You must be signed in to read the rest of this article.
Registration on CDEWorld is free. Sign up today!
Forgot your password? Click Here!
Patients have an increased awareness of their appearance and how it affects their business and personal relationships. Many often desire an esthetic enrichment of their smile. McLaren and Cao outlined the differences between cosmetic and esthetic enhancement. Cosmetic means to do “something superficial to cover a defect or deficiency,” whereas “esthetics denotes a sense of beauty that is attractive but natural.”1 Romano, in devising the title The Art of the Smile for his book, realized the “smile” incorporates three main components: the teeth, the lips and the gingiva.2
The size, shape, shade, and texture of the teeth and their interaction with the lips and gingiva involve the concept of smile design. McLaren and Fradeani1,3,4 also indicated the evaluation of the smile should be accomplished in a logical sequence:
• Facial analysis (general facial balance)
• Dento-facial analysis (maxillo-mandibular relationships to the face and the dental midline to the face)
• Dento-labial analysis (the relationships of the teeth to the lips)
• Dento-gingival analysis (the relationship of the teeth to the gingiva)
• Dental analysis (the inter-tooth and intra-tooth relationships—form, position, and color).
The constant progression of dental materials and techniques has also allowed the dentist to often restore teeth with a minimally invasive approach. Coachman and colleagues coined the term visagism5 to encourage the dentist to not only provide restorations that are not only esthetic but also restorations that incorporate the patient’s desires and personality in the final design. The purpose of this article is to provide the reader with a systematic evaluation of dento-facial esthetics and the proper selection of materials and techniques that need to be incorporated when restoring anterior teeth.
The Design Process
Previously, treatment was initiated from biology to structure, to function, and eventually to esthetics. Currently, it is recommended to progress from esthetics to function to structure and then to biology.6 Smile analysis is usually accomplished from the frontal aspect. Sarver and Ackerman increased the scope of information used in analysis by incorporating oblique, sagittal, and time-specific dimensions.7 Ackerman and Ackerman developed8 a ratio they termed the smile index. The smile index is defined as the area framed by the vermillion boundary of the lips for the duration of a social smile and is created by dividing the commissure width by the interlabial opening during a smile. Ideally the patient should display approximately 75% of the central incisor while smiling and less is considered insufficient (Figure 1). A reduced incisor presentation can be a result of vertical maxillary deficiency, an increased smile index, or short clinical crown height. The reduced clinical height may be due to deficiency of tooth eruption, gingival infringement, or tooth attrition.
Incisal Edge
The initial step in smile evaluation is the determination of the incisal edge of the central incisors relative to the upper lip (Figure 2).9 The upper lip of the patient should be at rest and a ruler is used to measure the location of the incisal edge relative to the upper lip. The amount of satisfactory incisal display at rest is age related. The resiliency of the upper lip decreases as the patient ages, with resultant diminished tooth display and increased mandibular tooth display. The sex and race of the patient also have to be considered.
Insufficient incisal edge display would necessitate restorative treatment, orthodontic extrusion, and/or orthognathic surgery.10 The selection of optimal treatment will be determined by facial proportions, amount of existing tooth structure, and the relation to the mandibular arch. Excessive tooth display requires apical movement of the maxillary incisors. Again, this may entail incisal edge reduction, restorations, orthodontics, or orthognathic surgery. The tooth size and position, lip length, and lip mobility have to be taken into consideration. Typical lip length has been determined to be 20 to 24 mm from the base of the nose to the edge of the upper lip.11 McLaren1 has found that most patients with esthetic expectations desire to display 3 to 4 mm at rest with the tips of the incisors in close proximity to the lower lip.
Maxillary Midline
After incisal edge position is determined, the maxillary midline must be ascertained. This is the least noticed by patients and dentists, but canting 2 mm to left or right is immediately discerned. Once the incisal edge and midline are determined, the labiolingual inclination has to be evaluated. The labial surface of the current maxillary incisors should ideally be perpendicular to the patient’s posterior occlusal plane. Retroclined or proclined teeth may require orthodontics or restorative treatment. The posterior edges of the maxillary teeth should be an extension of the anterior smile line. The buccal cusps of the maxillary posterior teeth are often determined by using the interpupillary line as a reference.6
Gingival Level
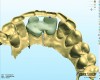
The gingival level is then considered relative to the incisal edge that has been determined. The ideal gingival level is calculated by creating an accurate width-to-length ratio of the maxillary anterior teeth, ascertaining the degree of gingival display desired and symmetry bilaterally (Figure 3). The subsequent step is the determination of the papilla levels in relation to the crown length of the central incisors. This has usually been determined to be 50% contact and 50% papilla.13,14 Once the incisal edge has been determined, an intraoral mock-up using bisacryl provisional material (eg, Luxatemp® Ultra, DMG America, www.dmg-america.com) should be inserted to verify incisal edge position and midline (Figure 4). Once the mock-up and treatment plan is accepted by the patient, the teeth can be prepared with minimal preparation needed to achieve esthetic goals. Figure 5 shows such a preparation for placement of four lithium disilicate crowns (IPS e.max®, Ivoclar Vivadent, www.ivoclarvivadent.com). For this case, the crowns and two partial veneers (Figure 6) are tried on a model (Figure 7). The final result demonstrates an esthetic result can be achieved using lithium disilicate with a combination of full and partial coverage (Figure 8 and Figure 9).
Material Selection
The selection of the most suitable restoration for anterior teeth is often a difficult decision. The anterior dentition can present with a variable amount of damage. The treatment option that best suits the patient, the restorative dentist, and sometimes the technician will determine to some extent the choice of materials. The selection of the best material to restore the dentition will depend on the esthetic requirements, the occlusion, and the shade of the underlying preparation (eg, endodontically treated teeth, posts, or implants). Cardosa and colleagues coined the “concept of restorative volume” based on structural, optical, and periodontal elements to determine how these features will impact the short-and long-term conduct of the restorations.15
Ideally, the minimally invasive approach that achieves the esthetic desires of the patient would be most appropriate. There is increasing indication that it is possible to bond decidedly esthetic restorations with minimal preparation. This allows the tooth to retain its original physical properties; however, proper preparation design is critical. Composites and ceramics are acceptable materials for anterior restorations. Each material has its indications, benefits, and limitations, and sometimes various materials can be used successfully for a similar purpose. The selection of the most appropriate material may depend on the clinician, the age of the patient, life expectancy of the material, and the esthetic requirements.
Composite Veneers
Resin composite can be placed directly or with new generation composite veneers such as Componeers® (Coltene Whaledent, www.coltene.cpom) or Edelweiss™ Composite Veneers (Ultradent, www.ultradent.com). Componeers are polymerized, prefabricated nano-hybrid composite (Synergy D6, Coltene Whaledent) enamel shells that combine the advantages of direct composite restoration with the advantages of prefabricated veneers. Componeers are thin veneer shells (0.3 mm cervically and 0.6 to 1.0 mm at the incisal edge). Componeers are placed with Synergy D6 so the pre-polymerized and unpolymerized composite are used. Each composite veneer in the Edelweiss system is laser sintered, combining a high-gloss, uniform surface with a thermally tempered base.16,17
Dietchi and Devigus provided the following indications for single direct composite veneer restorations: non-vital, discolored teeth; extensive restorations; traumatized teeth but not endodontically treated; extensive tooth fracture; and dysplasia and hypoplasia.16 Additionally, they can be used for more extensive rehabilitations in cases of tetracycline staining, fluorosis, enamel hypoplasia/dysplasia, extensive restorations, worn incisal edges, a young patient, and financial concerns. The preparations and cementation are similar to that of porcelain veneers except for modifications needed in the cervical profile and proximal and incisal edges. In appropriate cases, it serves to offer the clinician a one-visit alternative to porcelain veneers at a reasonable cost.
Direct Composites
Direct composites are excellent for conservative restorations on anterior teeth. The functional and esthetic properties of dental composite resins have greatly improved since their introduction.18 Recent improvements embrace the development of new monomers, increased filler loading, and reduced particle size. Translucency, value, and chroma are closely connected in direct composite resin restorations. The dentin and enamel layers must be placed very precisely so that the optical properties match those of the adjacent dentition. To minimize chroma mismatch, precise layering of dentin shades are critical. The enamel thickness also has to be precisely controlled so that a discrepancy in the optical properties doesn’t occur.
Direct composites can be used in the anterior to restore simple to more complex restorations such as Class IV, full veneers, and peg-shaped incisors. Since the tooth is polychromatic, however, reproduction of the inherent characteristics of natural teeth requires an artistic capacity. An understanding of color, translucency, fluorescence, and opalescence are required to derive the best results from current composites, as natural teeth demonstrate these characteristics. A failure is a result of an incorrect analysis of the natural dentition and the inability to use the capabilities of current composites.
Dietchi has described four different layering concepts.19 The classical two-layer concept requires only opaque and incisal (transparent) materials. This is a relatively monochromatic rendition of the natural tooth, however. The classical three-layer concept incorporates dentin and enamel followed by one of several incisal transparent composites. The modern two-layer concept incorporates dentin with varying chroma and enamels that may be white opalescent, neutral ivory, or gray translucent, depending on the age of the patient. The trendy three-layer concept incorporates the same concept of the modern two-layer system, but in addition uses “effect” materials that are placed between the dentin and enamel layers to mimic anatomic details (Figure 10, Figure 11, and Figure 12).
The Uveneer™ System (Dental Art Innovations Pty Ltd, www.uveneers.com) is a translucent template that is pressed over composite that has been laid on a tooth. Any composite the clinician prefers can be used. The template is removed after the material has cured. It is autoclavable and can be reused. It has a non-stick surface and is designed for all cases requiring a composite veneer application, such as one or multiple teeth to correct diastemas; fractures; abraded, discolored, or malposition teeth; caries restoration; and other esthetic corrections. It can be used for the creation of temporary veneers between appointments when porcelain veneers are manufactured in a laboratory and for direct chairside mock-up for demonstration before the application of any type of veneer.
Ceramics
Since the first feldspathic porcelain crown was introduced by Land,20 the desire for nonmetallic, biocompatible, and esthetic restorations has greatly increased. The clinical inadequacies of these materials, including brittleness, crack propagation, low tensile strength, wear resistance, and marginal accuracy, have previously limited their use. There are many products on the market today that have improved physical characteristics, making them viable options for many types of restorations.
Ceramic veneers are usually fabricated from either feldspathic ceramics (Figure 13 and Figure 14) or glass ceramics. Petridis and colleagues21 found both materials had an adequate survival rate after 5 years and minimal complications. Gurel and colleagues22 found that porcelain laminate veneers (PLVs) confined to enamel had a 99% survival compared to 94% with enamel at only the margins. PLVs bonded to dentin and margins in dentin were 10 times more likely to fail. Crown lengthening increased the risk by 2.3 times. This has to be considered when establishing the gingival margin to create the ideal length-to-width ratio.
Lithium disilicate can be used for veneers, single crowns, and anterior conventional bridges and resin-bonded fixed partial dentures (RBFPD). The longevity of two-unit cantilevered RBFPD has ranged from 95.5% to 100% over a period of 35 to 52 months. These cases were not influenced by case selection, as bruxers were included. The success has been attributed to the fact that the prosthesis will not be subject to unfavorable interabutment stresses.23 The concept of guided tooth preparations, based on natural tooth morphology (provided by a wax-up and a mock-up), creates a tailored and practical approach to indirect ceramic veneer tooth preparations.24
The concept of a laboratory-guided preparation technique for minimally invasive laminate veneers was conceived by de Anrade and colleagues.25 The tooth preparation was guided by a laboratory-made guide, termed the ultimate ceramic veneer (UCV) guide, for tooth reduction. The UCV guide was placed on each tooth for a controlled reduction. The guide has to be very stable during this procedure. Hajtó and Marinescu26 feel this method does not always work well and that it can be risky with regarding seating precision. Modern CAD/CAM technology can be used to fabricate a thin veneer (0.4 mm) made of lithium disilicate in one visit to provide the correct contour for a malformed tooth.27
Yttria tetragonal zirconia polycrystal (Y-TZP) is the sturdiest of current dental ceramics and is often used as a core material in full-coverage crowns (Figure 15 through Figure 17). Conventional Y-TZP is not esthetic and is often veneered with matching porcelain. Porcelain is brittle, however, and porcelain veneers may be disposed to chipping.28 To overcome some of porcelain’s deficiencies, several modifications have been introduced. Monolithic zirconia crowns have been introduced to avoid the necessity of a veneering porcelain and research has indicated the amount of antagonistic enamel wear after 6 months is comparable with, or even lower than, that caused by other ceramic materials.29
Monolithic zirconias have superior chipping and flexural fracture resistance in comparison with their veneered equivalents.30 Polishing decreases the lightness, however; glazing also decreases the lightness but increases the yellowness of monolithic zirconia. This may be problematic in an esthetic area.31 The introduction of translucent zirconia has increased its esthetic potential and versatility.32 The translucency of all materials increased exponentially as the thickness decreased. All of the zirconia ceramics evaluated in a study by Wang and colleagues showed some degree of translucency but were less sensitive to thickness compared to the glass ceramics.33 Different sintering conditions result in differences in grain size and translucency as well.34
Restorations can be colored individually prior to sintering, followed by characterization with staining.35 Good esthetic results in the posterior region are achieved, even in cases with substantially reduced space, but in the anterior, more traditional material may allow greater esthetic potential. Another alternative was introduced by Zhang and colleagues36 with the development of a graded ceramic. Dense zirconia was infiltrated with a matching glass to the depth of 0.1 creating a resilient veneering coat. This improved esthetics by controlling the color shading of the infiltrated glass.36
Conclusion
The rehabilitation of the anterior dentition involves several steps that must be accomplished in the appropriate sequence. The first step after a conventional examination is the recording of all pertinent data required to formulate an esthetic diagnosis. Once an esthetic diagnosis is made and the patient agrees to the treatment plan, the most appropriate material needs to be selected for the restorative phase. If the patient doesn’t have a high smile line and possibly metal abutments (implant or posts), traditional porcelain-fused-to-metal restoration can be used (Figure 18 and Figure 19). The ideal would be to accomplish the esthetic goals of the patient and clinician with minimal removal of hard and soft tissue. A well thought-out treatment plan should provide a long-lasting esthetic result.
Acknowledgements
The authors wish to thank WVneer laboratory for the e.max case photographs, Jurim Dental Studio for the feldspathic veneers and zirconia (Lava) case photographs, and New Dent Dental Lab for the implant-supported PFM bridge photographs. Finally, thanks to Dr. Newton Fahl for generously supplying the Class IV composite photographs, as well as for his friendship and the inspiration to achieve excellence.
References
1. McLaren EA, Cao PT. Smile analysis and esthetic design: “In the zone.” Inside Dentistry.
2009;5(7):44-49.
2. Romano R, ed in chief; Bichacho N, Touati B, eds. The Art of the Smile: Integrating Prosthodontics, Orthodontics, Periodontics, Dental Technology, and Plastic Surgery in Esthetic Dental Treatment. 1st ed. Hanover Park, IL: Quintessence Publishing; 2005.
3. Fradeani M. Anterior maxillary aesthetics utilizing all-ceramic restorations. Pract Periodontics Aesthet Dent. 1995;7(7):53-66.
4. Fradeani M, Bottachiari RS, Tracey T, et al. The restoration of functional occlusion and esthetics. Int J Periodontics Restorative Dent. 1992;12(1):63-71.
5. Paolucci B. Visagismo: A Arte de Personalizar o Desenho do Sorriso. São Paulo, Brazil: VM Cultural; 2011.
6. Spear FM, Kokich VG, Mathews DP. Interdisciplinary management of anterior dental esthetics. J Am Dent Assoc. 2006;137(2):160-169.
7. Sarver DM, Ackerman MB. Dynamic smile visualization and quantification: Part 2. Smile analysis and treatment strategies. Am J Orthod Dentofacial Orthop. 2003;124(2):116-127.
8. Ackerman JL, Ackerman MB, Brensinger CM, Landis JR. A morphometric analysis of the posed smile. Clin Orthod Res. 1998;1(1):2-11.
9. Vig RG, Brundo GC. The kinetics of anterior tooth display. J Prosthet Dent. 1978;39(5):502-504.
10. Kokich V. Esthetics and anterior tooth position: an orthodontic perspective. Part II: Vertical position. J Esthet Dent. 1993;5(4):174-178.
11. Arnett GW, Bergman RT. Facial keys to orthodontic diagnosis and treatment planning. Part I. Am J Orthod Dentofacial Orthop. 1993;103(4):299-312.
12. Kokich V. Esthetics and anterior tooth position: an orthodontic perspective. Part III: Mediolateral relationships. J Esthet Dent. 1993;5(5):200-207.
13. Kurth JR, Kokich VG. Open gingival embrasures after orthodontic treatment in adults: prevalence and etiology. Am J Orthod Dentofacial Orthop. 2001;120(2):116-123.
14. Hochman MN, Chu SJ, Tarnow DP. Maxillary anterior papilla display during smiling: a clinical study of the interdental smile line. Int J Periodontics Restorative Dent. 2012;32(4):375-383.
15. Cardoso JA, Almeida PJ, Fischer A, Phaxay SL. Clinical decisions for anterior restorations: the concept of restorative volume. J Esthet Restor Dent. 2012;24(6):367-383.
16. Dietschi D, Devigus A. Prefabricated composite veneers: historical perspectives, indications and clinical application. Eur J Esthet Dent. 2011;6(2):178-187.
17. Dietschi D. Optimizing smile composition and esthetics with resin composites and other conservative esthetic procedures. Eur J Esthet Dent. 2008;3(1):14-29.
18. Nahsan FP, Mondelli RF, Franco EB, et al. Clinical strategies for esthetic excellence in anterior tooth restorations: understanding color and composite resin selection. J Appl Oral Sci. 2012;20(2):151-156.
19. Dietschi D. Layering concepts in anterior composite restorations. J Adhes Dent. 2001;3(1):71-80.
20. Land CH. Porcelain dental art: No. II. Dent Cosmos. 1903;45:615-620.
21. Petridis HP, Zekeridou A, Malliari M, et al. Survival of ceramic veneers made of different materials after a minimum follow-up period of five years: a systematic review and meta-analysis. Eur J Esthet Dent. 2012;7(2):138-152.
22. Gurel G, Sesma N, Calamita MA, et al. Influence of enamel preservation on failure rates of porcelain laminate veneers. Int J Periodontics Restorative Dent. 2013;33(1):31-39.
23. Botelho MG, Ma X, Cheung GJ, et al. Long-term clinical evaluation of 211 two-unit cantilevered resin-bonded fixed partial dentures [published online ahead of print March 28 2014]. J Dent. doi: 10.1016/j.jdent.2014.02.004.
24. Magne P, Hanna J, Magne M. The case for moderate “guided prep” indirect porcelain veneers in the anterior dentition. The pendulum of porcelain veneer preparations: from almost no-prep to over-prep to no-prep. Eur J Esthet Dent. 2013;8(3):376-388.
25. De Andrade OS, Hirata R, Celestrino M, et al. Ultimate ceramic veneer: a laboratory-guided preparation technique for minimally invasive laminate veneers. J Calif Dent Assoc. 2012;40(6):489-494.
26. Hajtó J, Marinescu C. An esthetic challenge: isolated areas of high translucency in laminate veneers. Eur J Esthet Dent. 2012;7(3):282-294.
27. Schmitter M, Seydler BB. Minimally invasive lithium disilicate ceramic veneers fabricated using chairside CAD/CAM: a clinical report. J Prosthet Dent. 2012;107(2):71-74.
28. Sailer I, Fehér A, Filser F, et al. Five-year clinical results of zirconia frameworks for posterior fixed partial dentures. Int J Prosthodont. 2007;20(4):383-388.
29. Stober T, Bermejo JL, Rammelsberg P, Schmitter M. Enamel wear caused by monolithic zirconia crowns after 6 months of clinical use. J Oral Rehabil. 2014;41(4):314-322.
30. Zhang Y, Lee JJ, Srikanth R, Lawn BR. Edge chipping and flexural resistance of monolithic ceramics. Dent Mater. 2013;29(12):1201-1208.
31. Kim HK, Kim SH, Lee JB, et al. Effect of polishing and glazing on the color and spectral distribution of monolithic zirconia. J Adv Prosthodont. 2013;5(3):296-304.
32. Rinke S, Fischer C. Range of indications for translucent zirconia modifications: clinical and technical aspects. Quintessence Int. 2013;44(8):557-566.
33. Wang F, Takahashi H, Iwasaki N. Translucency of dental ceramics with different thicknesses. J Prosthet Dent. 2013;110(1):14-20.
34. Kim MJ, Ahn JS, Kim JH, Kim HY, Kim WC. Effects of the sintering conditions of dental zirconia ceramics on the grain size and translucency. J Adv Prosthodont. 2013;5(2):161-166.
35. Rinke S, Fischer C. Range of indications for translucent zirconia modifications: clinical and technical aspects. Quintessence Int. 2013;44(8):557-66. doi: 10.3290/j.qi.a29937.
36. Zhang Y, Kim JW. Graded zirconia glass for resistance to veneer fracture. J Dent Res. 2010;89
(10):1057-1062.
About the Authors
Richard D. Trushkowsky, DDS
Clinical Associate Professor and Associate Director
Advanced Program for International Dentists in Aesthetic Dentistry
NYU College of Dentistry
New York, New York
Private Practice
Staten Island, New York
Natalia De Rabago, DDS
Former Resident
Advanced Program for International Dentists in Aesthetic Dentistry
NYU College of Dentistry
New York, New York