You must be signed in to read the rest of this article.
Registration on CDEWorld is free. Sign up today!
Forgot your password? Click Here!
Working as an oral health provider offers many rewards and challenges. With one exception, oral diseases are not fatal. Most oral health conditions can be prevented or treated successfully with education and regular dental and dental hygiene care. Unfortunately, the one oral disease that can be life-threatening is the disease that is often overlooked with respect to emphasis on prevention and early detection in clinical practice settings.
According to the National Cancer Institute, it is estimated that 36,540 Americans will be diagnosed with oral and pharyngeal cancer and 7880 deaths will occur.1 Sadly, of those newly diagnosed, only about 60 percent of those diagnosed with this disease will be alive in 2016.2 Oral cancer is the 6th most common malignancy in the world.3 It is estimated that over 640,000 new cases will be identified worldwide on a yearly basis.4
Placing perspective on the magnitude of oral cancer, this disease kills approximately one person per hour, every day. It is more common than Hodgkin's disease, and cancers of the brain, liver and bone. Approximately $3.2 billion is spent annually in the United States on treatment of this disease.4
The prognosis for oral and pharyngeal cancer varies depending upon when it is identified. Approximately 83 percent of patients with localized lesions survive beyond five years.2 Prognosis is significantly worse when oral cancer has metastasized resulting in a 28 percent survival rate.5 Oral cancer has a high risk of producing second primary tumors. If a patient survives the initial diagnosis and treatment, they still have up to a 20 time higher risk of developing a second cancer.4
These statistics can be improved with emphasis on prevention and early detection. Unfortunately, oral and pharyngeal cancer is routinely discovered at a later stage in development when the cancer has already metastasized. Part of the problem is that early cancer is painless and not easily recognized by the patient. The other contributing element is that dental practitioners are not placing the same level of importance on early detection of oral cancer as they place on the prevention and treatment of caries and periodontal disease.6 Therefore, this paper will highlight key elements of oral cancer as well as current approaches used for early detection.
Oral Cancer Considerations
Over 90 percent of oral cancers are squamous cell carcinoma (SCC). These lesions present as leukoplakia, erythroplakia, or erythroleukoplakia. There are multiple risk factors for and causes of oral cancer as noted in Table 1. Tobacco use and alcohol consumption are the most common risk factors and etiologies of oral cancer. Other cofactors include periodontal disease, poor oral hygiene, ill-fitting dentures, sharp teeth and edentulism.7 It is important to note, however that approximately 25 percent of patients with oral cancer do not fit the traditional profile and have no risk factors.8-12
More recent attention to risk factors for oral cancer have focused on exposure to the human papillomavirus (HPV), which has led to annual increases in the incidence of tonsillar and base-of-tongue cancers.13 Multiple sex partners and unprotected sex increases the risk of exposure to HPV. Although there are over 130 subtypes of HPV, subtype HPV-16 accounts for more than 90 percent of cases of HPV-SCC.13 Other types less frequently detected in oropharyngeal cancers include HPV6, 18, 31, 33, 35, 45, 52 and 58.14,15 As the evidence for an association between HPV and oropharyngeal cancer mounts,16-18 further research into HPV vaccination has been suggested as a means to demonstrate causality.13
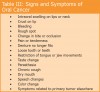
As noted previously, oral cancer tends to be painless initially. In the absence of pain there are a variety of warning signs and symptoms that are associated with oral cancer. These warning signs of oral cancer are summarized in Table II. Signs and symptoms of oral cancer appear in Table III. These tables provide information that can be addressed with patients during prevention procedures that are part of oral health care assessment.
Screening Options for Early Detection
Those who have reviewed the evidence associated with adjunctive screening devices for oral cancer advocate the comprehensive oral examination (COE) as the "gold standard" for early detection.19 All dental and dental hygiene students are taught how to perform a COE; however, this procedure is not performed routinely on all patients once students transfer to licensed clinicians.6,20 Studies have demonstrated that not all dentists feel knowledgeable about the etiology of oral cancer or how to perform a COE.21-24 Further, it has been noted in the report, Healthy People 2010 and Healthy People 2010 Midcourse Review, that only 13 percent of Americans recall having an oral examination performed in the past year.25,26Healthy People 2020 targets the goal of increasing this statistic to 20 percent so that more individuals receive an annual COE.27 To assist dental professionals with reviewing the procedure for performing an oral examination, the National Institute of Dental & Craniofacial Research of the National Institutes of Health has published a document entitled "Detecting Oral Cancer: A Guide for HealthCare Professionals." This guide can be downloaded for free at www.nidcr.nih.gov.28
Although the eye is a valuable tool in the performance of an oral examination, it is not the sole tool available for identifying early SCC. Other adjunctive devices that may be used in clinical practice include the OralCDx® Brush Test®, ViziLite®, VELScope®, and Identafi®. These devices are not meant to take the place of the COE; rather they are available to supplement and support oral cancer examinations and screenings.
In his editorial concerning oral cancer screening aids, Dr. Lingen discussed the need for adherence to suggested guidelines for research related to adjunctive screening devices. He noted that studies should clearly address sensitivity, specificity, or positive predictive value (PPV) of these devices. Further, these studies should provide these data in relation to the COE. Dr. Lingen advocated that research about these devices should be placed in the context in which they could demonstrate that there is improvement beyond.29 This perspective provides the basis for discussing adjunctive screening devices. Definitions for these key terms are provided in Box 1.
Brush biopsy is biopsy in which cells or tissues are obtained by manipulating tiny brushes against the tissue or lesion in question. This device has been used successfully for biopsies of bronchial, renal, ureter, bile, pancreatic, gastric and nasopharynx tissues. Applications of the brush biopsy system to the oral cavity have been developed through OralCDx®, which is part of CDx Diagnostics™. This system is based on the microscopic study of cell samples from the oral cavity. A specialized brush is used to collect transepithelial cells onto a glass slide for surface oral and oropharyngeal mucosal abnormalities, which may include leukoplakia; erythroplakia; erythroleukoplakia and speckled leukoplakia. These samples are sent to a laboratory for staining and analysis. Computer-based imaging ranks the cells on the basis of abnormal morphology. A cytopathologist then interprets the results and findings are faxed to the dental office. Results are reported as "negative," "positive," or "atypical." Abnormal results require follow-up with scalpel biopsy.
A landmark study published in 1999 described the results of a multicenter study involving 35 academic institutions and 945 patients evaluating the detection of precancerous and cancerous oral lesions using the brush biopsy. Sensitivity was reported as 96 percent, specificity of "positive" lesions at 97 percent and "atypical" lesions at 90 percent.30 A study comparing the brush biopsy results with follow-up scalpel biopsy was reported in 2002. Findings of this study of 243 patients with abnormal brush biopsies revealed a positive predictive value of "atypical" lesions as 38 percent and only 1 false negative case reported.31 In a study of 103 cases comparing the brush biopsy with scalpel biopsy on the same lesion, sensitivity was reported at 92.3 percent and specificity at 94.3 percent.32 A study conducted in Sweden provided a positive predictive value for "atypical" lesions as 42.9 percent and for "positive" lesions at 100 percent,33 while Poate and colleagues reported PPV value of 44. 1 percent and a negative predictive value of 60 percent (n=112).34 In contrast, Bhoopathi and colleagues performed a cross-sectional study of the brush biopsy in detecting dysplastic lesions by evaluating 152 pathology reports from scalpel biopsies of those who tested either "positive" or "atypical." They found that the PPV was only 7.9 percent for "positive" lesions and 7.4 percent for "atypical" lesions. The proportion of false-positive was 92.1 percent. These authors noted that OralCDx® overestimated dysplastic lesions and produced a high number of false-positive results.35
In their report of a systematic review of the literature on adjunctive techniques for oral cancer examination and diagnosis, Patton, Epstein and Kerr36 evaluated studies performed related to the brush biopsy. They found inconsistencies in the specificities and PPVs across studies of the OralCDx® brush biopsy and noted weaknesses including lack of information about original clinical lesion diagnosis and failure to conduct histopathological examination on all suspicious lesions perhaps biasing the results related to sensitivity, specificity and PPV. These authors recommended that future studies could be improved by sampling lesions that have been present for a period of time (10–14 days) after the removal of the suspected etiology.36
In their review of scientific evidence about Oral CDx®, Rethman, et al.19 concluded that there was not enough evidence to support a recommendation for or against the use of this device in innocuous mucosal lesions. They indicated the belief that clinically suspicious lesions should be biopsied immediately; however, OralCDx® had relevance to be used for those patients with multiple lesions throughout the oral cavity, nonadherent patients, those individuals with disabilities who may not be able to safely tolerate a scalpel biopsy procedure, and those with a history of previous upper airway and digestive tract cancer.19
Chemiluminescent light offers another way to enhance visualization techniques for oral cancer screening. ViziLite® Plus with TBlue® (from Zila Pharmaceuticals) combines a blue-white light energy source with toluidine blue staining. Patients pre-rinse with a 1 percent acetic acid solution, which is followed by examination of the oral cavity with a blue-white light source. Lesions that appear white are followed by TBlue® metachromatic dye so further evaluation and monitoring of changes can be made.
Kerr and colleagues reported on the effectiveness of ViziLite® to enhance visualization of mucosal lesions in 501 subjects. The findings demonstrated that this type of visualization can provide additional information, in particular with leukoplakias.37 A study of ViziLite® with TBlue® was performed comparing this technique with conventional visual examination. Ninety-seven clinically suspicious lesions in 84 patients were evaluated. Results demonstrated that the brightness and sharpness of margins were improved in 61.8 percent of lesions using ViziLite®. The authors reported that biopsied lesions stained with toluidine blue reduced the false positive rate by 55.26 percent and the negative predictive value was 100 percent.38 Ram and Siar conducted a study comparing ViziLite® with a 1 percent tolonium chloride mouth rinse. Forty-six lesions and 5 cases of normal oral mucosa from 40 subjects were examined with these technologies. Sensitivity reported for ViziLite® and tolonium chloride was 100 percent and 70.3 percent respectively, while specificity was noted to be 14.2 percent for ViziLite® and 25 percent for tolonium chloride.39
Further analysis of studies related to chemiluminescence found concerns about the quality of the Ram and Siar study, and inconsistent accuracy values with specificity ranging from zero to 14 percent, PPVs of 18 to 80 percent, and negative predictive values (NPVs) of zero to 100 percent. Another limitation noted was that the studies involved only those patients who had been previously identified with visualized mucosal lesions.36
Autofluorescence imaging provides another means of assessing potentially malignant oral pathoses. The VELscope® system (LED Dental Inc.) uses narrow emission fluorescence exposing oral mucosa to a blue light spectra. Tissue that is undergoing dysplastic or neoplastic changes will demonstrate a loss of fluorescence. Abnormal tissue appears as an irregular, dark area against normal, green fluorescence patterns found in surrounding healthy tissue. The device has been commercially available since 2006.
Most of the literature reported on the use of VELscope® has reflected case reports and observational studies.40-42 In a pilot study of 44 patients, Lane et al examined the effectiveness of autofluorescence direct visualization with histology. Results in terms of sensitivity and specificity were 98 percent and 100 percent respectively.43 Scheer, et al reported on a recent study of 64 patients considered at risk for SCC. These individuals had biopsies performed following examination with the Velscope® device. Results revealed sensitivity of 100 percent, specificity of 80.8 percent, PPV 54.5 percent and NPV was 100 percent. The authors noted that the group studied was high-risk and that additional histology controlled prospective studies in a general population were needed to determine the role of this imaging device as an adjunctive screening aid.44
In contrast to the above studies, Mehrota, et al evaluated the ViziLite® and Velscope® in the detection of clinically innocuous precancerous and cancerous oral lesions. This cross sectional study involved 258 patients who were found to have clinically innocuous lesions. Of these individuals, 102 were in the Vizilite® group and underwent biopsy, while there were 156 subjects in the Velscope® group who were biopsied. Results of the Vizilite® group revealed that three had dysplasia and one had cancer. The sensitivity rate was 0 percent, specificity was 75.5 percent, PPV was 0 percent and NPV was 94.8 percent. Results of the VELscope® group revealed that 11 had dysplasia, one had cancer, and six of these were detected with this device. The sensitivity rate was 50 percent, specificity was 38.9 percent, PPV was 6.4 percent and NPV was 90.3 percent. The authors concluded that use of these devices with a COE was not beneficial in identifying dysplasia or cancer, and that further studies were indicated prior to recommending these devices.45
One criticism of the VELscope® system is that there have been no published studies assessing its effectiveness as a diagnostic adjunct in lower-risk populations.36 Huff et al reported on an investigation of a low-risk population in a general dental practice setting. During the period of the study, 959 patients ages 12 and older received a standard COE. One year later, 905 patients received a conventional oral examination and VELscope® examination. Results of this study revealed that the visual examination showed a prevalence of mucosal abnormalities of 0.83 percent, none of which were premalignant. Screening with the VELscope® device yielded a 1.3 percent prevalence of mucosal abnormality, of which 83 percent were potentially premalignant.46
Another device using autofluorescence technology is Identafi® (Dental EZ Group). This device utilizes three distinct wavelengths, white light, violet light, and green-amber light, to screen for oral cancer and premalignant dysplasia. This technology is based on multispectral optical imaging. The technology was developed and tested by observing changes in fluorescence between normal tissues and those patients who present with precancerous and cancerous lesions. Roblyer and colleagues47 reported their imaging pilot study that demonstrated that patients with histologically confirmed neoplasia demonstrated decreased bluegreen autofluorescence and increased red autofluorescence. Further, they could detect increased visibility of vasculature using narrow-band reflectance and orthogonal polarized reflectance. The authors concluded that multispectral imaging may provide information not available through fluorescence mode alone, and may be useful in "discriminating precancerous and cancerous tissue from normal and benign or inflammatory regions."47
Additional studies of this autofluorescence technology have focused on identifying optical devices that distinguish epithelial fluorescence from stromal fluorescence, using excitation wavelengths in the UV range to improve diagnostic accuracy,48 and creating a computational model to study how tissue characteristics affect clinically measured spectra.49 Another report presented an algorithm to objectively delineate neoplastic oral mucosa from autofluorescence imaging. In this study, an algorithm was applied to patient images and histologic sections of resected tissues were used as a validation measure. Results indicated 95.9 percent sensitivity and 96.2 percent specificity in a training set discriminating normal tissue from dysplasia and invasive carcinoma. The validation set revealed a sensitivity of 100 percent and specificity of 91.4 percent.50
Clinical studies related to the use of Identafi® are limited. One paper provided an overview of a case report using this autofluorescence imaging to detect a metastatic palatal tumor that appeared clinically innocuous, but was confirmed as a metastatic SCC.51 Further research is needed to determine the efficacy of this device among patients in oral health practices.
It is important to note that all these devices are considered safe and cost-effective for use in dental practice settings. More studies are needed to determine the efficacy of these devices in community settings and with low-risk populations. Although reviewers have discussed the lack of adjunctive devices to distinguish between benign, premalignant, and malignant lesions as a major limitation of these tools,19,36 they fail to mention the obvious. The COE does not distinguish between these types of lesions as well. The fact is that all lesions considered suspect need to be biopsied to determine the definitive diagnosis. Eyes are only trained to see abnormal, not see into the cells of the tissue clinically. Some screening tools are used to identify more details of a lesion once detected by a COE (i.e., OralCDx® Brush test®). Other screening tools (i.e., VELScope®, Identafi®) are used to identify lesions that may not be detected during a visual COE. Therein lies the value of these adjunctive screening devices. While they may not provide a histologic analysis, these devices do provide additional information that may translate to early detection of premalignant and malignant lesions. The future relevance of these adjunctive devices for oral cancer screening and detection remains to be determined.
First Line of Defense
As a prevention specialist, dental hygienists are the first line of defense for assessing patients for risks and identifying signs of oral cancer. Teaching patients about oral cancer examinations and screenings, and performing regular oral cancer examinations at every appointment is part of the dental hygiene process of care and policy of the American Dental Hygienists' Association.52,53
Some patients are not aware that any dental professional has ever performed a COE. Educating patients about this important component of dental hygiene assessment helps them appreciate the scope of responsibilities of their care provider. As well, it offers the patient an opportunity to ask questions about their oral health. Patients may not know that technological advances in screening for oral cancer exist and the benefits of using these devices. Teaching patients about these additional screening approaches will help them gain acceptance of their use in practice. Technological advances are fluid and dynamic. As advances in adjunctive screening devices occur, dental hygienists can update their patients accordingly.
Engaging patients as active participants in the process of oral cancer awareness, examination, and screening is another important consideration. Patients can be asked to identify their risks for oral cancer. Table I in this paper can be modified and used as a tool that patients complete prior to their dental hygiene appointment. Reviewing perceptions of risk factors with the patient opens the door to discussing signs and symptoms or oral cancer and prevention strategies. For example, if a patient identifies that he smokes cigarettes daily and has a family history of cancer, an opportunity has presented itself for discussing the COE, adjunctive screening, and smoking cessation. If another patient identifies a risky sexual history, the hygienist can use that information to discuss the need for oral cancer evaluation and prevention strategies that may include HPV vaccination or DNA testing if deemed appropriate.
Another avenue of engaging active involvement of patients is to teach them how to perform an oral cancer self-examination. The concept of performing a self-examination is not new to patients. They may already be performing self-exams for other types of cancer early detection. Adding this examination process to their standard home care regimen helps the patient recognize their own responsibility in early recognition of oral health concerns. The sidebar accompanying this paper presents a review of the oral cancer examination procedure that both patients and clinicians can use to assist in the recognition and diagnosis of oral cancer.54
Finally, and equally important for the benefit of the patient, is to teach them to advocate for and request a regular COE and subsequent adjunctive screening, as deemed appropriate, as part of every dental and dental hygiene appointment. There is no substitute for awareness.
References
1. Oral Cavity and Pharynx Cancer Stat Fact Sheet. Surveillance, Epidemiology, and End Results (SEER) Program, National Cancer Institute. Bethesda, MD, Available at: http://www.seer.cancer.gov/statfacts/html/oralcav.html. Accessed July 2, 2011.
2. American Cancer Society. Oral Cancer. Available at: http://www.cancer.org/acs/groups/content/@nho/documents/document/oral-cancerpdf.pdf. Accessed July 2, 2011.
3. Lingen MW, Kalmar JR, Karrison T, Speight PM. Critical evaluation of diagnostic aids for the detection of oral cancer. Oral Oncol 2008;44(1):10-22.
4. The Oral Cancer Foundation web site. Oral Cancer Facts. Available at: http://oralcancerfoundation.org/facts/index/htm. Accessed June 28, 2011.
5. Oral Cancer Statistics. Oral Cancer in the United States. Available at: http://www.nidcr.nih.gov/FactSheet2.pdf. Accessed July 2, 2011.
6. Kammer C. Shine a light on oral cancer. Dental Products Report. October, 2009. Available at: http://www.dentalprodcutsreport.com/ articles/show/dpr1009. Accessed May 3, 2011.
7. Bsoul SA, Huber MA, Terezhalmy GT. Squamous cell carcinoma of the oral tissues: A comprehensive review for oral healthcare providers. J Contemp Dent Pract. 2005;6(4):1-16.
8. Schantz SP, Yu GP. Head and neck cancer incidence trends in young Americans, 1973-1997, with a special analysis for tongue cancer. Arch Otolaryngol Head Neck Surg. Mar 2002;128(3):268-274.
9. Lingen M, Sturgis EM, Kies MS. Squamous cell carcinoma of the head and neck in nonsmokers: clinical and biologic characteristics and implications for management. Curr Opin Oncol. May 2001;13(3):176-182.
10. Shiboski CH, Shiboski SC, Silverman S, Jr. Trends in oral cancer rates in the United States, 1973-1996. Community Dent Oral Epidemiol. Aug 2000;28(4):249-25.
11. Llewellyn CD, Johnson NW, Warnakulasuriya KA. Risk factors for squamous cell carcinoma of the oral cavity in young people–a com prehensive literature review. Oral Oncol. Jul 2001;37(5):401-418.
12. Corcoran TP, Whiston DA. Oral cancer in young adults. J Am Dent Assoc. Jun 2000;131(6):726.
13. D'Souza G, Freimer AR, Viscidi R, Pawlita M, et al. Case-control study of human papillomavirus and oropharyngeal cancer. N Engl J Med 2007;356:1944-1956.
14. Machado J, Reis PP, Zhang T, Simpson C, et al. Low prevalence of human papillomavirus in oral cavity carcinomas. Head &Neck Oncology 2010. 2:6.
15. Gillison ML, Shah KV. Role of mucosal human papillomavirus in nongenital cancers. J Natl Cancer Inst Monograph Chapter 9. 2003;(31): 57-65.
16. Schwartz, SM, Daling JR, Doody DR, Wipf GC. Oral cancer risk in relation to sexual history and evidence of human papillomavirus infection. J Natl Cancer Inst 1998;90(21):1626-1636.
17. Herrero R, Castellsagué X, Pawlita M, Lissowska J, et al. Human papillomavirus and oral cancer: the international agency for research on cancer multicenter study. J Natl Cancer Inst 2003;95(23):1772-1783.
18. The HPV Connectionthe human papillomavirus related to oral cancer. Oral Cancer Foundation. Available at http://oralcancerfoundation.org. Accessed 4/12/11.
19. Rethman MP, Carpenter W, Cohen EEW, Epstein J, et al. Evidence based clinical recommendations regarding screening for oral squamous cell carcinomas. J Am Dent Assoc 2010;141(5):509-520.
20. Hein, C, Kunselman B, & Frese, P: Preliminary findings of consumer-patient's perceptions of dental hygienists' scope of practice/qualifications and the level of care being rendered. American Dental Hygienists' Association Annual Session, June, 2006.
21. Horowitz AM, Nourjah PA. Factors associated with having oral cancer examinations among US adults 40 years of age or older. J Public Health Dent 1996;56:331–5.
22. Horowitz AM, Drury TF, Goodman HS, Yellowitz JA. Oral pharyngeal cancer prevention and early detection: dentists' opinions and practices. JADA 2000;131:453–62.
23. Yellowitz JA, Horowitz AM, Drury TF, Goodman HS. Survey of U.S. dentists' knowledge and opinions about oral pharyngeal cancer. JADA 2000;131:653–61.
24. Horowitz AM, Siriphant P, Sheikh A, Child WL. Perspectives of Maryland dentists on oral cancer. JADA 2001;132:65–72.[Abstract/Free Full Text]
25. U.S. Department of Health and Human Services, Office of Disease Prevention and Health Promotion. Healthy People 2010: objective 21—oral health. Available at: "www.health.gov/healthypeople/Document/HTML/Volume2/21Oral.htm" (scroll down to Objective 21-7). Accessed Sept. 23, 2001.
26. U.S. Department of Health and Human Services. Healthy People 2010 Midcourse Review. Washington, D.C.: U.S. Government Printing Office, December 2006.
27. Healthy People 2020 Topics & Objectives. Available at http://www.healthypeople.gov/2020/topicsobjectives2020/default.aspx. Accessed July 2, 2011.
28. National Institute of Dental & Craniofacial Research, National Institutes of Health. Detecting Oral Cancer: A Guide for Health Care Professionals. National Institutes of Health. Bethesda, MD. May 12, 2011.
29. Lingen MW. Oral cancer screening aids: where is the science? Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2007;103(2):153-154.
30. Sciubba JJ and the U.S. Collaborative OralCDx Study Group. Improving detection of precancerous and cancerous oral lesions: Computer-assisted analysis of the oral brush biopsy. U.S Collaborative OralCDx Group. J Am Dent Assoc 1999;130:1445-1457.
31. Svirsky JA, Burns JC, Carpenter WM, et al. Comparison of computer-assisted brush biopsy results with follow up scalpel biopsy and histology. Gen Dent 2002;50:500.
32. Scheifele C, Schmidt-Westhausen AM, Dietrich T, Reichart PA. The sensitivity and specificity of the OralCDx technique: evaluation of 103 cases. Oral Oncol. Sep 2004;40(8):824-828.
33. Kosicki DM, Riva C, Pajarola GF, et al. OralCDx brush biopsy. A tool for early diagnosis of oral squamous cell carcinoma. Schweiz Monatsschr Zahnmed 2007;117:222-2
34. Poate TW, Buchanan JA, Hodgson TA, et al. An audit of the efficacy of the oral brush biopsy technique in a specialist Oral Medicine unit. Oral Oncol. Sep 2004;40(8):829-34.
35. Bhoopathi V, Kabani S, Mascarenhas AK. Low positive predictive value of the oral brush biopsy in detecting dysplastic oral lesions. Cancer 2009;115(5):1036-1040.
36. Patton, LL, Epstein JB, Kerr R. Adjunctive techniques for oral cancer examination and lesion diagnosis: a systematic review of the literature. J Am Dent Assoc 2008;139(7):896-905.
37. Kerr AR, Sirois DA, Epstein JB. Clinical examination of chemiluminescent lighting: an adjunct for oral mucosal examinations. J Clin Dent 2006;17(3):59-63.
38. Epstein JB, Silverman S Jr, Epstein JD, et al. Analysis of oral lesion biopsies identified and evaluated by visual examination, chemiluminescence and toluidine blue. Oral Oncol 2008 June;44(6):538-544.
39. Ram S, Siar CH. Chemiluminescence as a diagnostic aid in the detection of oral cancer and potentially malignant epithelial lesions. Int J Oral Maxillofac Surg 2005;Jul;34(5):521-527.
40. Kois J, Truelove E. Detecting oral cancer: a new technique and case reports. Dent Today 2006;25:96-97.
41. Poh CF, Zhabg L, Anderson DW, et al. Fluorescence visualization detection of field alterations in tumor margins of oral cancer patients. Clin Cancer Res 2006;12:6716-6722.
42. Poh CF, Ng SP, Williams PM, et al. Direct fluorescence visualization of clinically occult high-risk oral premalignant disease using a simple hand-held device. Head Neck 2007;29:71-76.
43. Lane PM, Gilhuly T, Whitehead P, et al. Simple device for the direct visualization of oral-cavity tissue fluorescence. J Biomed Opt. 2006;11(2):024006.
44. Scheer M, Neugebauer J, Derman A, et al. Autofluorescence imaging of potentially malignant mucosa lesions. Oral Sur Oral Med Oral Pathol Oral Radiol Endod 2011;111:568-577.
45. Mehrotra R, Singh M, Thomas S, et al. A cross-sectional study evaluating chemiluminescence and autofluorescence in the detection of clinically innocuous precancerous and cancerous oral lesions. J Am Dent Assoc 2010;141(2):151-156.
46. Huff KD, Stark PC, Solomon LW. Sensitivity of direct tissue fluorescence visualization in screening for oral premalignant lesions in general practice. Gen Dent 2009 Jan-Feb;57(1):34-38.
47. Roblyer D, Richards-Kortum R, Sokolov K, et al. Multispectral optical imaging device for in vivo detection of oral neoplasia. J Biomed Opt 2008 March/April 13(2),024019.
48. Pavlova I, Williams M, El-Naggar A, et al. Understanding the biological basis of autofluorescence imaging for oral cancer detection: high-resolution fluorescence microscopy in viable tissue. Clin Cancer Res 2008;14(8):2396-2404.
49. Pavlova I, Weber CR, Schwarz RA, et al. Fluorescence spectroscopy of oral tissue; Monte Carlo modeling with site-specific tissue properties.
50. Roblyer D, Kurachi C, Stepanek V, et al. Objective detection and delineation of oral neoplasia using autofluorescence imaging. Cancer Prev Res 2009;2(5):423-431.
51. Vigneswara N, Koh S, Gillenwater A. Incidental detection of an occult oral malignancy with autofluorescence imaging: a case report. Head & Neck Oncology 2009,1:37. Available at http://www.headandneckoncology.org/content/1/1/37. Accessed July 13, 2011.
52. American Dental Hygienists' Association. Standards for clinical dental hygiene practice. Chicago: American Dental Hygienists Association. March 10, 2008. Available at www.adha.org. Accessed July 14, 2011.
53. American Dental Hygienists' Association. Policy manual. Chicago: American Dental Hygienists' Association. January 24, 2011. Available at www.adha.org. Accessed July 14, 2011.
54. National Institute of Dental & Craniofacial Research, National Institutes of Health. Detecting Oral Cancer: A Guide for Health Care Professionals. National Institutes of Health. Bethesda, MD. May 12, 2011.
Support Organizations
Government
The National Cancer Institute
www.cancer.gov
1800-4-CANCER
National Health Information Center
www.health.gov/nhic
1-800-336-4797
National Institutes of Health
www.nlm.nih.gov
National Institute of Dental & Craniofacial Research
www.nidcr.nih.gov
1-301-496-4261
SEER Program
seer.cancer.gov
Cancer Organizations
American Cancer Society
www.cancer.org
Association of Cancer Online Resources
www.acor.org
1-212-226-5525
Cancer Care Inc.
www.cancercare.org
1-800-813-HOP
The Oral Cancer Foundation
www.oralcancerfoundation.org
Head and Neck Cancer Alliance
www.headandneck.org
Professional Societies
American Association for Cancer Research
www.aacr.org
1-215-440-9300
American Head and Neck Society
www.headandneckcancer.org
1-310-437-0059
American Dental Association
www.ada.org
1-312-440-2500
American Dental Hygienists' Association
www.adha.org
1-312-440-8900
American Association of Oral and Maxillofacial Surgeons
www.aaoms.org
1-847-678-6200
About the Author
JoAnn R. Gurenlian, RDH, PhD, is president of Gurenlian & Associates, and provides consulting services and continuing education programs to health care providers. She is a visiting scholar at Capella University, Department of Dental Hygiene, adjunct faculty at Burlington County College and graduate faculty at Idaho State University. The author is not affiliated with the sponsor of this supplement or any manufacturer of products mentioned. The supplement was developed in collaboration between the sponsor and the American Dental Hygienists' Association.