclusively delivered in large cancer centers staffed by multidisciplinary teams including dental oncology. A dental oncologist is often not included in the decision making prior to cancer therapy. Dental evaluation and treatment prior to chemotherapy and/or radiotherapy is the most beneficial period for the patient to seek dental treatment. The main objective of pre-chemotherapy dental treatment is to reduce the metabolic activity of the oral microflora and to prevent or reduce discomfort associated with oral mucositis (OM).3-7 Reducing the amount of microorganisms decreases the likelihood of secondary infections of the primary oral lesions.
Collaboration amongst various healthcare disciplines is becoming a necessity in our rapidly changing healthcare system. Patient-centered care requires the expertise of team members from a variety of disciplines including dental oncology, who communicate with one another in order to provide optimal care to all patients. Dental hygienists and dentists must be a part of this collaborative team and develop evidence-based protocols that outline dental treatment for various types of cancer.
Oral Care for the Cancer Patient
Cancer patients often are not referred for a dental evaluation prior to the commencement of cancer therapy. Oncologists express concern that the scheduling of a dental treatment may delay the commencement of cancer therapy.2 It has been documented that periodontal pathogens normally associated with infections in myelosuppressed cancer patients, as well as indigenous oral flora, are associated with acute periodontal infections during granulocytopenia.3 This finding is significant in that the oral cavity has not commonly been recognized as a source of acute infection in these individuals. Infected and inflamed periodontium can act as a focus for systemic infection in someone with neutropenic cancer. Conversely, severe mucositis lesions may lead to temporary or permanent treatment discontinuation and compromised cancer control.6,8 It is the responsibility of dental healthcare providers to prioritize dental treatment for individuals with cancer so they can begin cancer therapy as soon as possible. Assessment of the patient’s periodontal condition prior to the onset of profound neutropenia is critical for the diagnosis and management of these potentially life-threatening infections.3 A pre-treatment assessment would assist oncologists with information regarding potential sources of infection prior to severe myelosuppression, especially when time does not permit dental treatment prior to cancer therapy.4
In the absence of a dental oncologist, patients should be advised to visit their dental healthcare providers for a pre-screening prior to chemotherapy. It is the responsibility of the dental hygienist to educate patients on the adverse oral side effects of chemotherapy including mucositis. Patient education must also include discussion regarding the critical need to eliminate existing/potential areas of oral infection prior to chemotherapy. Some oral complications can be controlled through pre-therapy modification of potential dental and periodontal foci for infection. Mucosal ulcerations may become portals for the invasion of pathogens that can result in a life-threatening situation during periods of myelosuppresion.3-6 Dentistry is a vital component of the collaborative multidisciplinary oncology team. Communication amongst members of multidisciplinary teams is imperative in order to provide the highest standard of patient care.
An Evidence-Based Oral Health Protocol Model for the Dental Hygienist
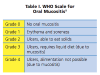
Table I and Table II are assessment tools to classify the severity of mucositis lesions and the standard grading scale for adverse events, respectively. Table III through Table VI provide the dental hygienist and dentist with an oral health treatment protocol for the chemotherapy patient. Every aspect of care must be evaluated and documented for the purpose of establishing outcomes. This information must be shared with other members of the collaborative multidisciplinary team.
Mucositis and Other Forms of Stomatitis
Mucositis is defined as inflammation of the oral mucosa caused by destruction of oral mucosa epithelium and suppression of its growth due to the effects of chemotherapy and/or radiotherapy. The direct cytotoxic effects on epithelial cells result in ulceration of mucosal lining of the oral cavity, pharynx, esophagus, and gastrointestinal tract. The buccal and labial mucosa, tongue, floor of the mouth, and soft palate are the areas most frequently affected. Clinical oral mucositis typically begins 5 to 10 days following initiation of chemotherapy and lasts 7 to 14 days.6-7,18 Oral complications include saliva changes, taste alterations, infection, and bleeding; late toxicities include mucosal atrophy and xerostomia. Many protocols have been proposed to prevent or reduce the severity of oral mucositis, but no treatment modality is yet known to be a definite prophylactic agent.
Final decisions regarding dental treatment during cancer therapy are made by multidisciplinary teams including dental oncologists. The risks and benefits of all options must be weighed against the overall well-being of the patient.
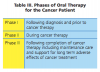
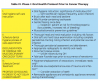
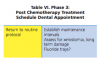
Table IV through VI outline dental treatment phases based on chemotherapy treatment. The goal of initial dental treatment prior to cancer therapy is to eliminate any preexisting acute and chronic pathological conditions. It is recommended that the patient’s oral health status be stabilized/optimized for minimally predictable complications during cancer therapy.6,7,9
Summary
The dental hygienist and dentist are vital to the collaborative multidisciplinary oncology team. Oncologists and individuals diagnosed with cancer must be informed regarding the significance of pre-dental evaluation/treatment prior to the commencement of cancer therapy. Priority must be given when scheduling these patients for dental evaluation/treatment in order to begin cancer therapy without delay. An evidence-based protocol for dental treatment must be in place in order to provide the highest standard of care to individuals with cancer. It is well documented that compromised oral health, prior to and during cancer therapy, dramatically affects treatment outcomes during periods of myelosuppression resulting from cancer therapy.
About the Author
Joanne C. Fletcher RDH, MS, is the 2010 recipient of the Johnson & Johnson/ADHA Excellence in Dental Hygiene Award and the founding dental hygiene director of Collin College in McKinney, Texas. She is a graduate of the Fones School of Dental Hygiene, University of Bridgeport, and was a Fones faculty member for 20 years. She had been a member of the Journal of Dental Hygiene Editorial Review Board for 25 years, member of the Dental Hygiene II National Board Test Construction Committee for 5 years, a dental hygiene accreditation consultant for the Commission on Dental Accreditation the past 17 years and a past president of the Connecticut Dental Hygienists’ Association. She is professor of periodontology, nutrition, radiology, oral medicine, and research at Collin College. This article is dedicated to the memory of her 16-year-old grandson, Drew Ducatelli.
References
1. Miller M, Kearney N. Oral care for patients with cancer: a review of the literature. Cancer Nursing. 2001;24(4):241-254.
2. Barker GJ, Epstein JB, Williams KB, et al. Current practice and knowledge of oral care for cancer patients: a survey of supportive health care providers. Support Care Cancer. 2005;13(1):32-41.
3. Dodd MJ, Dibble SL, Miaskowski C, et al. Randomized clinical trial of the effectiveness of 3 commonly used mouthwashes to treat chemotherapy-induced mucositis. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2000;90:39-47.
4. Raber-Durlacher JE, Epstein JB, Raber J, et al. Periodontal infections in cancer patients treated with high-dose chemotherapy. Support Care Cancer. 2002;10:466-473.
5. Peterson DE, Minah GE, Overholser CD, et al. Microbiology of acute periodontal infection in myelosuppressed cancer patients. J Clin Oncol. 1987;5(9):1461-1468.
6. Rankin K, Epstein J, Huber M, et al. Oral health care in cancer therapy. 2009;126(5):389-397, 406-419, 422-437.
7. Plemons JM, Rankin KV, Benton E. Oral health care in cancer patients: you can make a difference. Tex Dent J. 2013;130(8):682-690.
8. Campos Ines Da Cruz, Campos CN, Aarestrup FM, Aarestrup BJV. Oral mucositis in cancer treatment: Natural history, prevention and treatment. Mol Clin Oncol. 2014;2(3):337-440.
9. World Health Organization (WHO). Handbook for reporting results of cancer treatment. 1979. Available at: http://whqlibdoc.who.int/publications/9241700483.pdf.
10. National Cancer Institute. Common terminology criteria for adverse events (CTCAE). Available at: http://ctep.cancer.gov/protocolDevelopment/electronic_applications/ctc.htm.
11. Wilberg P, Hjermstad MJ, Ottesen S, Herlofson BB. Chemotherapy-associated oral sequelae in patients with cancers outside the head and neck region. J Pain Symptom Manage. 2014;48(6):1060-1069. doi: 10:1016/j.jpainsymman2014.02.009. Epub 2014 Apr 18.
12. Keefe DM, Schubert MM, Elting LS, et al. Updated clinical practice guidelines for the prevention and treatment of mucositis. Cancer. 2007;109:820-831.
13. El-Housseiny AA, Saleh SM, El-Masry AA, Allam AA. The effectiveness of vitamin ‘E’ in the treatment of oral mucositis in children receiving chemotherapy. J Clin Pediatr Dent. 2007;31(3):167-170.
14. Schubert MM, Jones DL. Management of oropharyngeal mucositis pain. Texas Dent J. 2010;127(5):463-481.
15. Kokako I, Long L, Hodgkinson B, Evans D. The effectiveness of strategies for preventing and treating chemotherapy and radiation induced oral mucositis in patients with cancer: a systematic review. The Joanna Briggs Institute for Evidence Based Nursing and Midwifery. 1998:2. Available at: www.joannabriggslibrary.org/index.php/jbisrir/article/view/398.
16. Peterson DE, Ohrn K, Bowen J, et al. Systematic review of oral cryotherapy for management of oral mucositis caused by cancer therapy. Support Care Cancer. 2013;21:327-332.
17. Alvarino-Martin C, Sarrion-Perez M. Prevention and treatment of oral mucositis in patients receiving chemotherapy. J Clin Exp Dent. 2014;6(1):e74-e80.
18. Stokman MA, Spijkerver FK, Boezen HM, et al. Preventive intervention possibilities in radiotherapy- and chemotherapy-induced oral mucositis: results of meta-analyses. J Dent Res. 2006;85:690-700.
19. Gautam AP, Fernandes DJ, Vidyasagar MS, et al. Low level laser therapy for concurrent chemoradiotherapy induced oral mucositis in head and neck cancer patients-a triple blinded randomized controlled trial. Radiother Oncol. 2012;104:349-354.
20. Borrajo Loyes JL, Varela LG, Lopez Castro G, et al. Efficacy of chlorhexidine mouthrinses with and without alcohol: a clinical study. J Periodontol. 2002;73(3):317-321.
21. Mehdipour M, Taghavi Zenoz A. Mouthwashes in the prevention of chemotherapy-induced oral mucositis. DARU J Pharmaceutical Sci. 2011;19(1):71-73.
22. Barber C, Powell R, Ellis A, Hewett J. Comparing pain control and ability to eat and drink with standard therapy vs. Gelclair: a preliminary, double centre, randomised controlled trial on patients with radiotherapy-induced oral mucositis. Support Care Cancer. 2007;15:427-440.
23. Sonis ST. Efficacy of palifermin (keratinocyte growth factor-1) in the amelioration of oral mucositis. Core Evid. 2010;4:199-205.
24. Roopashri G, Jayanthi K. Radiotherapy and chemotherapy induced oral mucositis-prevention and current therapeutic modalities. IJDA. 2010;2(2):174-179.