You must be signed in to read the rest of this article.
Registration on CDEWorld is free. Sign up today!
Forgot your password? Click Here!
In 2004, the Centers for Disease Control and Prevention (CDC) Division for Heart and Stroke Prevention, the American Heart Association (AHA), and the American Stroke Association (ASA) issued Recommendation for the Establishment of Stroke Systems of Care. It advanced the idea that, “A stroke system should ensure that all patients having signs or symptoms of stroke be transported to the nearest primary stroke center or hospital with an equivalent designation, given the available acute therapeutic interventions.” In 2008, CDC, the National Association of Chronic Disease Directors, and the University of Georgia collected information on stroke policy among the states and the District of Columbia. Via a four-step process in conjunction with The Joint Commission, in July 2010, 14 primary stroke centers were designated and accredited as Advanced Certified Comprehensive Stroke Centers. Simply stated, the policy requires EMS to transport a suspected stroke patient to the nearest certified stroke center or hospital in the area.1
A cerebral vascular accident (CVA) or stroke is a brain attack. A blood clot consists of red blood cells, platelets, fibrin, and white blood cells. It is responsible for an abrupt deprivation of blood flow that rapidly suffocates, deteriorates, and impairs cranial nerves, cranial arteries, and tissue. Most strokes are in the distribution of the Circle of Willis.2 The best image is found in a computed tomography (CT) scan without contrast. CVAs are diagnosed according to the nature of the event.3 Insufficient blood flow is an ischemic stroke. Some are due to an embolic (traveling) clot or thrombotic (inside the vessel wall) clot. It leaves an area of damage called an ischemic penumbra.4 The temporary blockage of blood flow is a transient ischemic attack (TIA). The symptoms can last less than 15 minutes and resolve within 3 hours. Overall, the attack is less than 24 hours. It can be a warning sign of an impending ischemic stroke. Expeditious medical intervention helps resolve some injury and increase survival rate. A ruptured vessel wall is indicative of a hemorrhagic stroke. Leakage into the brain tissue is an intracerebral hemorrhage. Bleeding into the subarachnoid space is a subarachnoid hemorrhage. Both intercerebral and subarachnoid hemorrhage have a poor prognosis, and over 50% of patients who suffer them die soon after the event.5
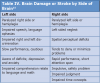
Statistically, 87% of all strokes are ischemic, 10% are intracerebral and 3% are subarachnoid.5 Time is of the essence when managing strokes (Table I).6
A stroke can happen to anyone, anytime and anywhere. Infants in the womb, newborns, children, and adults can be stroke survivors. Perinatal strokes or acute ischemic strokes (AIS) present around the 20th week of fetal life and 28 days after birth. Ninety percent of infants who suffer AIS experience seizures as the presenting feature. Perinatal AIS is 10 times more frequent than childhood strokes and is second to ischemic strokes in the elderly. Risk factors are underlying disease and infection. For example, postvaricella arteriopathy is a virus that travels from the trigeminal ganglion to the trigeminal nerve along to the cerebral arteries. Left-sided infective endocarditis, atrial or ventricular septal defect with pulmonary hypertension, iron deficiency anemia, low hemoglobin, and most cardiac diseases result in AIS.7
Moyamoya disease and syndrome, named for a Japanese term meaning “puff of smoke,” is seen as deep collateral vessels in an angiography of the head. It narrows the internal carotid artery, decreases blood flow to the brain, and forces stenosis of the anterior cerebral artery, middle cerebral artery, basilar artery, and posterior cerebral artery. Throughout childhood, most patients with Moyamoya experience AIS and TIAs. Later, in early adulthood, many succumb to intracranial hemorrhage. This syndrome is associated with Down syndrome, neurofibromatosis, Williams syndrome,96 and sickle cell disease (SCD).8 The leading cause of death in SCD is AIS between 2 and 9 years of age.7 Risk factors for adults are diabetes mellitus, obesity, smoking, sedentary lifestyle, atrial fibrillation, hypertension, high cholesterol, alcoholism, and previous CVA history. Elevated inflammatory markers of periodontal disease are also a risk factor for stroke. Periodontal pathogens contribute to the infection process, including increased C-reactive protein as well as interleukin 6, associated with the cytokine theory of periodontal disease and Porphyromonas gingivalis, as in the autoimmune theory of periodontal disease. The Oral Infections and Vascular Disease Epidemiology study found a relationship between chronic periodontitis and internal carotid artery plaque.9
AHA encourages communities nationwide to be educated and proficient in the use of FAST — an acronym for face, arms, speech, and time (Table II).10 First, observe the face for asymmetry, drooling and pooling of saliva, facial droop, or any type of contortion. Ask the person to smile. Second, request the person to raise both arms. If one or both extremities falls, drifts, or cannot be raised, this is a sign of a stroke. Third, speech reflects the person’s effort to communicate and enunciate. Ask the person to say their name or repeat a simple sentence. Listen for mumbled, slurred, hesitant, incoherent sounds, or futile attempts to form words. Fourth is time, and it is vitally important. Call 911 immediately. Meanwhile, mark the specific hour and minute the victim was last witnessed free of symptoms. It is the most significant information to know, remember and convey to emergency personnel. It is referred to as “last known normal.”11 Recording this time is imperative, as it will affect protocols, plans, and interventions. The stroke team has a window of only 3 hours from the onset of stroke symptoms to initiate life-saving procedures and medication. The competition is time, and time is brain.6
In the field, emergency personnel use various scales to assess injury and response in a stroke victim. For example, The Cincinnati Prehospital Stroke Scale (CPSS), National Institute of Health Stroke Scale (NIHSS) in conjunction with the Glasgow Coma Scale, designate quantitative values determining the degree of consciousness and level of orientation.12 Upon the patient’s arrival at the emergency department, healthcare workers put into motion the National Institute of Neurological Disorders and Strokes (NINDS) Algorithm for suspected stroke patients, along with the National Institute of Health (NIH) Golden Hour of Acute Ischemic Stroke Treatment for suspected ischemic stroke patients. Door-to-treatment time is 60 minutes. Time goals are divided into six milestones (Table III).13
If radiological report is positive for a hemorrhagic stroke, neurosurgery and or appropriate transfer to the neurology intensive care unit is started. Within the algorithm, the Glasgow Coma Score and Dysphagia Screening are performed to assess risk of secretion and fluid aspiration. Ongoing and time sequence labs are drawn. Depending on the diagnosis, the NIHSS is performed every 15 minutes, every 4 hours or every shift to help monitor cranial nerve innervations and arterial flow changes. Meticulous documentation is mandatory. The level of orientation, cooperation, ability to follow simple verbal commands, facial symmetry, tongue deviation, soft palate asymmetry, physical resistance, and drift of extremities are individually remarked.
Current research is developing an advanced formula to extend the window of infusion by 1 hour.14 A detrimental side effect of tPA is airway obstruction caused by angioedema. A hemorrhagic stroke may need an emergent craniotomy to reduce intracranial pressure. If the bleed is 1 week or more old, air-powered burr holes or trephination are drilled into the dura to drain the blood. Each procedure carries a medical benefit and surgical risk. Frank discussions and detailed explanations are vital.
Although the patient progresses out of ICU, neuro checks, physical therapy, occupational therapy, and NIHSS continue. The patient is prescribed statin, anticoagulant, and antiarrythmic medications as an inpatient and continued as a home regimen. The comparison of admission NIHSS to discharge NIHSS helps track patient progress. The discharge order may recommend a rehabilitation transfer prior to returning home or to an appropriate living accommodation. Follow-up appointments with the primary care physician and the neurologist are critical to monitor lab values and adjust drug dosages.
Dental hygienists are important professionals in the prevention of strokes. Taking the time to learn and understand the various diagnoses, risks, benefits, and protocols plus the relationship to chronic periodontal inflammation makes everyone safe. Managing care with an interdisciplinary approach establishes a feeling of confidence. It demonstrates excellent comprehensive medical and dental care.
Please read the basics of stroke education provided by ASA. Discuss the risk factors, demonstrate the FAST acronym, and explain the purpose of stroke centers or hospitals with dental patients. A majority are excited to share in the conversation. Some have personal experience in the FAST method. Many are well-versed in the signs and symptoms. All are grateful for the chance to share the information. ASA provides free pamphlets including a kitchen magnet demonstrating the FAST quick test. Dental patients visit the dentist and dental hygienist more often in one year alone than the physician and nurse. It is our opportunity to make a positive impact in the community regarding the prevention of strokes.
References
1. U.S. Centers for Disease Control and Prevention. A summary of Primary Stroke Center Policy in the United States. Available at: www.cdc.gov.
2. Vollmar TM. Personal interview.
3. Mohr JP, Wolf PA, Grotta JC, et al. Stroke Pathophysiology, Diagnosis and Management. 5th ed. Philadelphia, PA: Elsevier; 2011:49, 945-970.
4. Meoded A, Poretti A, Benson JE, et al. Evaluation of the ischemic penumbra focusing on the venous drainage: the role of susceptibility weighted imaging (SWI) in pediatric ischemic cerebral stroke. J Neuroradiol. (in press).
5. Fillit HM, Rockwood K, Woodhouse K. Brocklehurst’s Textbook Of Geriatric Medicine And Gerontology. 7th ed. Philadelphia, PA: Saunders; 2010:484-497.
6. Saver JL. Time is brain — quantified. Stroke. 2006;37(1):263-266.
7. Freundlich CL, Cerventes-Arslanian AM, Dorfman DH. Pediatric stroke. Emerg Med Clin North Am. 2012;30(3):805-828.
8. Smith JL. Understanding and treating moyamoya disease in children. Neurosurg Focus. 2009;26(4):E4.
9. Sfyroeras GS, Roussas N, Saleptsis VG, et al. Association between periodontal disease and stroke. J Vascular Surg. 2012;55(4):1178-1184.
10. American Heart Association American Stroke Association. Stroke warning sign and symptoms. Available at: www.strokeassociation.org.
11. National Institute of Neurological Disorders and Strokes. NIH revolutionizes stroke clinical research. Dec. 12, 2013. Available at: www.nih.gov/news/health/dec2013/ninds-12.htm.
12. American Association of Neuroscience Nurses. Guide to the care of the hospitalized patient with ischemic stroke, 2nd ed. Glenview, Ill.: AANN; 2008.
13. Iqbal A. The golden hour treatment of acute ischemic stroke. Med Health. 2011;84(12):378-9.
14. Parsons M, Spratt A, Campbell B, et al. A randomized trial of tenecteplase versus alteplase for acute ischemic stroke. N Engl J Med. 2012;366(12):1099-1107.
15. Lewis SL, Heitkemper MM, Dirksen SR. Medical-Surgical Nursing Assessment and Management of Clinical Problems. 6th ed. St. Louis, MO: Mosby; 2004:1525-1548.
About the Author
Mary Christine Seyer Signorino, BSDH, BSN, is a graduate of University of Missouri Kansas City School of Dentistry Dental Hygiene Department and Saint Louis University School of Nursing. Currently employed by D. Douglas Miley, DMD, MSD, program director, Saint Louis University Center for Advanced Dental Education Periodontal Department and Missouri Baptist Medical Center Neurology and Nephrology Unit.