You must be signed in to read the rest of this article.
Registration on CDEWorld is free. Sign up today!
Forgot your password? Click Here!
Medical computed tomography (CT) and cone beam scanners (CBCT) allow for the 3-dimensional (3-D) visualization of a patient’s anatomy. It is now possible to determine the height and width of available bone for implants; soft-tissue thicknesses; proximity and root anatomy of adjacent teeth; and the location of the maxillary sinuses, mental foramena, mandibular and incisive canals, and other vital structures in 3-D.1-3
After importing images into proprietary software programs (eg, SimPlant®, Materialise Dental, www.materialisedental.com; NobelClinician, Nobel Biocare, www.nobelbiocare.com, and others), implant placement can be “virtually” planned for a patient’s anatomy and treatment plan. Prior to performing surgery, the type and size of the planned implant, its bony position, its relationship to the planned restoration and adjacent teeth and/or implants, and its proximity to vital structures can be determined.1-5 Computer-aided manufactured (CAM) drilling guides can then be fabricated from the “virtual” treatment plan. These surgical guides are used to place the planned implants in the same positions as the “virtual” plan. This allows for more accurate and predictable implant placement 6-10 as well as reduced patient morbidity.11-14
All current CT/CBCT systems have similar workflows. Essentially, maxillary and mandibular arch impressions are made and a bite registration is obtained. Diagnostic casts are poured and mounted on an articulator. Guided surgery requires reverse planning. First, a restorative plan is made by creating a diagnostic tooth arrangement that indicates the dental anatomy and positions of the teeth to be replaced. An acrylic resin prosthesis, which reproduces the planned restorations in the appliance, is then fabricated. Depending on the system used, this “scan prosthesis” can be a removable partial or complete denture. To allow for radiopacity in the CT/CBCT images, most systems—other than NobelGuide (Nobel Biocare)—require that the planned restorations contain a 20% to 30% barium sulphate mixture in the resin. NobelGuide uses a double-scan technique with a hard-resin scan prosthesis and gutta percha fiducial marker reference points, but no barium sulphate. The CT/CBCT scan is then taken with the patient wearing the scan prosthesis. Some software programs allow for the creation and placement of “virtual teeth” in a computer environment. These features are limited to partially edentulous cases in which teeth are in the area to be used as references. The CT scan DICOM (digital imaging and communication in medicine) images are then imported into proprietary software programs (eg, SimPlant; NobelGuide; coDiagnostiX™, Straumann, www.straumann.com, etc.). The programs are used to “virtually” place implants into their ideal positions related to the planned restoration and underlying bony anatomy. The digital plan is then uploaded via the Internet for the CAM fabrication of a surgical guide. The surgical guide is used, along with implant-specific drilling instrumentation, to place the implants in the same positions, depths, and angulations as planned “virtually.”
Many guided implant technologies require radiopaque fiducial markers to be placed in the scan prosthesis worn during the CT/CBCT scan. The software uses these reference markers to position the scan prosthesis, and with it, the parameters of the planned restoration(s) related to the patient’s jaw. For some CBCT scanners it is difficult to accurately assess these geometric markers, adding potential error to a precise planning system. This can lead to inaccurately fitting surgical guides and implant placement errors. It is advisable to determine and use CBCT scanners with high levels of accuracy or medical CT scanners.15
Indications for Use
An argument could be made for the use of guided implant surgery in most implant patients because of its precision and accuracy. However, a cost/time/benefit determination must be made based on individual circumstances. Increased patient and treatment planning time, extra expense in laboratory and radiology fees, and added patient radiation exposure may outweigh the benefits. These technologies are most beneficial when the following clinical situations are applicable:
- planning for three or more implants in a row
- proximity to vital anatomy
- problems with the proximity of adjacent teeth
- questionable bone volume (deficient width or height, or unusual bony contours)
- implant position that is critical to the restoration
- flapless implant placement
- multiple-unit or complete-arch immediate restorations, with or without extractions and immediate placement
- significant alteration of soft tissue or bony anatomy by prior surgery or trauma
- patients with other physical, medical, or psychiatric comorbidities
Discussion
Commonly used surgical guides can be simple (vacuform shells with buccal or palatal/lingual facings of the planned restorations) or more complex (2-mm holes or metal tubes). When using these conventional appliances, there is no correlation between the planned restoration and the underlying bony anatomy. When using computer-guided surgical guides, this anatomic relationship can be predictably established and considered prior to surgery.
The patient’s anatomy and local references—such as the numbers and locations of teeth in the arch to be treated or in the opposing arch—determines surgical guide fabrication. As the edentulous area lengthens, fewer anatomic references are present for the predictable, accurate placement of implants. In a completely edentulous arch—other than the ridge, vestibules, and palate—all local references are lost. Bone and soft-tissue loss from periodontal disease and atrophy, long-term denture wear, and sinus pneumatization can make it difficult to predictably use a traditional surgical guide.
Three types of computer-generated surgical guides are available: tooth-supported, mucosa-supported, and bone-supported. Tooth-supported guides are used in partially edentulous patients; the guide rests on teeth in the arch for accurate fit. Mucosa-supported guides rest on mucosa and are primarily used in completely edentulous patients. Accurate inter-arch bite registrations are important when using these guides to assure precise guide positioning and placement of securing screws or pins prior to implant placement (Figure 1). Bone-supported guides can be used in partially or completely edentulous patients, with their primary use being in completely edentulous applications when ridge atrophy is present and good seating of a mucosa-supported guide is questionable. An extensive full-thickness flap is necessary when using bone-supported guides to expose the bone in the implant sites and adjacent areas for an intimate fit of the guide over the bony ridge.
Compared to the “freehand” technique, implant placement using guided surgery with drill guides enhances safety16,17 and is compatible with either flap-elevation surgery or flapless procedures.18 Absolute precision is not found with any CT-guided drilling technology. Errors can be made in all dimensions in stereolithographic (SLA) and CAM guides when comparing virtual planning and actual implant positions.19 Implants placed by mucosa-supported guides have low mean deviations; implants placed by bone-supported guides have higher deviations.20 Because teeth are present as accurate “stops,” tooth-supported guides have the lowest measured deviations.21 Errors are minimized by using a single guide with metal guide sleeves and rigid screw or pin fixation, as well as implant-specific drilling instrumentation. Most systems use these fixation modalities to stabilize mucosa-supported guides; some use them to stabilize all guides.
The two primary systems in use are SimPlant and NobelGuide/NobelClinician. NobelGuide has full instrumentation sets for fully guided placement of most all Nobel Biocare implants, with the components to immediately load implants. NobelGuide and BIOMET 3i Tapered Navigator® System (BIOMET 3i, www.biomet3i.com) have instrumentation for tapered implant placement. SimPlant is an open system for all implant systems. While this increases its functionality, it can also be a limitation because it is not perfectly adapted to one implant system comprehensively. Using the SimPlant platform, several manufacturers have developed and marketed instrumentation for placing their straight-walled implants flaplessly and fully guided (Facilitate™, DENTSPLY Implants, www.dentsplyimplants.us; ExpertEase™, DENTSPLY Implants; BIOMET 3i Straight Navigator). Other manufacturers have developed non-CAM technologies for surgical guide fabrication (coDiagnostiX; iGuide™, iDent Imaging, www.ident-surgical.com; EasyGuide®, Keystone Dental, www.keystonedental.com; and others). With these technologies, a CT/CBCT scan is obtained while the patient wears a barium radiographic appliance. The implant placement is then planned “virtually.” The surgical guide is fabricated by milling the radiographic appliance according to the digital treatment plan.
Limitations and questions associated with CT-based technologies merit further investigation. They include questions regarding the resolution and accuracy of specific CBCT machines compared to the “gold standard” of medical-grade CT scanners.22 Nobel Biocare markets a “calibration object,” which calibrates an individual CT/CBCT machine to an acrylic resin object of known contour and density specifically for the NobelGuide protocol. This object has been shown to add to the precision of the SLA fabrication of the NobelGuide.23
The manufacture of a SLA guide or model involves reproducing the object’s digitally planned dimensions by using a laser beam to selectively solidify an ultraviolet-sensitive liquid resin. Inherent potential problems can lead to light sensitivity and expansion and/or contraction of SLA materials, which distort when exposed to light for extended periods of time and when sterilized in high-temperature autoclaves. Regardless of the irrigation system used, implant site preparation using surgical drill guides generates more heat than conventional implant site preparation.24
Indications for CT-Guided Implant Surgery
Planning for Three or More Implants in a Row
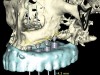
When three or more implants in a row are planned, concepts of spacing and angulations, parallelism in all dimensions, proximity to anatomic structures, and relationships between implant positions and planned restorations are all significant considerations. CT/CBCT-guided surgery allows for the ideal placement of multiple dental implants according to the planned restoration while taking these issues into consideration (Figure 2 and Figure 3). Implants can be placed flaplessly and immediately loaded.6-8,11-14,25-29
Proximity to Important Anatomic Structures
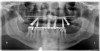
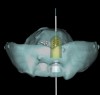
Panoramic and periapical radiographs are 2-dimensional (2-D) representations of a patient’s 3-D anatomy. Differences in radiographic machines and techniques can lead to image distortion, such as elongation and shortening of anatomy. Accurate evaluation and measurement of the relationship between the mental nerve, inferior alveolar nerve (Figure 4), or nasopalatine/incisive nerve, and the planned implant position can best be determined and planned by a 3-D evaluation of the anatomy as related to the planned restoration.3,30 Implant placement in patients in whom there is a question of nerve or sinus proximity is most accurate using “virtual” treatment planning and placement using CT-generated guides, thus minimizing potential patient morbidity. Technologies such as “all-on-four,” which is designed to maximize the intra-arch spread of implant platforms while avoiding the mandibular nerve and maxillary sinus, are excellent indications for CT-guided implant surgery (Figure 5 and Figure 6).
Problems Related to Proximity of Adjacent Teeth
Surgical dilemmas where implant placement is required in a single location or depth are common. Difficult scenarios frequently necessitate implant placement into tight spaces with minimal bony leeway mesial-distally, buccal-lingually, or both. Adjacent roots may require “threading the needle” with implant placement; this is commonly encountered with congenitally missing teeth. Limited bone volume often leaves situations in which the anatomy dictates where the implant can be placed.30
To aid in accurate implant placement between and adjacent to roots in planned sites, all proprietary implant-planning software programs have functionality to isolate roots in edentulous areas. Some software programs use virtual dots or lines to outline the roots (Figure 4), while others can alter the software’s sensitivity to Hounsfield units or isovalues to virtually remove bone around roots (“segmentation”) (Figure 7). These features are beneficial when roots are divergent or convergent or when implants must be placed in tight spaces due to close root proximities. Visualization of adjacent roots allows precise implant positioning in limited mesial-distal spaces. The ideal implant for the specific clinical application can then be selected. Some software programs allow the selection and placement of “virtual” stock and custom abutments.
Questionable Bone Volume
In cases involving limited bone volume, including deficient width or height, or unusual bony contours, the anatomy often dictates where an implant can be placed—usually in one location only. A CT/CBCT evaluation of the site can lead to decisions to perform preparatory grafting procedures. Three-dimensional evaluation of a grafted site provides valuable information as to the amount and location of the grafted bone volume, allowing for accurate implant placement.30 If guided implant placement is planned, occasionally a second CT/CBCT may be indicated after grafting.
In extraction/immediate implant placement patients, concavities can be found in the bone apical to the tooth to be extracted. Fenestrations and perforations can occur if this is not recognized preoperatively. In the anterior maxilla, the thickness of the palatal bone can be instrumental in determining whether an extraction with immediate implant placement can be accomplished with good primary stability.
Implant Position Critical to the Restoration
Some of the most complex restorative and surgical patients treated in implant dentistry involve single and multiple implants in the esthetic zone. Thicknesses of crestal and buccal soft tissues and buccal and palatal cortical plates, buccal-lingual ridge dimensions, proximity to adjacent teeth, implant-to-root relationships, gingival and papilla support and contours, gingival exposure, smile lines, and implant angulations and emergence are a few of the many complex considerations.
An important prosthetic consideration is knowledge of the appropriate implant position based on the type of restoration planned (cement- or screw-retained). Small variations in implant positions can lead to difficult restorative dilemmas. Accurate and predictable implant positioning using guided implant planning and placement can be critical to the esthetic and functional success of the restoration30 (Figure 8 through Figure 11).
Flapless Surgery and Multiple-Unit Immediate Placement/Immediate Load
Newer implant designs and surface characteristics have shortened the time required between implant placement and loading. Immediate placement and immediate loading of implants with provisional restorations are now common. Treatment planning has changed with concepts of cross-arch stabilization of implants and loading of multiple implants. These technologies are available to place single, multiple, or a complete arch of implants flaplessly. Patients experience less pain and swelling with less surgical trauma. Recovery time is reduced, and patients’ ability to return to their normal lives is expedited.6-8,11-14,25-30
Guided implant surgery involves reverse treatment planning. The ideal contour and arch position of the restoration is planned first, followed by virtual planning of the implant into that position according to the bony anatomy and clinical scenario. SLA surgical guides are then fabricated from the treatment plan. A dental laboratory next uses the SLA guide, with mounted casts, to fabricate provisional restorations prior to implant placement. At the time of surgery, the surgical guide is used to place the implants flaplessly, removing only a tissue core in the implant site(s). Abutments are immediately placed, and provisional restorations can be inserted.15-20 (Figure 12 through Figure 17).
Although technologies are available to place immediate definitive restorations, most clinicians are placing provisional restorations, for many reasons. Whether performed flaplessly or not, after surgery the final gingival contours and anatomy cannot be predicted. The clinician and dental technician can gain invaluable information as to the gingival contours and esthetics by observing tissue responses from the provisional restoration. Whether implant placement is guided or nonguided, a small number of implant failures occur. Most surgery-related failures take place within the first 3 to 4 months after implant placement. Surgical and restorative implant failure management is best accomplished prior to insertion of the definitive restoration. According to Abrahamsson et al, changing from a healing abutment to a permanent abutment did not result in a change in the dimension and quality of the transmucosal attachment that developed. It did not differ from the mucosal barrier that formed on a permanent abutment placed after surgery.31 An acrylic resin occlusal surface or a composite restoration reduces the forces of impact and has a better shock-absorbing behaviour compared to ceramic materials32; this is an additional reason for placing immediate acrylic resin provisional restorations, rather than immediate definitive porcelain restorations.
Minimally invasive procedures maximize patient comfort by minimizing tissue injury. Flapless insertion of implants has success rates comparable to conventional placement, while minimizing complications from soft-tissue elevation such as infection, dehiscence, and soft- and hard-tissue necrosis.13,33,34 Since fully guided instrumentation for implant insertion is not available in many SimPlant cases, fully flapless surgery is not advised. Depth and angulation guidance of all osteotomies is possible, but accurate implant platform placement requires an incision and flap elevation for direct visualization of the platform position in bone. Fully guided and flapless placement of implants using SimPlant is possible if using Navigator-, ExpertEase-, Facilitate-, or SimPlant-fabricated NobelGuide-compatible surgical guides, because fully guided instrumentation is available. Straumann coDiagnostiX has proprietary software and instrumentation for full-guided placement of Straumann implants.
Complex Problems with Significant Alteration of Bony Anatomy
The concept of “placing the implants where the bone is” is becoming a thing of the past in dentistry. Various soft-tissue and bone-alteration procedures are now commonly done for implant site preparation. Block bone grafts, ridge splitting, sinus lifts, and alveolar distraction procedures, as well as large and small soft-tissue and connective-tissue grafts, are a few of the procedures routinely performed. Previous surgical procedures, including the placement of different types of implants (blade and subperiosteal implants) can leave patients with challenging reconstructive defects (Figure 18). Traumatic injuries can result in loss of bone, teeth, and soft tissue. Treatment of benign and malignant pathology can result in defects of varying sizes, creating surgical dilemmas in the reconstruction of areas of abnormal bony anatomy and scarred soft tissue (Figure 19 and Figure 20).
After healing, graft maturation, and settling of graft materials, resultant bone and soft-tissue volumes can be unpredictable. Before implant placement, lateral block-onlay grafts can resorb a portion of their bone volume.35-37 CT technology allows for the prediction of the volume of sinus lift graft material necessary to augment the desired bone height of an area.38 Variability occurs in the shape and width of alveolar distracted bone. Three-dimensional analysis allows better assessment of these areas compared to 2-D radiographs.
Computer-guided surgery allows for the evaluation and visualization of distorted anatomy. Implants can be planned predictably and placed without making an incision or disrupting the periosteal vascularization of grafted or affected areas.39
Patients with Physical, Medical, or Psychiatric Comorbidities
Head and neck cancer patients are often treated with pre- and/or postoperative radiation therapy, which may potentially alter tissue and bone vascularity and healing capacity. Research and treatment protocols in place since the early 1980s discuss the use of pre- and postoperative hyperbaric oxygen (HBO) therapy to increase the vascularity of the tissue and bone prior to dental surgical procedures.40-42 Placing implants with minimal flap elevation and soft- and hard-tissue trauma is indicated to limit the likelihood that these patients will develop osteoradionecrosis of the jaws.43,44 Bleeding, swelling, and alteration of bone and soft-tissue vascularization are minimized by using these technologies.45
Patients with bleeding dyscrasias, anticoagulation issues, or significant cardiovascular disease may require specific medication protocols that cannot be altered prior to surgery. Minimizing bleeding by minimizing surgical trauma is indicated in these patients. Three-dimensional evaluation and planning with CT-guided implant placement enables the placement of implants flaplessly with accuracy and precision. These technologies are ideally indicated for use in patients with these challenging medical management problems.17,45
Dental patients present with various historical experiences, some of which can be problematic. Patient stress, anxiety, and phobias, as well as orthopedic and spinal problems can prevent them from undergoing procedures requiring long periods in a dental chair. Wheelchair-bound patients pose another set of logistical problems. These patients often require extensive planning and preparation prior to treatment, which must be performed quickly and efficiently without compromising quality. By using 3-D guided technologies, most planning and anatomic issues encountered during surgery are visualized before the patient is seated in the dental chair. Implants can be placed quickly and predictably, minimizing the patient’s stress, pain, and time in the chair, with surgical time reduced to a minimum.
Keys to Optimal Outcomes
CT-guided surgery does not excuse the surgical and restorative team from diligent adherence to the principles of oral and implant surgery and prosthetic implant dentistry. Adhering to and maintaining established concepts of implant depth and angulation, spacing, osseointegration times, ideal occlusion, planning and engineering, minimally traumatic manipulation of soft and hard tissues, bone and soft-tissue grafting and healing, heat generation, dental materials, and many others are of utmost importance to successful outcomes. The requirements of the patient and the comfort level of the surgical and restorative team will dictate the treatment plans generated with these technologies. Cases can be treated with implants buried and staged, with healing abutments, or immediately loaded with provisional restorations. Critical factors for success are proper case selection and patient awareness, education, and compliance. The advantages of using these technologies were reiterated in the Academy of Osseointegration’s 2009 consensus statements and recommended clinical procedures regarding computer-assisted implant dentistry.30
A steep learning curve is necessary for the successful integration of CT technology and CT-guided surgery into implant practice. Clinicians interested in these technologies are encouraged to pursue continuing education prior to their clinical use. Successful outcomes require knowledge of CT scans, proprietary computer planning software, complete treatment workflows, and guided-surgery instrumentation and techniques. Clinicians should consider the inherent additional costs involved in using these proprietary software and CAD/CAM-processing technologies. Good patient selection and diagnosis, pretreatment planning, knowledge of the technology, and adherence to surgical and prosthetic principles will strongly affect outcomes.
Conclusion
3-D implant patient evaluation and planning with guided surgery has opened new avenues in a multidisciplinary restoratively driven treatment approach for accurate and predictable implant treatment. A key component to improved results is good clinician communication and understanding of these technologies. Analyzing, understanding, and adopting future technologies will not only change the way patients are treatment-planned, but will offer patients the benefits of improved predictable outcomes.
References
1. Ludlow JB, Laster WS, See M, et al. Accuracy of measurements of mandibular anatomy in cone beam computed tomography images. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2007;103(4):534-542.
2. Pattijn V, Van Cleynenbreugel T, Vander Sloten, et al. Structural and radiological parameters for the nondestructive characterization of trabecular bone. Ann Biomed Eng. 2001;29(12):1064-1073.
3. Sonick M, Abrahams J, Faiella RA. A comparison of the accuracy of periapical, panoramic, and computerized tomographic radiographs in locating the mandibular canal. Int J Oral Maxillofacial Impl. 1994;9(4);455-460.
4. Todd AD, Gher ME, Quintero G, Richardson AC. Interpretation of linear and computed tomograms in the assessment of implant recipient sites. J Periodontol. 1993;64(12):1243-1249.
5. Gehr ME, Richardson AC. The accuracy of dental radiographic techniques used for evaluation of implant fixture placement. Int J Periodontics Restorative Dent. 1995;15(3):268-283.
6. van Steenberghe D, Glauser R, Blombäck U, et al. A computed tomographic scan derived customized surgical template and fixed prosthesis for flapless surgery and immediate loading of implants in fully edentulous maxillae. A prospective multicenter study. Clin Implant Dent Relat Res. 2005;7 Suppl 1:S111-S120.
7. Tardieu P, Vrielinck L. Implantologie assistèe par ordinateur: le propramme SimPlant/SurgiCase™ et le SAFE System™ mis en charge immediate d’unbridge mandibulaire avec des impalt transmuqueux. Implant. 2003;9:15-28.
8. Rosenfeld AL, Mandelaris GA, Tardieu PB. Prosthetically directed implant placement using computer software to ensure precise placement and predictable prosthetic outcomes. Part 3: stereolithographic drilling guides that do not require bone exposure and the immediate delivery of teeth. Int J Periodontics Restorative Dent. 2006;26(5):493-499.
9. Vrielinck L, Politis C, Schepers S, et al. Image-based planning and clinical validation of zygoma and pterygoid implant placement in patients with severe bone atrophy using customized drill guides. Preliminary results from a prospective clinical follow-up study. Int J Oral Maxillofac Surg. 2003;32(1):7-14.
10. Sarment DP, Sukovic P, Clinthorne N. Accuracy of implant placement with a stereolithiographic surgical guide. Int J Oral Maxillofac Implants. 2003;18(4):571-577.
11. Hahn, J. Single stage, immediate loading, and flapless surgery. J Oral Implantol. 2000;26(3):193-198.
12. Campelo LD, Dominguez Camara JR. Flapless implant surgery: a 10-year clinical retrospective analysis. J Oral Maxillofac Implants. 2002;17(2):271-276.
13. Becker W, Goldstein M, Becker BE, Sennerby L. Minimally invasive flapless implant surgery: a prospective multicenter study. Clin Implant Dent Relat Res. 2005;7 Suppl 1:S21-S27.
14. Becker W, Wikesjö UM, Sennerby L, et al. Histologic evaluation of implants following flapless and flapped surgery: a study in canines. J Periodontol. 2006;77(10):1717-1722.
15. Nickenig HJ, Eitner S. Reliability of implant placement after virtual planning of implant positions using cone bean CT data and surgical (guide) templates. J Craniomaxillofac Surg. 2007;35(4-5):207-211.
16. Komiyama A, Pettersson A, Hultin M, et al. Virtually planned and template-guided implant surgery: an experimental model matching approach. Clin Oral Implants Res. 2010;22(3):308-313.
17. Wagner A, Wanschitz F, Birkfellner W, et al. Computer-aided placement of endosseous oral implants in patients after ablative tumour surgery: assessment of accuracy. Clin Oral Implants Res. 2003;14(3):340-348.
18. Casap N, Tarazi E, Wexler A, et al. Intraoperative computerized navigation for flapless implant surgery and immediate loading in the edentulous mandible. Int J Oral Maxillofac Implants. 2005;20(1):92-98.
19. D’Haese J, Van De Velde T, Komiyama A, et al. Accuracy and complications using computer-designed stereolithographic surgical guides for oral rehabilitation by means of dental implants: a review of the literature. Clin Implant Dent Relat Res. 2012;14(3):321-335.
20. Arisan V, Karabuda ZC, Ozdemir T. Accuracy of two stereolithographic guide systems for computer-aided implant placement: a computed tomography-based clinical comparative study. J Periodontol. 2010;81(1):43-51.
21. Ozan O, Turkyilmaz I, Ersoy AE, et al. Clinical accuracy of 3 different types of computed tomography-derived stereolithographic surgical guides in implant placement. J Oral Maxillofac Surg. 2009;67(2):394-401.
22. Van Assche N, van Steenberghe D, Guerrero ME, et al. Accuracy of implant placement based on pre-surgical planning of three-dimensional cone-beam images: a pilot study. J Clin Periodontol. 2007;34(9):816-821.
23. Wouters V, Mollemans W, Schutyser F. Calibrated segmentation of CBCT for digitization of dental prostheses. Int J Comp Assist Radiol Surg. 2011;6(5):609-616.
24. Misir AF, Sumer M, Yenisey M, Ergioglu E. Effect of surgical drill guide on heat generated from implant drilling. J Oral Maxillofac Surg. 2009;67(12):2663-2668.
25. Tardieu PB, Vrielinck L, Escolano E. Computer-assisted implant placement. A case report: Treatment of the mandible. Int J Oral Maxillofac Implants. 2003;18(4):599-604.
26. van Steenberghe D, Naert I, Andersson M, et al. A custom template and definite prosthesis allowing immediate implant loading in the maxilla: a clinical report. Int J Oral Maxillofac Implants. 2002;17(5):663-670.
27. van Steenberghe D, Ericsson I, Van Cleynenbreugel J, et al. High precision planning for oral implants based on 3D CT scanning. A new surgical technique for immediate and delayed loading. Appl Osseoint Res. 2004;4:27-30.
28. Katsoulis J, Pazera P, Mericske-Stern R. Prosthetically driven, computer-guided implant planning for the edentulous maxilla: a model study. Clin Implant Dent Relat Res. 2009;11(3);238-245.
29. Sanna AM, Molly L, van Steenberghe D. Immediately loaded CAD-CAM manufactured fixed complete dentures using flapless implant placement procedures: a cohort study of consecutive patients. J Prosthet Dent. 2007;97(6):331-339.
30. Hämmerle CH, Stone P, Jung RE, et al. Consensus statements and recommended clinical procedures regarding computer-assisted implant dentistry. Int J Oral Maxillofac Implants. 2009;24 Suppl:126-131.
31. Abrahamsson I, Berglundh T, Sekino S, Lindhe J. Tissue reactions to abutment shift: an experimental study in dogs. Clin Implant Dent Relat Res. 2003;5(2):82-88.
32. Gracis SE, Nicholls JI, Chalupnik JD, Yuodelis RA. Shock-absorbing behavior of five restorative materials used on implants. Int J Prosthodont. 1991;4(3):282-291.
33. Arisan V, Karabuda CZ, Ozdemir T. Implant surgery using bone- and mucosa-supported stereolithographic guides in totally edentulous jaws: surgical and post-operative outcomes of computer-aided vs. standard techniques. Clin Oral Implants Res. 2010;21:980-988.
34. Cannizzaro G, Torchio C, Leone M, Esposito M. Immediate versus early loading of flapless-placed implants supporting maxillary full-arch prostheses: a randomised controlled clinical trial. Eur J Oral Implantol. 2008;1(2):127-139.
35. Johansson B, Grepe A, Wannfors K, Hirsch JM. A clinical study of changes in the volume of bone grafts in the atrophic maxilla. Dentomaxillofac Radiol. 2001;30(3):157-161.
36. Verhoeven JW, Ruijter J, Cune MS, et al. Onlay grafts in combination with endosseous implants in severe mandibular atrophy; one year results of a prospective, quantitative radiological study. Clin Oral Implants Res. 2000;11(6):583-594.
37. Smolka W, Eggensperger N, Carollo V, et al. Changes in the volume and density of calvarial split bone grafts after alveolar ridge augmentation. Clin Oral Implants Res. 2006;17(2):149-155.
38. Krennmair G, Krainhofner M, Maier H, et al. Computerized tomography-assisted calculation of sinus augmentation volume. Int J Oral Maxillofac Implants. 2006;21(6):907-913.
39. Orentlicher GP, Goldsmith DH, Horowitz AD. Applications of 3-dimensional virtual computerized tomography technology in oral and maxillofacial surgery: current therapy. J Oral Maxillofac Surg. 2010;68(8):1933-1959.
40. Marx RE. Osteoradionecrosis. A new concept of its pathophysiology. J Oral Maxillofac Surg. 1983;41(5):283-288.
41. Marx RE, Ames JR. The use of hyperbaric oxygen therapy in bony reconstruction of the irradiated and tissue-deficient patient. J Oral Maxillofac Surg. 1982;40(7):412-420.
42. Granström G. Placement of dental implants in irradiated bone: The case for using hyperbaric oxygen. J Oral Maxillofac Surg. 2006;64(5):812-818.
43. Granström G. Radiotherapy, osseointegration, and hyperbaric oxygen therapy. Periodontol 2000. 2003;33:145-162.
44. Koga DH, Salvajoli JV, Alves FA. Dental extractions and radiotherapy in head and neck oncology: review of the literature. Oral Dis. 2008;14(1):40-44.
45. Horowitz A, Orentlicher G, Goldsmith D. Computerized implantology for the irradiated patient. J Oral Maxillofac Surg. 2009;67(3):619-623.
Related content:
Learn more about Cone Beam products at dentalaegis.com/go/cced260
About the Authors
Gary Orentlicher, DMD
Private Practice
New York Oral
Maxillofacial, and Implant Surgery
Scarsdale, New York
Andrew Horowitz, DMD, MD
Private Practice
New York Oral, Maxillofacial, and Implant Surgery
Scarsdale, New York
Marcus Abboud, DMD
Chairman
Department of Prosthodontics and Digital Technologies
School of Dental Medicine
Stony Brook University
Stony Brook, New York