You must be signed in to read the rest of this article.
Registration on CDEWorld is free. Sign up today!
Forgot your password? Click Here!
Overview of Diabetes Mellitus
Diabetes mellitus (DM) is a chronic, metabolic disease that is associated with high levels of blood glucose resulting from defects in insulin production, insulin action, or both. Recent statistics concerning this disease indicate 23.6 million people in the United States (US) have DM and another 57 million are estimated to have prediabetes. Approximately 25 percent of those with DM do not know they have the disease.1 According to the Centers for Disease Control and Prevention, those with DM represent an increase of more than 3 million in almost two years. Almost 8 percent of the US population has diabetes. The cost of diabetes totals $174 billion representing an increase of 32 percent since 2002.1
Diabetes can contribute to serious health complications and premature death. In 2006, DM was the seventh leading cause of death in the US and is considered to be underreported as a cause of death.1 Systemic complications associated with DM appear in Table 1. A relative perspective on a daily basis indicates that 4,100 people are diagnosed with diabetes, 230 amputations occur in people with diabetes, 120 people will enter end stage renal disease programs, 55 people will go blind, and 810 will die.2
There are three main types of DM: type 1, type 2, and gestational diabetes. Type 1 diabetes accounts for approximately 5 to 10% of all cases of DM. Although type 1 DM can occur at any age, it typically affects children and young adults. Caucasians tend to have the highest rates of this type of DM. Type 1 diabetes represents an autoimmune disease characterized by the marked inability of the pancreas to secrete insulin caused by an immunologically mediated destruction of β cells. These cells are the only ones that make the hormone insulin used to regulate blood glucose. Individuals are insulin-dependent and produce no endogenous insulin. If insulin is withdrawn, ketosis and eventually ketoacidosis develops. Ketoacidosis can occur rapidly leading to coma and death. Therefore, individuals with type 1 diabetes must have insulin to survive, which is usually delivered by injection or a pump.1,3
Type 2 DM accounts for approximately 90 to 95% of all cases of DM. This disease tends to occur in older individuals, but there appears to be a growing trend in adolescents and young adults due to obesity, physical inactivity and weight management.4,5 The racial/ethnic groups at particularly high risk for type 2 diabetes include African Americans, Hispanic/Latino Americans, American Indians and some Asian Americans, Native Hawaiians or Other Pacific Islanders. This form of DM usually begins as a form of peripheral insulin resistance associated with insulin secretory defect. Over time, the pancreas gradually loses its ability to produce insulin.1,3
Gestational diabetes is a form of glucose intolerance during pregnancy. It is more common among African Americans, Hispanic/Latino Americans, American Indians, obese women and those with a family history of diabetes. To avoid complications in the infant, the mother is treated with medication. Unfortunately, 5 to 10% of women with gestational diabetes develop type 2 DM immediately after pregnancy, and others have a 40 to 60% chance of developing DM in the next 5 to 10 years.1,6
There are three classic signs of DM. These include polyuria, polydispia and nocturia. Other more subtle signs and symptoms of DM include unexplained weight loss early in the disease stage, general fatigue, increased infections, leg cramps, parasthesia of the fingers and toes, impotence, and blurred vision. These symptoms may be overlooked for an extended period of time contributing to the high number of cases of DM that are undiagnosed. Risk factors for type 2 Dm appear in Table 2.
Diagnosing diabetes and prediabetes is based on clinical history, comprehensive examination, and blood glucose assays. A positive diagnostic test should be followed by a repeated test on a different day to confirm the clinical diagnosis. Diagnostic criteria for prediabetes and diabetes appear in Table 3. Examples of blood assays that can be performed to identify DM include random plasma glucose, fasting plasma glucose, oral glucose tolerance test, and glycosulated hemoglobin, also known as HgbA1c or A1c. The A1c test measures glucose control over time, usually reflecting blood glucose levels in the blood over 6 to 12 weeks prior to administration of the test. The A1c is a useful way for health care providers to determine if treatment protocols are effective, especially for those individuals who tend not to monitor their blood glucose regularly at home.5,7
Treatment of DM is multifaceted and includes oral medications and/or insulin, nutrition counseling, regular monitoring of blood glucose levels, regular exercise, targeted weight management, and in some cases, gastric bypass surgery or pancreatic transplant. Controlled trials have demonstrated that maintaining modest weight loss through sustained lifestyle interventions such as diet and physical activity reduces the incidence of type 2 DM in high-risk persons by 40 to 60 percent over 3 to 4 years. Blood pressure, cholesterol and other lipid control have also reduced diabetes complications. Lowering blood glucose reduced the risk of eye disease by 76 percent, kidney disease by 50 percent, and nerve disease by 60 percent.8-14 Treatment must be tailored to individual needs, lifestyle, culture, and personal values. A one-size-fits-all approach by health care providers has shown to be ineffective in helping people with diabetes improve their health.3,15
Because DM has reached epidemic proportions in the U.S., it is incumbent upon all health professionals to assess individuals carefully to identify those who are risk for this disease, to identify the disease in undiagnosed persons, and to assist those with DM in achieving optimum health. Individuals diagnosed with DM often struggle to adhere to recommended changes in diet, exercise programs, and medication management. Dental hygienists, dentists, optometrists, podiatrists, endocrinologists, diabetes educators and family care providers need to support them in their efforts and reinforce key concepts of diabetes care regularly to help them achieve successful health outcomes. Therefore, a collaborative approach among a variety of health care providers is recommended to support diabetes awareness, prevention, and management.
Health care providers representing the disciplines of Pharmacy, Podiatry, Optometry, and Dental Professionals (PPOD) of the National Diabetes Education Program (NDEP) have partnered to promote the concept of collaboration and referral to provide comprehensive diabetes care. This team created the document "Working Together to Manage Diabetes: A Guide for Pharmacy, Podiatry, Optometry, and Dental Professionals."16 Included with this document are a medication supplement, clinical images, and brochures that can be used for primary prevention for each discipline.
Key concepts related to eye care, foot care, oral care, and medication management based on these documents follow.
Optometry and Diabetes Mellitus
Diabetic retinopathy is a major public health concern in the United States, causing significant suffering, disability, loss of productivity and diminished quality of life. Diabetic retinopathy is the fourth most common cause of preventable vision loss in adults.17 Each day 55 Americans needlessly go blind from diabetes.2 There are multiple levels of diabetic retinopathy ranging from mild, moderate or severe nonproliferative diabetic retinopathy to proliferative diabetic retinopathy. Between 40 and 45 percent of all Americans diagnosed with diabetes have some level of retinopathy, while vision-threatening retinopathy develops in nearly 8 percent.18 Early detection leads to early treatment, which is important in reducing vision loss from this disease. With timely treatment and appropriate follow-up care, even people with advanced diabetic retinopathy can reduce the risk of blindness.
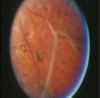
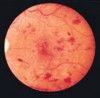
Diabetic retinopathy causes vision loss due to various diabetes-related changes in the eye. Damaged blood vessels from diabetic retinopathy cause fragile, abnormal blood vessels to develop. These new vessels (neovascularization) form when the normal retinal vessels no longer bring enough oxygen rich blood to the highly metabolic retina.19 Fragile vessels can leak blood, blocking light from reaching the retina, causing loss of vision. Fluid from these leaking blood vessels can also collect in the macula, the area of the retina responsible for central vision and fine acuity, causing swelling and blurring vision. Severe retinal neovascularization and fibrous proliferation can contract causing the retina to detach, which if left untreated leads to permanent blindness. Figures 1 and 2 demonstrate detached retina and diabetic retinopathy.
The development of retinopathy depends more on the length of time a person has diabetes and the degree of glycemic control rather than his or her age. People with type 1 diabetes are at a higher risk for developing vision-threatening diabetic retinopathy. However, retinopathy and vision-threatening retinopathy can also develop in people with type 2 diabetes who are not well controlled. The Diabetes Control and Complications Trial has shown that better control of blood sugar levels reduces the incidence of complications of diabetic retinopathy by 63 percent.19 Good control of blood glucose levels is important in delaying the onset and progression of diabetic retinopathy, and can reduce its severity.19-21 Other associated medical conditions known to worsen diabetic retinopathy, such as high blood pressure and high cholesterol, should also be controlled appropriately.19,20
Studies show that the early detection and treatment of diabetic retinopathy can prevent blindness.22-24 The Early Treatment Diabetic Retinopathy Study demonstrated a statistically significant reduction in severe vision loss for those eyes with early treatment.24 Diabetic retinopathy is most often treated with laser surgery, which seals leaking blood vessels or destroys abnormal ones. Laser treatment can reduce the onset and severity of vision loss and blindness due to diabetic retinopathy and macular edema. Pan retinal or scatter laser photocoagulation has been shown to reduce the risk of vision loss by 50 percent.24 Another form of laser treatment, focal laser therapy, can reduce the risk of vision loss in patients with significant macular edema.25 If a patient has blood in the center of the eye that will not resolve, a vitrectomy can be effective in restoring vision and reducing further vision loss.23 A vitrectomy is a surgical procedure that removes blood and replaces the gel in the center of the eye with a salt solution.
Diabetic retinopathy is asymptomatic at early stages. A comprehensive dilated eye exam is recommended soon after diagnosis of diabetes with annual dilated exams thereafter to check for early signs of diabetic retinopathy. People with diabetic retinopathy may need an eye exam more often. The goal is to detect diabetic retinopathy before obvious symptoms develop. Although treatments have high success rates, they do not cure diabetic retinopathy. Vision that has already been lost can rarely be restored. Diagnosing the disease early is the best way to prevent permanent vision loss. With early and timely treatment and appropriate follow-up care, even people with advanced diabetic retinopathy can reduce the risk of blindness by 90 percent.24 People with diabetes must be made aware that a test for visual acuity, such as for glasses or a driver's license, will not detect sight-threatening retinopathy. Instead, people with diabetes should see an optometrist or ophthalmologist for a comprehensive dilated eye examination.
Podiatry and Diabetes Mellitus
Complications from DM include serious foot problems that can lead to lower extremity amputations and long-term disability. Plantar ulceration has been reported as the most frequently common diabetic foot complication with 20%-25% of all hospital admissions owing to foot problems.26 The average hospital stay for foot related conditions has been an average of 26 days.27 Approximately 15% of people with diabetes will develop foot ulceration during their lifetime.28,29 Therefore, foot complications are a financial burden for healthcare.
Numerous factors lead to diabetic foot complications. The most single important risk factor for foot complication is neuropathy. Neuropathy in combination with deformity such as hammertoes will lead to ulceration. Peripheral vascular disease adds to the equation poor wound healing, which will lead to infection and gangrene. Figure 3 provides an example of neuropathy and infection. Routine foot care and the foot examination are extremely important in preventing complications. Health care providers should look for risk factors leading to the diabetic foot problems including peripheral neuropathy. Patients should be counseled on the risk of developing neuropathy. About 80% of all patients with diabetes experience lack of sensation that is combined with repetitive stress with tissue break down and then eventually infection.30 Patients with diabetic neuropathy alone are 1.7 times more likely to develop pedal ulcerations and are 12.1 times more likely to have foot deformities.31 The etiology of diabetic neuropathy is not clearly understood, but one major theory has been described as angiopathy of the vasa nervosum causing ischemia of the nerve. Evidence of the metabolic disturbance has been found, including the accumulation of intraneural sorbitol and glycosilation of the nerve protein and reduction of axonal transport. Loss of protective sensation, combined with recurrent trauma, is the primary mechanism of foot breakdown. The neurological exam evaluates for deficiencies in sensation. Testing involves the use of a Semmes-Weinstein 5.07 (10-g) monofilament and 128-Hz tuning fork. Both instruments have been validated identifying patients at risk for ulcers.
It is also imperative to assess the vascular status of individuals with diabetes. The Framingham study showed peripheral vascular disease is 2-3 times more likely to develop in the persons with diabetes than the general population.32 Peripheral vascular disease affects the femoral and iliac arterial systems in the same rates between diabetics and non-diabetics. However, persons with diabetes are more likely to have infra-popliteal vascular disease.33 The gold standard for assessing vascular disease is angiography. Non-invasive arterial studies can be performed to assess the vascular status of the patient as well as the potential for healing. These include ankle-brachial index (ABI), toe-brachial index, toe pressures and photoplethysmography. The use of ABI in diabetics is complicated by calcification of vessels (MAC) or Monckeberg's sclerosis. This results in a "lead pipe" condition that may result in a falsely elevated blood pressure.
Foot ulcers can develop in any location of the foot. They are more common under the metatarsal heads, great toe, heel or other weight-bearing areas. Foot ulcers may also develop as a consequence of poor footwear fit creating undue pressures, frictions or irritants. The mechanism of injury is commonly described as moderate pressure with repetitive trauma in presence of neuropathy. Offloading is the key for healing the neuropathic ulceration. Different modalities exist to decrease pressure. Some of these are extra-depth shoes with inserts, off-the-shelf off loading braces, custom molded orthosis, and the total contact cast.34
Poor glycemic control has been associated with the predisposition of diabetic patients to infections. The presences of high levels of glucose in the bloodstream decrease the ability of leukocyte chemotaxis, and phagocytosis. In general, blood glucose of 250 or more place the patients in a compromised situation to develop an infection. Patients with an infected foot ulcer may have diminished signs of inflammatory reaction possibly due to peripheral neuropathy or ischemia. Many patients lack a fever, elevated white blood cell count, elevated sedimentation rate, and report no pain.35 Once there is a diagnosis of clinical infection, then microbiology is a useful tool to determine the causative agent once a clinical diagnosis of infection is made. The treatment option will be dependent upon if the infection is mild, moderate or severe. The decision to hospitalize a patient or not is the question that most physicians must address. Assessing the severity of the infection helps to determine the need for hospitalization, the potential necessity and timing of surgery, and the likelihood of amputation. As a general rule, mild diseases can be treated with oral antibiotics in the outpatient setting, whereas moderate and severe disease will usually require intravenous antibiotic therapy and hospitalization.36
According to the American Diabetes Association, patients diagnosed with diabetes need to have a foot exam yearly. Vascular and neurological exams are imperative to identify patients at risk. Those patients identified at risk for complications should have their feet checked between 3-6 months. Patients should be educated regarding foot health and shoe wear. Patients should be advised to inspect their feet daily, look for any area of redness, and call their physician if any abnormality is noticed.
Oral Health and Diabetes
In addition to eye and foot changes, there are multiple oral signs and symptoms associated with DM. These symptoms include xerostomia, burning mouth syndrome, abnormal wound healing, multiple carious lesions, candidal infection (Figure 4), acetone (fruity) breath, increased salivary viscosity and asymptomatic parotid gland swelling. These findings may be related to excessive loss of fluids through frequent urination, the altered response to infection, microvascular changes, and increased glucose concentrations in saliva.3,37,38
As noted in Table 1, periodontal disease is considered the sixth complication of DM.39 People with diabetes are two to three times more likely than persons without diabetes to have periodontal disease.40 Periodontal disease is more prevalent, progresses more rapidly, and is often more severe in those with both type 1 and type 2 diabetes.41 Research suggests that there is a bidirectional relationship between diabetes and periodontal disease. People with diabetes are more susceptible to periodontal disease. Likewise, the presence of periodontal disease may make glycemic control more difficult to achieve.42-45 Treatment of periodontal disease decreases periodontal inflammation. Evidence is accumulating to support periodontal treatment contributing to improvement of glycemic control.46
Signs of periodontal problems associated with DM include gingival proliferation, gingivitis, aggressive periodontitis, and periodontal abscesses (Figure 5). These periodontal changes reflect host-response abnormalities such as nonenzymatic glycation and oxidation, imbalance in lipid metabolism, altered collagen metabolism, and neutrophil dysfunction.47 Bacterial invasion of the gingival stimulates the formation of inflammatory mediators including interleukin-1, tumor necrosis factor- alpha (TNF-α), prostaglandins, and cytokines. These inflammatory mediators led to production and activation of enzymes that destroy gingival connective tissue and resorb bone. In periodontal disease among persons with diabetes, it appears as though there is an impairment to produce new bone after bone loss has occurred. The cytokines that stimulate loss of tissue, most notably TNF-α, may be responsible for killing cells that repair damaged connective tissue or bone. Further, there may be more TNF-α produced, which can lead to an even more limited ability to repair periodontal tissues.48
Drug Therapy Management
Drug therapy management is especially important for people with diabetes. These individuals may present with multiple diseases, take five or more medications daily, and have several health care providers. Comprehensive review of medications used and medical records, education of persons with diabetes to improve adherence with medication regimens, and an assessment of response to therapy helps to ensure timely interventions and continuity of care. More than 50 percent of those with chronic disorders do not take their medication properly. Particularly, over 60 percent of persons with diabetes do not adequately control their blood glucose. Further, of those treated for hypertension and dyslipidemia, 65 percent and 49 percent respectively were unable to reach target blood pressure and cholesterol levels.49 To improve these circumstances, medication therapy regimens must be consistently and carefully monitored. Correct use of medication improves health and reduces health costs.50-52
Individuals with DM may be recommended to take either oral medications, insulin, or both. Individualized drug regimens should be determined to reduce side effects and drug interactions. Many persons with DM take non-prescription medications, vitamins, herbal or other nutritional supplements, or topical and skin care products without recognizing that these medicinals may interact with their diabetes medication. One study reported that over 57 percent of people with diabetes use complementary and alternative therapies.53 Therefore, pharmacists can advise these individuals on potential interactions, appropriateness of use based on complaint or need, and precautions and contraindications.
Another challenge for many persons with DM is regular use of a blood glucose meter. Self-monitoring blood glucose is an important way to assess the effectiveness of therapy, yet some individuals find it difficult to use the device itself or do not adhere to health care provider recommendations for regular use. Pharmacists can provide training on how to use a blood glucose meter, the results, actions to take, and when to seek help. In addition, pharmacists can offer information on ways to decrease costs of medications and supplies.
Oral health professionals need to be informed of medications being used by individuals with DM. The action of the medication, typical dosage, side effects, and particularly peak activity of insulin, are important considerations when planning dental and dental hygiene treatment. To assist with this understanding, the NDEP offers a "Diabetes Medications Supplement"54 as a companion to "Working Together to Manage Diabetes."
Implications for Dental Hygiene Practice
Given the connections between diabetes, oral health and systemic health, dentists and dental hygienists have an opportunity to reframe their practices to provide comprehensive care utilizing principles of oral medicine. Based on a recent forum concerning oral health and systemic health, a consensus statement was developed that defines opportunities for knowledge transfer from research to practice, collaborations among health care providers, and treatment considerations.55 In addition to this international panel of experts that promoted collaboration among health care providers, a group of medical and dental experts convened in April 2007, to review evidence related to the association between diabetes, periodontal disease, and cardiovascular disease. Known as "The Scottsdale Project," the group's report detailed the importance of medical-dental collaboration in the co-management of persons at risk for or already diagnosed with diabetes who may have periodontal disease. The report provides recommendations for providing comprehensive oral health care while collaborating with medical health care providers.56 Likewise, the PPOD work group of the NDEP promotes the concepts of collaboration to increase awareness of diabetes, primary prevention strategies, and effective treatment approaches.16 These documents provide the basis of promoting oral health care that is based on current and relevant scientific evidence, and on a process of care that is focused on collaborative patient centered care.
Individuals who present with diabetes or prediabetes require particular attention during oral health care appointments that challenge the traditional paradigm of the 45 minute prophylaxis appointment and dental examination. Guidelines for providing care for persons with DM appear in Table 4. As can be seen from this table, comprehensive oral health care includes collaboration and consultations with other health care providers, preventive protocols to avoid emergency situations in the office, and treatment considerations.
Implementing an oral medicine approach to care for patients with DM requires a change in practice philosophy and procedures. Consideration needs to be given to modifying appointment time frames for these individuals. A longer initial appointment to allow for comprehensive assessment and treatment plan development is needed. A re-evaluation appointment needs to be scheduled to assess improvement in oral health and to determine whether or not further treatment is indicated. Further, a continuing care schedule needs to be individualized based on the patient's oral health and medical health. The traditional six month "recall" appointment will likely not be appropriate for many patients with diabetes and significant periodontal problems. The guidelines that appear in Table 4 address more frequent appointment scheduling until periodontal health has been achieved.
In addition, oral health providers must be prepared to promote health practices beyond traditional brushing and flossing reminders. Key preventive messages to promote a healthy lifestyle and better manage diabetes related conditions should be offered. Sample key preventive messages for patients with DM appear in Table 5. As can be seen from this table, the key concepts support regular evaluations with health care specialists, promoting medical-dental collaboration.
When oral health care providers give preventive and control messages to patients with DM, it is important to consider that not all messages can be provided at one appointment. Messages should be prioritized and customized according to individual needs. Key messages can be provided in the form of computer generated reminder notes or prescriptives that are handwritten. Further, the clinician should document which messages were provided and the patient's response.
To establish a broader base for relaying health prevention and control messages about diabetes, the dentist and dental hygienist can offer this information through office newsletters or provide health awareness screening and education programs for patients with diabetes. In addition, the oral health providers can establish a broad referral base that includes other health care professionals such as optometrists, podiatrists, pharmacist, diabetes educators, nurse practitioners, endocrinologists, family practitioners, and cardiologists. These individuals may not be aware of oral considerations and connections with DM. They may welcome the opportunity to collaborate and participate in continuing education programs, study clubs, and health awareness programs. Likewise, persons with diabetes may not know which health care provider to contact when experiencing a diabetes-related symptom or complication. Having a strong referral base will provide them an opportunity to seek care with informed specialists.
Further, oral health providers must develop a presence within the community to create greater awareness of the relationship between oral health and systemic health. Offering health education programs to the community, sponsoring wellness fairs, and conducting screening programs may help them view dentists and dental hygienists as partners in promoting improved total health.
Conclusion
Diabetes mellitus is a chronic disease that can be managed through medication and lifestyle changes. Serious systemic and oral complications can occur as a result of this disease. Because the disease has reached epidemic proportions in the U.S., it is essential that all health care providers, including oral health professionals, screen for those who are at risk for the disease, identify the disease in undiagnosed individuals, and assist those with diabetes in achieving optimum oral and total health.
Glossary of Terms
Diabetes mellitus – chronic, metabolic disease associated with abnormal, high levels of blood glucose
Prediabetes – a condition in which blood glucose levels are higher than normal, but not in the diabetes range
Ketosis – accumulation in the blood and tissues of large quantities of ketone bodies such as beta-hydroxybutyric acid, acetoacetic acid and acetone; may result in a sweet or "fruity" odor to the breath.
Ketoacidosis – accumulation of ketone bodies causing acidosis; usually present in uncontrolled diabetes mellitus in which there is a substantial increase in fatty acid metabolism and impaired or absent carbohydrate metabolism resulting in the increased production of ketone bodies
Polyuria – excessive excretion of urine
Polydipsia – excessive thirst
Nocturia – excessive urination at night
Diabetic retinopathy – noninflammatory disease of the retina; manifestations in diabetes mellitus include microaneurysms and punctate exudate
Neuropathy – functional disturbances and pathologic changes in the peripheral nervous system; in diabetes, neuropathy may cause pain, weakness and wasting of proximal and distal muscles, peripheral sensory impairment, and loss of tendon reflexes
Peripheral vascular disease – any disorder affecting blood flow through the veins and arteries distal to the heart, which can eventually lead to ischemic necrosis and gangrene, varicose veins and thrombophlebitis
Angiography – radiography of vessels of the body
Blood glucose meter – a device used to either visually or digitally read the glucose concentration in a drop of blood; used to help adjust medication, particularly insulin use, during treatment of diabetes mellitus.
References
1. Centers for Disease Control and Prevention. National diabetes fact sheet: general information and national estimates on diabetes in the United States, 2007. Atlanta, GA: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, 2008.
2. National Institute of Diabetes and Digestive and Kidney Diseases. National Diabetes Statistics fact sheet: general information and national estimates on diabetes in the United States, 2005.Bethesda, MD: U.S. Department of Health and Human Services, National Institutes of Health, 2005.
3. Little JW, Falace DA, Miller CS, Rhodus NL. Dental management of the medically compromised patient, 7th ed. 2008. St.Louis: Mosby Elsevier, 212-235.
4. Nathan DM, Cleary PA, Backlund JY, et al. Intensive diabetes treatment and cardiovascular disease in patients with type 1 diabetes. N Engl J Med. 2005;353:2643-2653.
5. Mensinger C. Diagnosis and classification of diabetes mellitus. Diabetes Care. 2006;29(Suppl 1):S43-S48.
6. Kumar V, Abbas AK, Fausto N. Robbins and Cotran pathologic basis of disease, 7th ed. 2005. Philadelphia: Elsevier Saunders, 1189-1207.
7. Mensing C. Standards of medical care in diabetes -- 2006. Diabetes Care. 2006;29(suppl 1):S4-S42.
8. Knowler WC, Barrett-Connor E, Fowler SE, Hamman RF, et al. Reduction in the incidence of type 2 diabetes with lifestyle intervention or metformin. N Engl J Med. 2002;346:393-403.
9. The effect of intensive treatment of diabetes on the development and progression of long-term complications in insulin-dependent diabetes mellitus. The Diabetes Control and Complications Trial Research Group. N Eng J Med. 1993;329:977-86.
10. Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes. (UKPDS) Group. Lancet. 998;352:837-53.
11. Tight blood pressure control and risk of macrovascular and microvascular complications in type 2 diabetes. IKPDS 38. UK Prospective Diabetes Study Group. BMJ. 1998;317:703-13.
12. Goldberg RB, Mleeies MJ, Sacks FM, Moyé LA, et al. Cardiovascular events and their reduction with pravastatin and diabetic and glucose-intolerant myocardial infarction survivors with average cholesterol levels; Subgroup analyses in the cholesterol and recurrent events (CARE) trial. The Care Investigators. Circulation. 1998;98:2513-9.
13. Effects of ramipril on cardiovascular and microvascular outcomes in people with diabetes mellitus. Results of the HOPE study and MICRO-HOPE substudy. Heart Outcomes Prevention Evaluation Study Investigators. Lancet. 2000;355:253-9.
14. Schwartz JS, Boccuzzi SJ, Glick H, Cook JR, et al. Cost-effectiveness of LDL-C reduction in diabetic CHD patients: Implications from the Scandinavian Simvastatin Survival Study (4S). Circulation. 1997;96(Suppl 1):1504-5 [Abstract].
15. Sack K: Doctors miss cultural needs, study says. The New York Times. June 10, 2008. Available at http://www.nytimes.com/2008/06/10/health/10study.html. Accessed June 10, 2008.
16. Centers for Disease Control and Prevention. Working Together to Manage Diabetes: A Guide for Pharmacists, Podiatrists, Optometrists, and Dental Professionals. Atlanta, GA: U.S. Department of Health and Human Services, Public Health Service, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, 2007.
17. The Diabetes Control and Complications Trial/Epidemiology of Diabetes Interventions and Complications Research Group. "Retinopathy and Nephropathy in Patients with Type 1 Diabetes Four Years After a Trial of Intensive Therapy." N Engl J Med. 2000;342: 381-89.
18. Kempen, J.H. et al. "The Prevalence of Diabetic Retinopathy Among Adults in the United States." Archives of Ophthalmology 2004;122.4: 552-63.
19. Ashton N: Studies of the retinal capillaries in relation to diabetic and other retinopathies. Br J Ophthalmology. 1963;47:521-538.
20. Fong, D.S., et al. "American Diabetes Association. Retinopathy in Diabetes." Diabetes Care. 2004; 27 (suppl. 1): S4-87.
21. Moss, S.E., R. Klein, and B.E. Klein. "The 14-year Incidence of Visual Loss in a Diabetic Population." Ophthalmology. 1998;105.6:998-1003.
22. The Diabetic Retinopathy Study Research Group. Photocoagulation treatment of proliferative diabetic retinopathy: clinical applications of Diabetic Retinopathy Study (DRS) findings: DRS Report Number 8. Ophthalmology. 1981;88:583-600.
23. The Diabetic Retinopathy Vitrectomy Study Research Group. Early vitrectomy for severe vitreous hemorrhage in diabetic retinopathy: DRVS Report Number 5. Arch Ophthalmol.1990;108:958-964.
24. Early Treatment Diabetic Retinopathy Study Research Group. Early photocoagulation for diabetic retinopathy: ETDRS Report Number 9. Ophthalmology. 1991;98(suppl):767-785.
25. ETDRS Research Group. Photocoagulation for diabetic macular edema. ETDRS Report Number 1. Arch Ophthalmol. 1985;103:1796-1806.
26. Ramsey SD, Newton K, Blough D, et al. Incidence, outcomes, and cost of foot ulcers in patients with diabetes. Diabetes Care. 1999;22:382-387.
27. Currie CJ, Morgan CL, Peters JR: The epidemiology and cost of inpatient care for peripheral vascular disease infection, neuropathy and ulceration in diabetes. Diabetes Care. 1998;21:42-48.
28. King H, Aubert RD, Herman WH. Global burden of diabetes, 1995-2025: prevalence, numerical estimates and projections. Diabetes Care. 1998; 21:1414-31.
29. Laing P. The development and complications of diabetic foot ulcers. American Journal of Surgery. 1998;76:5S-10S.
30. Jeffcoate WJ, Harding KG. Diabetic Foot Ulcers. Lancet. 2003;361-1545-1551.
31. Armstrong DJ, Lavery LA, Harkless LB: Treatment-based classification system for assessment and care of diabetic feet. JAPMA. 1996;86:311-316.
32. Kannel WB, McGee DL: Diabetes and cardiovascular disease: the Framingham Study. J Am Med Assoc. 1979;241:2035-2038.
33. Akbari CM, Pomposelli FB, Gibbons GW, Campbell DR, Pulling MC, Mydlarz D, LoGerfo FW: Lower extremity revascularization in diabetes. Arch Surg. 2000; 135:452-456.
34. Armstrong DG, Nguyen HC, Lavery LA, VanSchie CHM, Boulton AJM, Harkless LB, Off-Loading the Diabetic Foot Wound: A randomized clinical trial: Diabetes Care. 2001;24(6):1019-1022.
35. Armstrong DG, Lavery LA, Sariaya M, Ashry H. Leukocytosis is a poor indicator of acute osteomyelitis of the foot in diabetes mellitus. JFAS. 1996; 35:281.
36. Lipsky BA, Berendt AR, Deery HG, et al. Diagnosis and treatment of diabetic foot infections. Clin Infect Dis. 2004;39(7):885-910.
37. Vernillo AT: Diabetes mellitus: relevance to dental treatment. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2001;91(3):263-270.
38. Southerland JH, Taylor GW, Offenbacher S. Diabetes and periodontal infection: making the connection. Clinical Diabetes. 2005:23(4):171-178.
39. Löe H. Periodontal disease: the sixth complication of diabetes mellitus. Diabetes Care. 1993;16(1):329-34.
40. Mealey BL, Oates TW. Diabetes mellitus and periodontal diseases. J Periodontol. 2006;77:1289-1303.
41. U.S. Department of Health and Human Services. Oral Health in America: A Report of the Surgeon General. Rockville, MD: U.S. Department of Health and Human Services, National Institutes of Health, National Institute of Dental and Craniofacial Research, 2000.
42. Taylor GW. Bidirectional interrelationships between diabetes and periodontal diseases: An epidemiologic perspective. Ann Periodontol. 2001;6(1):99-112.
43. Grossi SG, Genco RJ. Periodontal disease and diabetes mellitus: Two-way relationship. Ann Periodontol. 1998;3(1):51-61.
44. Grossi SG, Skrepcinski FB, DeCaro T, Robertson DC, et al. Treatment of periodontal disease in diabetics reduces glycated hemoglobin. J Periodontol. 1997;68(8):713-9.
45. Taylor GW, Burt BA, Becker MP, Genco RJ, et al. Severe periodontitis and risk for poor glycemic control in patients with non-insulin-dependent diabetes mellitus. J Periodontol. 1996;67(10 Suppl):108S-93.
46. Donahue RP, Wu T. Insulin resistance and periodontal disease: An epidemiologic overview of research needs and future directions. Ann Periodontol. 2001;6(1):119-24.
47. Ryan ME, Carnu O, Kamer A. The influence of diabetes on the periodontal tissues. JADA. 2003;134:34S-40S.
48. Graves DA, Al-Mashat H, Liu R. Evidence that diabetes mellitus aggravates periodontal diseases and modified the response to an oral pathogen in animal models. Compend Contin Ed Dent. 2004; 25(7) (Suppl 1):38-46.
49. Saydah SH, Fradkin J, Cowie CC. Poor control of risk factors for vascular disease among adults with previously diagnosed diabetes. JAMA. 2004;291(3):335-342.
50. Galt KA. Cost avoidance, acceptance, and outcomes associated with a pharmacotherapy consult clinic in a Veterans Affairs Medical Center. Pharmacotherapy. 1998;8(5):1103-11.
51. Bluml BM, McKenney JM, Cziraky MJ. Pharmaceutical care services and results in project ImPACT: Hyperlipidemia. J Am Pharm Assoc. 2000;40(2):157-65.
52. Tsuyuki RT, Johnson JA, Teo KK, Simpson SH, et al. A randomized trial of the effect of community pharmacist intervention on cholesterol risk management: The Study of Cardiovascular Risk Intervention by Pharmacists (SCRIP). Arch Intern Med. 2002;162(10):1149-55.
53. Yeh G, Eisenberg D, Davis R, Phillips R. Use of complimentary and alternative medicine among persons with diabetes mellitus: Results of a national survey. Am J Pub Health. 2002;92:1648-52.
54. Centers for Disease Control and Prevention. Diabetes Medication Supplment: Working Together to Manage Diabetes. Atlanta, GA: U.S. Department of Health and Human Services, Public Health Service, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, 2007.
55. Oral and systemic health: consensus statement from an international panel. Inside Dentistry. 2006;2(Special Issue 1):1-9.
56. Hein C, Cobb C, Iacopino A. Report of the independent panel of experts of 'The Scottsdale Project'. Published as a special supplement to Grand Rounds in Oral-Sys Med. 2007;3.
About the Authors
JoAnn R. Gurenlian, RDH, PhD, is the owner of Gurenlian & Associates, offering consulting and continuing education programs for health care providers. She has experience in general, periodontic, pediatric, and orthodontic practices, and works part-time in a medical practice. She is an internationally recognized speaker on the topics of oral pathology, oral medicine, diabetes, and women's health. She currently serves as the Vice President of the International Federation of Dental Hygienists, and Chair of the Pharmacy, Podiatry, Optometry, and Dental Professionals (PPOD) Work Group of the National Diabetes Education Program (NDEP).
W. Lee Ball, OD, FAAO, is an optometrist in Boston, Massachusetts. He is an adjunct professor of optometry at Beth Israel Deaconess Medical Center and Joslin Diabetes Center. Dr. Ball serves as the Vice Chair of the PPOD Work Group of the NDEP.
Javier La Fontaine, DPM, MS, is the chief of the podiatry section of the Central Texas Veterans health Care System and associate professor, Department of surgery, of Texas A&M University, College of Medicine in Temple, Texas. Dr. Fontaine is a member of the PPOD Work Group of the NDEP.