You must be signed in to read the rest of this article.
Registration on CDEWorld is free. Sign up today!
Forgot your password? Click Here!
Introduction
Periodontal disease is a common, mixed oral infection affecting the supporting structures around the teeth. While 75% of the adult population has at least mild periodontal disease (gingivitis), 20%-30% exhibits the severe destructive form (chronic periodontitis).1 Characteristically, the disease is silent until the advanced stage when patients may report symptoms like swelling (abscess), discomfort, shifting of the dentition, or tooth mobility. The clinical signs of periodontitis emanate from inflammatory and destructive changes in the gingiva, connective tissues, alveolar bone, periodontal ligament, and root cementum. These signs include the formation of periodontal pockets, loss of clinical attachment, and resorption of alveolar bone.2
Accordingly, periodontitis begins with a pathogenic shift in the bacterial flora around teeth. Gram-negative organisms, such as Porphyromonas gingivalis, Tannerella forsythia, Treponema denticola and Aggregatibacter (formally Actinobacillus) actinomycetemcomitans, predominate in the subgingival space and organize as a biofilm.3 Several of the gram-negative bacteria in the biofilm are particularly important because they have been identified as red-complex bacteria (T. forsythia, P. gingivalis, and T. denticola) and have been linked with important parameters of periodontal diagnosis, such as pocket depth and bleeding on probing.3 This bacterial biofilm is in direct contact with host tissues along an ulcerated epithelial interface called a periodontal pocket. Locally, bacteria and their products (eg, lipopolysaccharide entotoxin) penetrate host periodontal tissues and stimulate host expression of inflammatory mediators like arachidonic acid metabolites (prostaglandin E2) and cytokines (interleukin-1).4 These mediators in turn trigger local inflammatory and destructive changes in the tissues.
Longitudinal population studies indicate that these destructive changes (disease progression) are not continuous over time but appear restricted to "random bursts" of activity confined to short intervals (6 months or less).5 Risk factors associated with progressive periodontitis include smoking, diabetes, obesity, poor plaque control, and certain genetic polymorphisms.6-10 In addition, residual or persistent deep probing depths are associated with periodontitis progression.11 Paulander and coworkers recently demonstrated that periodontitis subjects with moderate (4-5 mm) and deep (> 6 mm) probing depths were 2 to 3 times more likely to exhibit alveolar bone loss over 10 years.12 Similarly for tooth loss, the odds ratio for moderate pockets was 2.9 (95% CI, 1.9-4.2), and the odds for deep pockets was 4.2 (95% CI, 2.4-7.3). These data imply pocket depth reduction (or resolution) is a clinically important treatment goal to ensure stability and maintenance in patients.
Complementary Medical-Mechanical Treatment Model with Adjunctive Antimicrobials
Strategies for treating periodontitis principally focus on addressing the etiologic bacteria or biofilm.13,14 According to the mechanical model, the bacterial biofilm is disrupted and removed via scaling and root planing (SRP) procedures. These debridement procedures can be accomplished nonsurgically or surgically, and both approaches result in pocket depth (PD) reductions in patients.15,16 In addition, a number of adjunctive chemotherapeutic approaches have been developed, tested and approved for use in patients with chronic periodontitis (Table 1). These "locally delivered antimicrobials" follow a complementary medical-mechanical treatment model since they are used in combination with SRP for enhanced efficacy. These formulations typically couple an antimicrobial or antibiotic with a drug polymer that extends drug release within the periodontal pocket (controlled-release delivery).17
A recent systematic review and meta-analysis conducted by Hanes and coworkers demonstrated that adjunctive locally administered antimicrobials improved PD over SRP alone in chronic periodontitis patients.18 This group of investigators searched electronic databases and relevant dental journals and identified 32 clinical studies fitting selection criteria. The studies (28 randomized controlled clinical trials, 2 cohort, and 2 case-control studies) represented a variety of locally administered antimicrobials (eg, minocycline, doxycycline, tetracycline, metronidazole, and chlorhexidine formulations). The resulting meta-analysis indicated an overall significant reduction in PD with adjunctive local antimicrobials versus SRP alone. These findings strongly support the use of locally administered antimicrobials in combination with SRP in patients with chronic periodontitis, especially those at risk for disease progression.
The first local delivery system approved for use by the US Food and Drug Administration (FDA) was called Actisite® (ALZA Corporation, Palo Alto, Calif, USA) and was developed by Dr. Max Goodson in 1983.19 This product consisted of a nonresorbable polymer fiber of ethyl vinyl acetate containing tetracycline hydrochloride (25% or 12.7 mg). Each fiber (23 cm) was placed subgingivally similar to retraction cord. Since that time, clinicians have been introduced to second generation locally delivered antimicrobials that are easier to utilize and produce greater clinically significant results. Following is a discussion about the 3 products currently available in the United States.
Chlorhexidine Gluconate Chip
The PerioChip® (Dexcel Technologies Limited, Jerusalem, Israel) is a biodegradable gelatin-based polymer system containing the active antimicrobial, chlorhexidine gluconate (2.5 mg). Each chlorhexidine (CHX)-gelatin wafer or chip is placed subgingivally with cotton pliers. While pharmacokinetic studies indicate that chlorhexidine is released from the system for 7-10 days in periodontal pockets, microbial studies have shown suppression of the pocket flora for up to 11 weeks following CHX chip treatment.20,21 In the phase 3 clinical trials, CHX chip treatment plus SRP significantly reduced PD and maintained CAL at 9 months compared with SRP controls.22 Importantly, SRP was limited in these trials to one hour of ultrasonic scaling. In addition, retreatment with CHX chip occurred at 3 and 6 months at sites with residual pockets (> 5 mm). Nevertheless, after 9 months of adjunctive CHX chip treatment, no sites exhibited bone loss, and 25% of the sites exhibited bone gain as measured with subtraction radiography.23 In contrast, 15% of periodontal sites treated with SRP alone exhibited bone loss. Chlorhexidine gluconate chip has a documented safety profile, and unlike chlorhexidine mouthrinse, does not cause any visible staining of teeth.
Doxycycline Bioresorbable Gel
Atridox® (Atrix Laboratories, Fort Collins, Colo, USA) is a 10% formulation of doxycycline (50 mg) in a bioresorbable gel system (poly DL-lactide and N-methyl-2-pyrrolidone mixture). The system is supplied as 2 pre-filled syringes that are mixed chair-side and applied subgingivally to the base periodontal pockets using a syringe. The "flowable" polymer gel fills and conforms to pocket morphology, then solidifies to a wax-like consistency upon contact with gingival crevicular fluid. Doxycycline is released at effective concentrations over 7 days, and significant reductions (60%) in anaerobic pathogens are sustained for up to 6 months posttreatment.24,25 In subjects with chronic periodontitis, the application of doxycycline gel (at baseline and 4 months later) reduced PD (1.3 mm) and improved CAL (0.8 mm) comparable to SRP alone at 9 months following treatment.26 While current and former smokers within the trials did not respond as well to SRP alone, smoking status did not diminish the clinical improvements observed with doxycycline gel.27 While these studies demonstrated equivalency of doxycycline gel (monotherapy) with SRP and supported regulatory approval, this system like other locally delivered antimicrobials is conventionally used as an adjunct to SRP in clinical practice.
One phase 4 or postmarketing trial investigated the use of doxycycline gel as an adjunct to SRP and demonstrated incremental benefits when the system was used in combination with SRP.28 Accordingly, one arm of the adjunctive use trial involved initiating treatment with ultrasonic scaling plus doxycycline gel at baseline, and then isolated SRP at 3 months for those sites with residual pocketing (PD > 5 mm). The second arm of the study involved SRP alone at baseline, and then isolated ultrasonic scaling and doxycycline gel at those sites with residual pocketing. While both treatment strategies were equally effective at improving probing depths and clinical attachment levels over 6 months, responses were greater on average for the adjunctive doxycycline gel treatment at 3 months compared to SRP alone.
Minocycline Microspheres
Arestin® (OraPharma, Inc., Warminster, Pa, USA) is an approved local delivery system featuring 1mg of minocycline hydrochloride microencapsulated in resorbable polymer microspheres (polyglycolide-co-dl-lactide). The delivery system (cartridge and syringe) is designed for quick and easy administration of one unit dose of Arestin subgingivally in periodontal pockets measuring ≥ 5 mm with bleeding on probing (BOP) (Figure 1). With this system, minocycline hydrochloride is maintained within pockets for 21 days at concentrations effective against periodontal pathogens. The agent may also block collagenases that are implicated in host tissue breakdown.29
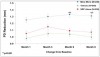
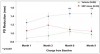
The pivotal clinical trials of minocycline microspheres involved approximately 750 subjects with generalized moderate to advanced chronic periodontitis recruited at 18 centers.30 Periodontitis subjects meeting inclusion criteria at baseline were randomized to 1 of 3 treatments: 1) scaling and root planing (SRP) alone (positive control); 2) SRP plus polymer vehicle (placebo control); or 3) SRP plus minocycline microspheres. Full mouth probing exams were performed at baseline (prior to treatment) and at 1, 3, 6, and 9 months. Figure 2 graphs mean probing depth reductions observed in the 9-month trial for all subjects (intent-to-treat population) in the primary analysis. Analyses of covariance adjusting for centers indicated significant-inter-group differences in probing depth reductions at all time points (p < 0.001). In particular, subjects treated with adjunctive minocycline microspheres exhibited significantly greater probing depth reductions as compared to control subjects treated with SRP alone. When smokers (Figure 3) or those with advanced periodontitis (mean baseline PD > 6 mm) (Figure 4), were considered in secondary analyses, again ANCOVA indicated significant probing depth reductions with adjunctive minocycline microspheres over control treatments.31 Indeed, inter-group differences in PD reduction were greater among advanced periodontitis subjects versus the overall population.
A priori, a shift in subject mean probing depth < 5 mm with treatment was considered a clinically relevant and "maintainable" response. When regression analyses were performed comparing response odds with adjunctive minocycline microspheres treatment versus SRP alone, the odds ratios for subjects who smoked or who had advanced periodontitis were 2.06 (95% CI 1.10, 3.85) and 2.86 (95% CI 1.45, 5.66), respectively.32 These data indicate that patients with advanced periodontitis or smokers are 2 to 3 times more likely to respond, and that this increase in odds is clinically relevant. Site analyses on pocket resolution (posttreatment PD < 5 mm) were also designated as meaningful. Again, a significantly and consistently higher percent of pockets were "resolved" with adjunctive minocycline microspheres versus SRP alone for all subjects and smokers, respectively (Table 2).33
A large, phase 4 (postmarketing) trial involving 2805 patients and 895 dentists was conducted to evaluate the use of minocycline microspheres in private practices throughout the United States.34 Accordingly, 1095 patients received 2 applications of minocycline microspheres (at baseline and 3 months) per protocol, and 1710 patients received only one minocycline microsphere application (at baseline). Mean 6-month pocket depth reductions were 1.82 and 1.94 mm for the patients receiving one and 2 minocycline microspheres treatments, respectively. Similar results were obtained in smokers, diabetic patients, and cardiovascular disease patients. After one minocycline microspheres treatment, 62% of sites had decreased to less than 5 mm, and after 2 treatments the corresponding proportion increased to 67%. This large private practice study demonstrated that minocycline microspheres plus SRP is effective in reducing pocket depth and that efficacy increased with retreatment (dose-response).
One recently published trial indicates that the effects of flap surgery may be enhanced with adjunctive minocycline microspheres treatment. Hellström and coworkers recruited 60 periodontitis patients and randomized them to either flap surgery plus minocycline microspheres therapy (baseline and weeks 2, 3, and 5) or surgery alone.35 At week 25, the mean PD reduction from baseline was 2.51 mm in the surgery plus minocycline microspheres (test) group versus 2.18 mm in the control group. Smokers in the test group had a significantly greater probing depth reduction (2.30 mm) as compared to smokers in the control group (2.05 mm). In addition, the number of sites with probing depth reductions of 2 mm or more was significantly higher in the test group than in the control group. Hence, minocycline microspheres may be adjuncts to both nonsurgical and surgical therapies for patients with moderate to severe, chronic periodontitis.
These efficacy findings for minocycline microspheres have been extended to peri-implantitis, an inflammatory process around one or more osseointegrated implants in function, resulting in a loss of supporting bone and associated with a similar pathogenic flora. Renvert and coworkers conducted a clinical trial in which 32 subjects with peri-implantitis (one implant with PD > 4 mm, bleeding and/or exudate on probing and the presence of putative pathogens) randomly received debridement plus minocycline microspheres or debridement plus chlorhexidine gel (0.2%) at baseline, 1 month, and 3 months.36 While both treatments reduced putative pathogens, adjunctive minocycline microsphere treatment resulted in significant improvements in PD compared to chlorhexidine gel at 1 month, 3 months, and 6 months. Significant reductions in bleeding on probing were also noted for up to 12 months. This investigative group published the results from a second trial with 30 peri-implantitis subjects. Again, adjunctive minocycline microspheres improved PD and bleeding scores, whereas the adjunctive use of chlorhexidine gel had limited effects on bleeding scores.37 Another investigative team, Salvi and coworkers, also noted consistent efficacy with minocycline microspheres for treating peri-implantitis.38 Here, the investigators applied minocycline microspheres to implant sites exhibiting bone loss and PD > 5 mm following a 3-week debridement and hygiene interval. While 6 of 31 implants were either rescued or exited from the trial because of persistent peri-implantitis, all other implants (80.6%) showed significant reduction in both PD and BOP over 12 months with minocycline microspheres therapy. The investigators also examined peri-implant microflora using DNA-DNA checkerboard hybridization techniques and observed significant reductions in A. actinomycetemcomitans at 12 months and reductions in "red complex" bacteria (T. forsythia, P. gingivalis, and T. denticola) for 6 months.39 Binary regression analysis showed that the clinical parameters and smoking history could not discriminate between successfully treated and rescued/exited implants at any observation time point. In addition, failures in treatment could not be associated with the presence of specific pathogens or by the total bacterial load at baseline. Collectively, these new data indicate improvements in the clinical signs of peri-implantitis over 12 months with adjunctive locally administered minocycline.
Goodson and coworkers conducted a clinical trial utilizing 124 subjects with moderate to advanced chronic periodontitis. Subjects were randomly assigned to either SRP alone or minocycline microspheres and SRP. All patients received full-mouth SRP at baseline, followed by treatment with minocycline microspheres if assigned to the SRP and minocycline microspheres group. The examiner was blinded to the patient's treatment. Clinical assessments were made and plaque samples were collected at baseline and at Day 30. The results demonstrated that adjunctive minocycline microspheres significantly reduced red-complex periodontal pathogens as compared to SRP alone by one month.40
Another investigation conducted by Oringer et al41 investigated the effect of minocycline microspheres on gingival crevicular fluid (GCF) levels pyridinoline cross-linked carboxy-terminal telopeptide of type I collagen (ICTP) and interleukin 1-beta (IL-1). ICTP is a bone-specific degradation product and IL-1 is a potent bone-resorptive cytokine. Forty eight periodontitis patients were randomized to receive SRP followed by minocycline microspheres or vehicle. Eight healthy individuals served as a control group. Results found a potent short term reduction of ICTP and IL-1 in the SRP plus minocycline microspheres group.
Summary and Conclusions
Residual or persistent periodontal inflammation is associated with instability of dental tissues (periodontal disease progression and tooth loss). Cumulative data from clinical trials and meta-analyses support a complementary medical-mechanical model using locally delivered antimicrobials for treating chronic periodontitis. Overall, the clinical evidence accrued to date consistently shows that when locally administered antimicrobials are used adjunctively, significantly greater PD reductions and/or attachment level gains occur in patients. These responses are clinically relevant because they are accompanied by a greater likelihood for patient maintenance or pocket resolution. Recent trials also indicate that locally administered antimicrobials may enhance the effects of periodontal surgical therapy and may reduce the signs of peri-implantitis. The consistency of these findings supports the use of locally administered antimicrobials for managing dental patients with chronic periodontitis.
Clinical Implications
- Recent clinical trials indicate that locally administered antimicrobials may enhance the effects of periodontal surgical therapy and may reduce the signs of peri-implantitis.
- Patients with periodontitis exhibiting moderate (4-5mm) and deep (≥ 6 mm) probing depths were 2 to 3 times more likely to exhibit alveolar bone loss over 10 years.
- A systematic review and meta-analysis demonstrated that adjunctive locally administered antimicrobials improved PD over SRP alone in chronic periodontitis patients.
- Patients with advanced periodontitis or smokers are 2 to 3 times more likely to respond to SRP + minocycline microspheres than to SRP alone.
- se of minocycline microspheres has been shown to be advantageous when used as an adjunctive therapy to both nonsurgical and surgical therapies in patients with moderate to severe, chronic periodontitis.
- Adjunctive use of minocycline microspheres has shown a reduction in red-complex periodontal pathogens as compared to SRP alone.
Disclosure
Dr. Paquette has served as a scientific consultant and investigator for OraPharma, Inc. Dr. Ryan and Ms. Wilder are scientific consultants for Orapharma, Inc.
References
1. Albandar J, Brunelle JA, Kingman A. Destructive periodontal disease in adults 30 years of age and older in the United States, 1988-1994. J Periodontol 1999;70:13-29.
2. Flemmig TF. Periodontitis. Ann Periodontol 1999;4:32-38.
3. Socransky SS, Haffajee AD. Periodontal microbial ecology. Periodontol 2000 2005;38:135-187.
4. Offenbacher S. Periodontal diseases: pathogenesis. Ann Periodontol 1996;1:821-878.
5. Socransky SS, Haffajee AD, Goodson JM, Lindhe J. New concepts of destructive periodontal disease. J Clin Periodontol 1984; 11:21-32.
6. American Academy of Periodontology Research, Science and Therapy Committee. Tobacco use and the periodontal patient. J Periodontol 1999;70: 1419-1427.
7. Grossi SG, Genco RJ. Periodontal disease and diabetes mellitus: a two-way relationship. Ann Periodontol 1998;3:51-61.
8. Saito T, Shimazaki Y, Sakamoto M. Obesity and periodontitis. N Eng J Med. 1998;482-483.
9. Ramfjord SP, Morrison EC, Burgett FG, Nissle RR, Shick RA, Zann GJ, Knowles JW. Oral hygiene and maintenance of periodontal support. J Periodontol 1982;53:26-30.
10. Kornman KS, Crane A, Wang HY, di Giovine FS, Newman MG, Pirk FW, Wilson TG Jr et al. The interleukin-1 genotype as a severity factor in adult periodontal disease. J Clin Periodontol 1997;24:72-77.
11. Halazonetis TD, Haffajee AD, Socransky SS. Relationship of clinical parameters to attachment loss in subsets of subjects with destructive periodontal diseases. J Clin Periodontol 1989;16:563-568.
12. Paulander J, Axelsson P, Lindhe J, Wennstrom J. Intra-oral pattern of tooth and periodontal bone loss between the age of 50 and 60 years. A longitudinal prospective study. Acta Odontol Scand 2004;62:214-222.
13. American Academy of Periodontology. Parameter on chronic periodontitis with slight to moderate loss of periodontal support. J Periodontol 2000;71:853-855.
14. American Academy of Periodontology. Parameter on chronic periodontitis with advanced loss of periodontal support. J Periodontol 2000;71:856-858.
15. Cobb CM. Non-surgical pocket therapy: Mechanical. Ann Periodontol 1996;1:450-490.
16. Palcanis KG. Surgical pocket therapy. Ann Periodontol 1996;1:589-606.
17. Drisko CH. Nonsurgical pocket therapy: Pharmacotherapeutics. Ann Periodontol 1996;1:491-566.
18. Hanes PJ, Purvis JP, Gunsolley JC. Local anti-infective therapy: pharmacological agents. A systematic review. Ann Periodontol 2003;8:79-98.
19. Goodson JM, Holborow D, Dunn RL, Hogan P, Dunham S. Monolithic tetracycline-containing fibers for controlled delivery to periodontal pockets. J Periodontol 1983; 54:575-579.
20. Soskolne WA, Chajek T, Flashner M, Landau I, Stabholtz A, Kolatch B, Lerner EI. An in vivo study of the chlorhexidine release profile of the PerioChip in the gingival crevicular fluid, plasma and urine. J Clin Periodontol 1998;25:1017-1021.
21. Stabholz A, Sela MN, Friedman M, Golomb G, Soskolne A. Clinical and microbiological effects of sustained release chlorhexidine in periodontal pockets. J Clin Periodontol 1986;13:783-788.
22. Jeffcoat MK, Bray KS, Ciancio SG, Dentino AR, Fine DH, Gordon JM et al. Adjunctive use of a subgingival controlled-release chlorhexidine chip reduces probing depth and improves attachment level compared with scaling and root planing alone. J Periodontol 1998;69:989-997.
23. Jeffcoat MK, Palcanis KG, Weatherford TW, Reese M, Geurs NC, Flashner M. Use of a biodegradable chlorhexidine chip in the treatment of adult periodontitis: clinical and radiographic findings. J Periodontol 2000;71:256-262.
24. Stoller NH, Johnson LR, Trapnell S, Harrold CQ, Garrett S. The pharmacokinetic profile of a biodegradable controlled-release delivery system containing doxycycline compared to systemically delivered doxycycline in gingival crevicular fluid, saliva, and serum. J Periodontol 1998;69:1085-91.
25. Walker CB, Godowski KC, Borden L, Lennon J, Nango S, Stone C et al. The effects of sustained release doxycycline on the anaerobic flora and antibiotic-resistant patterns in subgingival plaque and saliva. J Periodontol 2000;71:768-774.
26. Garrett S, Johnson L, Drisko CH, Adams DF, Bandt C, Beiswanger B et al. Two multi-center studies evaluating locally delivered doxycycline hyclate, placebo control, oral hygiene, and scaling and root planing in the treatment of periodontitis. J Periodontol 1999;70:490-503.
27. Ryder MI, Pons B, Adams D, Beiswanger B, Blanco V, Bogle G et al. Effects of smoking on local delivery of con- trolled-release doxycycline as compared to scaling and root planing. J Clin Periodontol 1999;26:683-691.
28. Wennstrom JL, Newman HN, MacNeill SR, Killoy WJ, Griffiths GS, Gillam DG et al. Utilisation of locally delivered doxycycline in non-surgical treatment of chronic periodontitis. A comparative multi-centre trial of 2 treatment approaches. J Clin Periodontol 2001;28:753-761.
29. Oringer RJ, Al-Shammari KF, Aldredge WA, Iacono VJ, Eber RM, Wang HL, Berwald B et al. Effects of locally delivered minocycline microspheres on markers of bone resorption. J Periodontol 2002;73:835-842.
30. Williams R, Paquette D, Offenbacher S, Adams D, Armitage G, Bray K et al, Treatment of periodontitis by local administration of minocycline microspheres: a controlled trial. J Periodontol 2001;72:1535-1544.
31. Paquette DW, Oringer R, Lessem J, Offenbacher S, Genco R, Persson GR, Williams R. Locally delivered minocycline microspheres for the treatment of periodontitis in smokers. J Clin Periodontol 2003;30:787-794.
32. Paquette DW. Pocket depth reduction as an outcome measure of inflammation and soft tissue changes in Periodontitis trials. J Int Acad Periodontol 2005;7/4 (Supplement):147-156.
33. Paquette DW, Williams RC, Hanlon A, Lessem J. Clinical relevance of adjunctive minocycline microspheres in patients with chronic periodontitis: secondary analysis of a phase 3 trial. J Periodontol 2004;75:531-536.
34. Lessem J, Hanlon A. A post-marketing study of 2805 patients treated for periodontal disease with Arestin. J Int Acad Periodontol 2004;6:150-153.
35. Hellström MK, McClain PK, Schallhorn RG, Bellis L, Hanlon AL, Ramberg P. Local minocycline as an adjunct to surgical therapy in moderate to severe, chronic periodontitis. J Clin Periodontol 2008;35:525-31.
36. Renvert S, Lessem J, Dahlén G, Lindahl C, Svensson M. Topical minocycline microspheres versus topical chlorhexidine gel as an adjunct to mechanical debridement of incipient peri-implant infections: a randomized clinical trial. J Clin Periodontol 2006;33:362-9.
37. Renvert S, Lessem J, Dahlén G, Renvert H, Lindahl C. Mechanical and repeated antimicrobial therapy using a local drug delivery system in the treatment of peri-implantitis: a randomized clinical trial. J Periodontol 2008;79:836-44.
38. Salvi GE, Persson GR, Heitz-Mayfield LJ, Frei M, Lang NP. Adjunctive local antibiotic therapy in the treatment of peri-implantitis II: clinical and radiographic outcomes. Clin Oral Implants Res 2007;18:281-5.
39. Persson GR, Salvi GE, Heitz-Mayfield LJ, Lang NP. Antimicrobial therapy using a local drug delivery system (Arestin) in the treatment of peri-implantitis. I: Microbiological outcomes. Clin Oral Implants Res 2006;17:386-93.
40. Goodson JM, Gunsolley JC, Grossi SG, Bland PS, Otomo-Corgel J, Doherty F, Comiskey J. Minocycline HCl microspheres reduce red-complex bacteria in periodontal disease therapy. J Periodontol. 2007;78:1568-79.
41. Oringer RJ, Al-Shammari KF, Aldredge WA, Iacono VJ, Eber RM, Wang HL et al. Effects of locally delivered minocycline microspheres on markers of bone resorption. J Periodontol. 2002; 73:835-842.
About the Authors
David W. Paquette, DMD, MPH, DMSc, is an associate professor, graduate program director in Periodontology and assistant dean of graduate/advanced dental education at the University of North Carolina at Chapel Hill. He received his Doctor of Dental Medicine degree, Master of Public Health, Doctor of Medical Sciences, and Certificate in Periodontics from Harvard University. His current leadership roles include chairing the American Academy of Periodontology Subcommittee on Research Submissions and serving on the editorial boards for 6 journals. He also is a past president of the International Association for Dental Research Periodontology Research Group and is a past fellow with the American Dental Education Association (ADEA) Leadership Institute. He has published 45 articles and 2 book chapters relating to possible links between periodontal and systemic health and other issues related to periodontal disease. Dr. Paquette is an international speaker and consultant.
Maria Emanuel Ryan, DDS, PhD, a 1989 Stony Brook School of Dental Medicine graduate, is a tenured full professor in the Department of Oral Biology and Pathology at the School of Dental Medicine and a member of the Medical Staff at University Hospital at Stony Brook University Medical Center. She also serves as director of clinical research. Dr. Ryan is actively involved in teaching, practice, and research at the School of Dental Medicine. Dr. Ryan serves on several scientific, dental, and medical advisory boards. She is a nationally and internationally known speaker and author and has published over 75 original scholarly works.
Rebecca Wilder, RDH, BS, MS, is an associate professor and director of the Master of Science Degree program in Dental Hygiene Education at the University of North Carolina at Chapel Hill. She is also the director of faculty development for the UNC School of Dentistry. Ms. Wilder is the editor-in-chief of the Journal of Dental Hygiene and an author of Mosby's Dental Hygiene: Cases, Concepts and Competencies, published in 2008. She has published over 70 papers and 40 abstracts on oral health care issues. She is a consultant to the dental industry and is an international speaker in the areas of risk and practice management and periodontics.